E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 47(6); 2013 > Article
-
Original Article
Diagnostic Accuracy of Cerebrospinal Fluid (CSF) Cytology in Metastatic Tumors: An Analysis of Consecutive CSF Samples - Yoon Sung Bae1, June-Won Cheong2, Won Seok Chang3,4, Sewha Kim1, Eun Ji Oh1, Se Hoon Kim1
-
Korean Journal of Pathology 2013;47(6):563-568.
DOI: https://doi.org/10.4132/KoreanJPathol.2013.47.6.563
Published online: December 24, 2013
1Department of Pathology, Yonsei University College of Medicine, Seoul, Korea.
2Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea.
3Department of Neurosurgery, Yonsei University College of Medicine, Seoul, Korea.
4Brain Research Institute, Yonsei University College of Medicine, Seoul, Korea.
- Corresponding Author: Se Hoon Kim, M.D. Department of Pathology, Yonsei University College of Medicine, 50 Yonsei-ro, Seodaemun-gu, Seoul 120-752, Korea. Tel: +82-2-2228-1769, Fax: +82-2-362-0860, 'paxco@yuhs.ac'
• Received: August 22, 2013 • Revised: October 23, 2013 • Accepted: October 24, 2013
© 2013 The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Background
- Cerebrospinal fluid (CSF) examination can be used to verify the presence of primary malignancies as well as cases of central nervous system (CNS) metastasis. Because of its importance, there have been several studies concerning the sensitivity of CSF cytology. To determine the practical use and reproducibility of diagnoses based on CSF cytology, we evaluated this test by analyzing cytology results from consecutive CSF samples.
-
Methods
- Between July 2010 and June 2013, 385 CSF cytology samples from 42 patients were collected. The samples were gathered using a ventricular catheter and reservoir. CSF cytology of all patients was examined more than two times with immunocytochemistry for cytokeratin.
-
Results
- Primary neoplastic sites and histologic types of patients' metastatic cancer were diverse. The overall sensitivity for detecting malignancy was 41.3%. Even within short-term intervals, diagnoses frequently changed.
-
Conclusions
- Our results were inconsistent, with low sensitivity, when compared to the results of previous studies. However, CSF evaluation can still provide valuable diagnostic and prognostic information because adjuvant treatments are now routinely performed in patients with CNS metastasis. Negative CSF cytology results should not be ignored, and continuous CSF follow-up is essential for following the clinical course of patients with metastatic cancer involving the CNS.
- Patient selection
- Between July 2010 and June 2013, 385 CSF cytology samples were collected from 42 patients with the presence of a metastatic tumor confirmed by at least two histologic or cytological studies. Cytology samples obtained before adjuvant therapies were excluded to evaluate the diagnostic rate of CSF cytology more consistently. The breakdown of the patient population was as follows: 25 males and 17 females, with a median age of 55 years (range, 29 to 77 years). The mean observation period was 5 months (range, 1 to 22 months), and the mean number of CSF examinations was 9 (range, 2 to 34).
- Cerebrospinal fluid specimen collection and cytology slide preparation
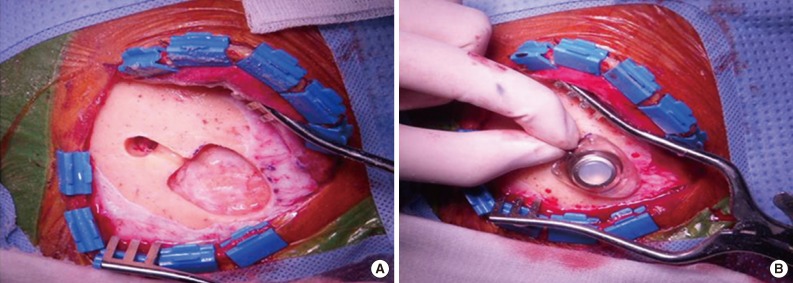
- All patients underwent an operation for the placement of a ventricular catheter and reservoir as well as consecutive CSF collections using the reservoir (Fig. 1). To minimize dry artifacts and prevent cell degeneration, samples were delivered to the Department of Pathology immediately upon collection. Samples were then processed using liquid-based cytology (LBC) (ThinPrep, Cytyc Co., Boxborough, MA, USA), an automated method of preparation and smearing of cells in a monolayer. Slides were stained and evaluated with the Papanicolaou staining method. Of the 385 CSF samples, 54 were processed by a conventional smear method rather than the liquid-based method because those samples were obtained when the liquid-based method was not available for CSF cytology.
- Immunocytochemistry
- Immunocytochemistry (ICC) was performed using a Ventana XT automated stainer (Ventana Co., Tucson, AZ, USA) with an antibody to cytokeratin (1:300, AE1/AE3, Dako, Carpinteria, CA, USA). Slides were incubated with primary antibody for 32 minutes at 37℃ followed by a universal secondary antibody for 8 minutes at 37℃. Slides were incubated in streptavidin-horseradish peroxidase D for 16 minutes at 37℃, and then the substrate, 3,3'-diaminobenzidine tetrahydrochloride (DAB) H2O2, was added for 8 minutes, followed by hematoxylin and bluing reagent counterstains at 37℃.
- Interpretation criteria
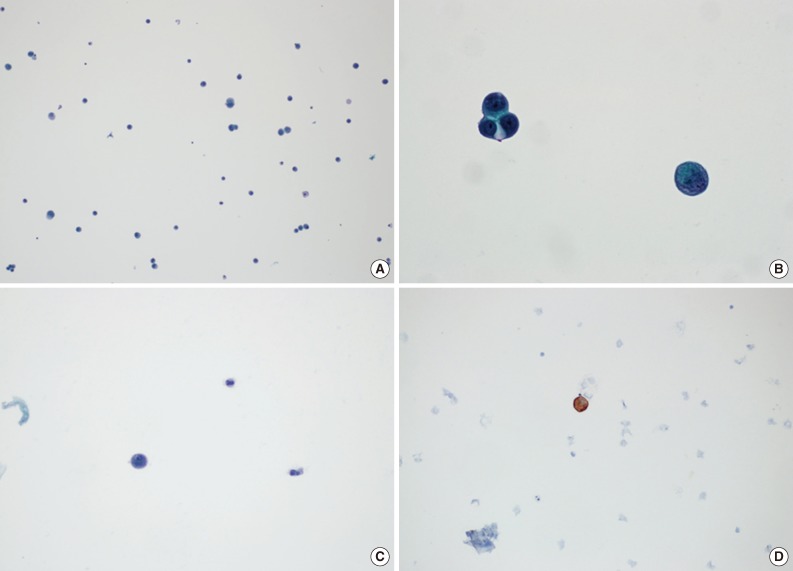
- Cases without atypical cells suggestive of metastasis were diagnosed as negative for malignancy. A positive diagnosis of malignancy was defined as the presence of atypical cells with cytokeratin immunoreactivity, regardless of the amount (Fig. 2). There were some cases that presented with atypical cells on Papanicolaou-stained slides, but it was not possible to evaluate many of these cases using cytokeratin ICC slides because the cells disappeared during the staining process. In those cases, we termed the diagnosis suspicious for malignancy, and these cases were regarded as positive findings when calculating the diagnostic rates. All slides, including those for ICC, were independently reviewed by two pathologists (S.H.K and Y.S.B).
MATERIALS AND METHODS
- As summarized in Table 1, primary malignancy sites were diverse. Lung was the most common primary site with 22 cases, followed by breast with 6 cases. The histologic types of primary malignancies are shown in Table 1. Of the 385 specimens, 132 were diagnosed as positive for malignancy and 27 were suspicious for malignancy, for a total of 159 specimens considered to have a positive diagnosis of malignancy. Among the 42 patients, 3 were never diagnosed as malignant by cytology examination even though all were confirmed to have CNS metastasis on brain tissue biopsy. Eight patients were consistently diagnosed as positive for malignancy in serial CSF evaluations. The positive malignancy diagnosis rates in the other 31 patients ranged from 4.5% to 87.5%, and the mean positive rate was 41.3%.
- Table 2 demonstrates two representative cases (case nos. 4 and 12) from our series. During a period of two months, these two patients underwent 13 and 15 CSF cytology examinations, which yielded positive results in 6 and 10 of the tests, respectively. The intervals between CSF cytology examinations ranged from 0 to 13 days and were short enough to enable more meticulous analysis of consecutive diagnostic rates. However, the results appeared random, without a consistent trend. Even within the same day, the diagnoses made from two specimens were different.
RESULTS
- Rapid transport is important for optimal cellular preservation in CSF materials, which can be cytolysed quickly. In order to reduce the number of nondiagnostic cases, CSF materials should be examined as soon as possible after collection. From a routine diagnostic viewpoint, degeneration is one of the most problematic artifacts when diagnosing cytology slides, as CSF specimens tend to degenerate more readily than other cytology specimens. These artifacts can affect the diagnostic accuracy and reduce specimen adequacy. We were able to control artificial factors by reminding clinicians of the importance of rapid processing and encouraging them to submit the samples immediately.
- Most previous studies concerning the diagnostic rates of CSF examination used the lumbar puncture as a diagnosing modality.4-6 However, lumbar puncture can be harmful to patients and difficult for clinicians because it is an invasive procedure. It is this for reason that most previous studies regarding the diagnostic accuracy of CSF performed only one CSF examination per patient. In this study, however, consecutive CSF sampling was performed using the ventricular catheter and reservoir from each patient. Although a neurosurgical procedure is required to implant a ventricular catheter in patients, it enables the continuous collection of CSF and consecutive analysis.
- LBC is now a widely used method for preparing cytology samples and has achieved broad acceptance for most cytology specimens.8-11 Furthermore, for the diagnosis of metastatic tumors in CSF, thin-layer LBC has been suggested as an appropriate diagnostic method.12,13 As in immunohistochemistry, ICC improves the diagnostic rates because cytology is often difficult and problematic to evaluate using cellular morphology alone.14 Using LBC is more convenient for performing ICC than conventional smear techniques, and the diagnostic efficacy of ICC on smears processed by thin-layer LBC has been previously validated.15-17
- Up to the present time, there have been several reports regarding the diagnostic accuracy of CSF cytology in patients with CNS metastasis. Wasserstrom et al.5 reported a sensitivity of 54.4% in initial examination and 91.1% in subsequent examination. Gondos and King6 also reported a sensitivity of 53.3%. Even though we used implanted ventricular catheters when obtaining CSF and LBC when preparing CSF slides, results of our study showed much lower diagnostic rates than previous studies. The discrepancy between results of previous studies and ours might be due to the different process of gathering CSF; unlike previous studies, we tried to evaluate the diagnostic rates of CSF cytology using consecutive examination of CSF samples from each patient. Moreover, in our study, samples were obtained from patients receiving adjuvant treatments such as chemotherapy and radiation therapy, which may have affected the diagnostic rates of CSF analysis. From the viewpoint of daily practice, our results may be more practical and accurate because most patients with CNS metastasis are now managed with ancillary treatments.7
- We could not analyze the results of CSF examinations with statistics of sensitivity or specificity because not all cytology specimens had a concordant tissue biopsy. In other words, the negative findings could not be directly considered as false negatives because we could not completely exclude the possibility that the negative findings resulted from true tumor regression due to adjuvant therapies. However, as shown in Table 2, results were distributed unevenly although all examinations were performed within very short intervals, even within the same day in some cases. Therefore, we suggest that the negative findings are not the results of tumor regression but false negative results. If so, the value of 41.3% can be regarded as sensitivity of CSF cytology in patients being treated with adjuvant therapies due to CNS metastasis.
- Several possible explanations exist for the negative results. First, several factors influencing the quality of CSF cytology specimens should be investigated. In our study, cytology specimens from positive cases were more cellular than those from negative cases. However, this cannot be the reason for the negative results because CSF is physiologically acellular. The volume of the submitted specimen can affect the diagnostic accuracy, but unfortunately this aspect was not evaluable because the amount of fluid was not promptly recorded. Dry artifact is one of the most important factors in determining the quality of CSF slides. As mentioned earlier, we could maintain the quality of CSF cytology by notifying clinicians of the importance of rapid transport. However, specimen transport could not be controlled precisely and evenly because the specimens were transported by different clinicians with different time intervals. There was no significant difference among negative results when grouped according to the sites of primary tumors (data not shown). Taken together, the negative results should be regarded as a multifactorial phenomenon without a specific reason.
- Temporary CSF cytology examinations are no longer sufficient for estimating clinical course because chemotherapy and optional radiotherapy are generally standard treatment modalities in patients with CNS metastasis. Although the total number of cases included was not remarkable, this study is noteworthy in that we tried to evaluate the diagnostic rates of CSF cytology in a novel way. By analyzing consecutive CSF samples obtained within short-term intervals, we were able to evaluate the diagnostic rates of CSF examination more precisely and more practically. Although the sensitivity of CSF cytology as a diagnostic tool in patients with CNS metastasis was lower than expected, even with the ICC, we consider this result to be important and instructive as negative results should not be ignored or regarded as tumor regression. Alternatively, continuous follow-up using CSF cytology is essential for determining clinical course, and the results must be interpreted in conjunction with clinical and radiological findings.
DISCUSSION
Acknowledgments
Acknowledgments
- 1. Savage NM, Crosby JH, Reid-Nicholson MD. The cytologic findings in choroid plexus carcinoma: report of a case with differential diagnosis. Diagn Cytopathol 2012; 40: 1–6. PMID: 22180231. ArticlePubMed
- 2. Aboulafia DM, Taylor LP, Crane RD, Yon JL, Rudolph RH. Carcinomatous meningitis complicating cervical cancer: a clinicopathologic study and literature review. Gynecol Oncol 1996; 60: 313–318. PMID: 8631558. ArticlePubMed
- 3. Glosová L, Dundr P, Effler J, Růzicková M. Gallbladder carcinoma cells in cerebrospinal fluid as the first manifestation of a tumor: a case report. Acta Cytol 2003; 47: 1087–1090. PMID: 14674086. ArticlePubMed
- 4. Glass JP, Melamed M, Chernik NL, Posner JB. Malignant cells in cerebrospinal fluid (CSF): the meaning of a positive CSF cytology. Neurology 1979; 29: 1369–1375. PMID: 573381. ArticlePubMed
- 5. Wasserstrom WR, Glass JP, Posner JB. Diagnosis and treatment of leptomeningeal metastases from solid tumors: experience with 90 patients. Cancer 1982; 49: 759–772. PMID: 6895713. ArticlePubMed
- 6. Gondos B, King EB. Cerebrospinal fluid cytology: diagnostic accuracy and comparison of different techniques. Acta Cytol 1976; 20: 542–547. PMID: 186997. PubMed
- 7. Chowdhary S, Chamberlain M. Leptomeningeal metastases: current concepts and management guidelines. J Natl Compr Canc Netw 2005; 3: 693–703. PMID: 16194457. ArticlePubMed
- 8. Scurry JP, Duggan MA. Thin layer compared to direct smear in thyroid fine needle aspiration. Cytopathology 2000; 11: 104–115. PMID: 10772010. ArticlePubMed
- 9. Frost AR, Sidawy MK, Ferfelli M, et al. Utility of thin-layer preparations in thyroid fine-needle aspiration: diagnostic accuracy, cytomorphology, and optimal sample preparation. Cancer 1998; 84: 17–25. PMID: 9500648. ArticlePubMed
- 10. Linder J. Recent advances in thin-layer cytology. Diagn Cytopathol 1998; 18: 24–32. PMID: 9451555. ArticlePubMed
- 11. Leung CS, Chiu B, Bell V. Comparison of ThinPrep and conventional preparations: nongynecologic cytology evaluation. Diagn Cytopathol 1997; 16: 368–371. PMID: 9143834. ArticlePubMed
- 12. Argon A, Uyaroğlu MA, Nart D, Veral A, Kitapçıoğlu G. The effectiveness of the liquid-based preparation method in cerebrospinal fluid cytology. Acta Cytol 2013; 57: 266–270. PMID: 23636078. ArticlePubMed
- 13. Sioutopoulou DO, Kampas LI, Gerasimidou D, et al. Diagnosis of metastatic tumors in cerebrospinal fluid samples using thin-layer cytology. Acta Cytol 2008; 52: 304–308. PMID: 18540294. ArticlePubMed
- 14. Schinstine M, Filie AC, Wilson W, Stetler-Stevenson M, Abati A. Detection of malignant hematopoietic cells in cerebral spinal fluid previously diagnosed as atypical or suspicious. Cancer 2006; 108: 157–162. PMID: 16649227. ArticlePubMed
- 15. Fadda G, Rossi ED, Mulè A, Miraglia A, Vecchio FM, Capelli A. Diagnostic efficacy of immunocytochemistry on fine needle aspiration biopsies processed by thin-layer cytology. Acta Cytol 2006; 50: 129–135. PMID: 16610678. ArticlePubMed
- 16. Dabbs DJ, Abendroth CS, Grenko RT, Wang X, Radcliffe GE. Immunocytochemistry on the Thinprep processor. Diagn Cytopathol 1997; 17: 388–392. PMID: 9360054. ArticlePubMed
- 17. Leung SW, Bédard YC. Immunocytochemical staining on ThinPrep processed smears. Mod Pathol 1996; 9: 304–306. PMID: 8685232. PubMed
References
Fig. 1Operation for ventricular catheter and reservoir placement. A localized area of the skull is removed (A), and the reservoir is placed in the defect area (B).
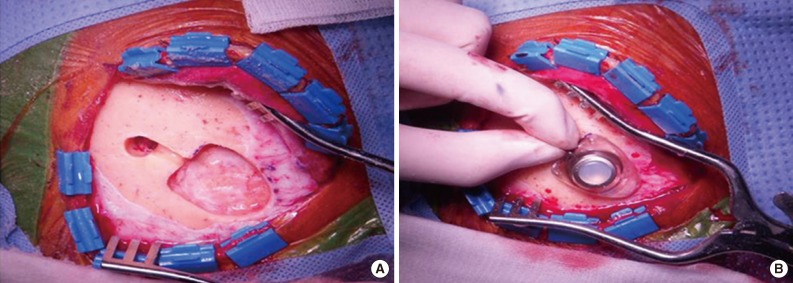
Fig. 2Low (A) and high (B) power views of cerebrospinal fluid in a patient with metastatic adenocarcinoma of the lung. Separate case showing an atypical cell (C) confirmed as metastatic carcinoma using immunocytochemistry for cytokeratin (D).
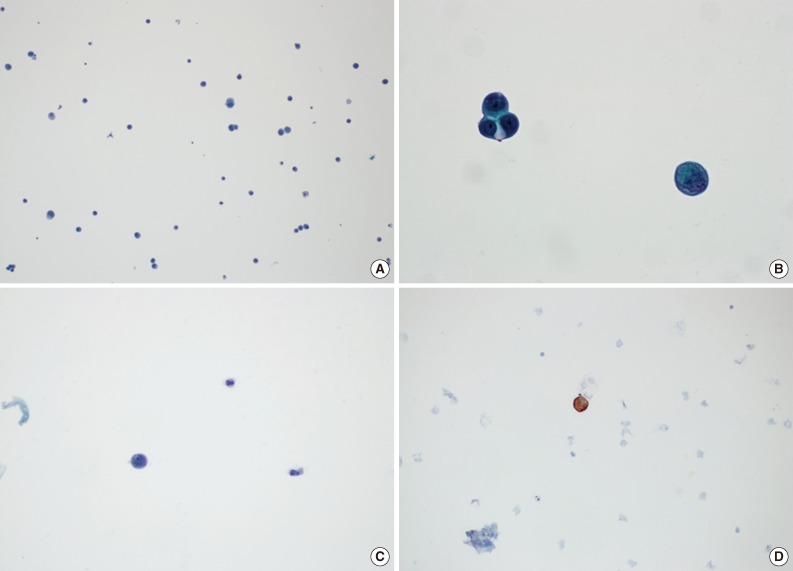
Table 1.Clinicopathologic features of 42 cases and diagnostic rates of cerebrospinal fluid cytology
Table 2.Consecutive cerebrospinal fluid cytology results of case no. 4 and case no. 12
Figure & Data
References
Citations
Citations to this article as recorded by 
- Numb cheek syndrome in breast cancer: a case report
Zhibin Tan, Si Ying Tan
Frontiers in Oncology.2024;[Epub] CrossRef - Body fluids: Comparison of liquid based cytology with conventional cytopreparatory technique
ShyamH Nemade, MeherbanoM Kamal
Indian Journal of Pathology and Microbiology.2023; 66(1): 75. CrossRef - Standardizing a volume benchmark for cerebrospinal fluids for optimal diagnostic accuracy
David Kim, Susan A. Alperstein, Momin T. Siddiqui
Diagnostic Cytopathology.2021; 49(2): 258. CrossRef - Evaluating Infectious, Neoplastic, Immunological, and Degenerative Diseases of the Central Nervous System with Cerebrospinal Fluid-Based Next-Generation Sequencing
Konstantinos I. Tsamis, Hercules Sakkas, Alexandros Giannakis, Han Suk Ryu, Constantina Gartzonika, Ilias P. Nikas
Molecular Diagnosis & Therapy.2021; 25(2): 207. CrossRef - Imaging of Intraspinal Tumors
Luke N. Ledbetter, John D. Leever
Radiologic Clinics of North America.2019; 57(2): 341. CrossRef - Isolated leptomeningeal carcinomatosis and possible fungal meningitis as late sequelae of oesophageal adenocarcinoma
Richard Dumbill, Sanja Thompson, Heiko Peschl, GDH Turner, Charles Woodrow
BMJ Case Reports.2019; 12(11): e230117. CrossRef - Cytomorphological and immunocytochemical examinations of cerebrospinal fluid in primary and metastatic brain lesions
M. V. Savostikova, L. Ya. Fomina, E. S. Fedoseeva, E. Yu. Furminskaya
Onkologiya. Zhurnal imeni P.A.Gertsena.2018; 7(1): 28. CrossRef - Metastatic Breast Carcinoma in Cerebrospinal Fluid: A Cytopathological Review of 15 Cases
Rema Rao, Syed A. Hoda, Alan Marcus, Rana S. Hoda
The Breast Journal.2017; 23(4): 456. CrossRef - Clinicocytological analysis of cases with positive cerebrospinal fluid in our hospital
Nozomi IWAMOTO, Mitsuaki ISHIDA, Akiko KAGOTANI, Nozomi KASUGA, Muneo IWAI, Yuji HAYASHI, Namie ARITA, Yoshimitsu MIYAHIRA, Ryoji KUSHIMA
The Journal of the Japanese Society of Clinical Cytology.2016; 55(5): 291. CrossRef
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-