E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 48(1); 2014 > Article
-
Case Study
Primary Sigmoid Adenocarcinoma Metastasis to the Breast in a 28-Year-Old Female: A Case Study and a Review of Literature - Amna Ahmad, Kweku Baiden-Amissah, Adegoke Oyegade, Mohammed Absar1, Kate Swainson2, Sami Titi
-
Korean Journal of Pathology 2014;48(1):58-61.
DOI: https://doi.org/10.4132/KoreanJPathol.2014.48.1.58
Published online: February 25, 2014
Department of Cellular Pathology, Pennine Acute Hospitals NHS Trust, Royal Oldham Hospital, Oldham, UK.
1Breast Unit, Pennine Acute Hospitals NHS Trust, North Manchester General Hospital, Manchester, UK.
2Department of Radiology, Pennine Acute Hospitals NHS Trust, North Manchester General Hospital, Manchester, UK.
- Corresponding Author: Amna Ahmad, M.B.B.S. Specialty Training Registrar, Royal Oldham Hospital, Rochdale Rd, Oldham, OL1 2JH, UK. Tel: +44-7947567907, Fax: +44-1616278745, 'amnahamid@doctors.org.uk'
• Received: May 15, 2012 • Revised: August 4, 2012 • Accepted: August 7, 2012
© 2014 The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
- Metastasis to the breast from colorectal carcinoma is rare, only a few cases have been reported in the literature, and no cases have been reported in a young, 28-year-old patient. This report confirms the occurrence of the disease in a younger age group. The patient was referred to the Breast Clinic with a history of a gradually increasing lump in her right breast for two weeks' duration. On clinical examination, a 2-cm firm lump was noted in the upper inner quadrant of the right breast, which was clinically benign; however, histological examination of the breast core biopsy together with immunohistochemistry confirmed metastatic colorectal adenocarcinoma. The primary colorectal carcinoma was later confirmed to be a stage pT4N2M1 tumor, and the Duke stage was C1. Histology with immunohistochemistry is very important in the diagnosis of cases of this nature, but the clinical correlation should be taken into consideration at multidisciplinary team meetings to decide the final management of the patient.
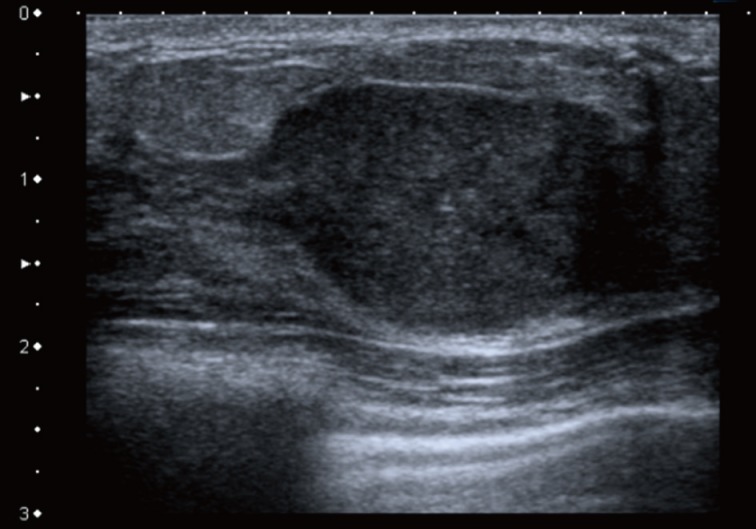
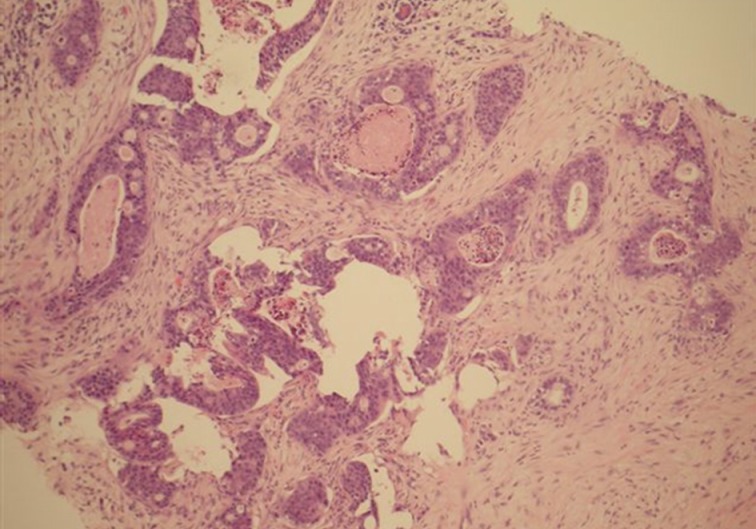
- A 28-year-old Caucasian female presented to her general practitioner after she noticed a lump in her right breast for two weeks' duration. It was gradually increasing in size with no pain or nipple discharge. She had no previous breast problems or family history of breast cancer. On examination, a 2-cm firm lump was noted in the upper inner quadrant of her right breast, which was clinically benign. No lymph nodes were palpable. The ultrasound examination demonstrated a hypoechoic solid area with some calcification, consistent with a benign lesion (Fig. 1). A mammogram showed a partially well-defined nodule with intermediate type microcalcifications, which suggested suspicious morphology corresponding to the site of the primary carcinoma. Fine needle aspiration cytology showed low-grade atypia of probable benign nature set in a background of numerous polymorphs. Core biopsies were taken, and the histological examination revealed a malignant tumor made of cells showing prominent nuclear pleomorphism, significant mitotic activity, glandular structures with epithelial stratification, and focal cribriform formations. Some of the glands were dilated and contained necrotic debris within the lumen, or 'comedo-like necrosis.' These findings were consistent with a well to moderately differentiated adenocarcinoma (Fig. 2).
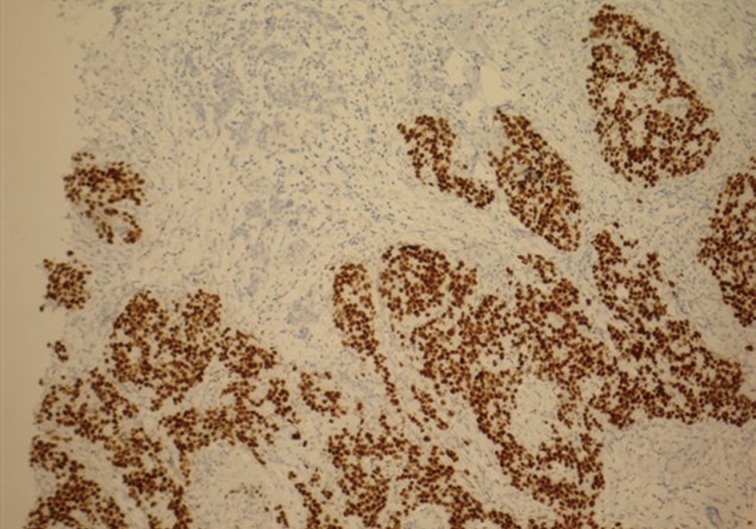
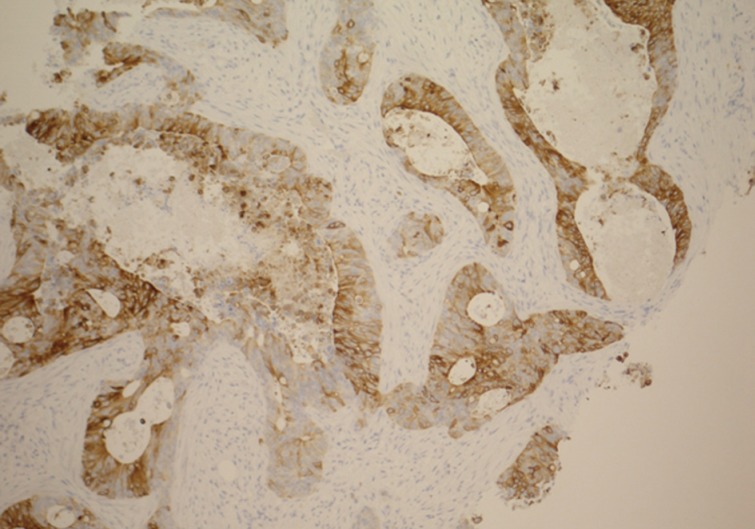
- The main differential diagnosis included primary breast ductal carcinoma of nonspecific type and metastatic adenocarcinoma from other primary sites, including the colon, lung, upper gastrointestinal tract, hepato-pancreatobiliary sites, endometrium, and ovary. An immunohistochemical profile was performed, and the tumor was found to be strongly positive for CDX2 (Fig. 3) and cytokeratin (CK) 20 (Fig. 4). CK5/6 (myoepithelial marker) showed a patchy reaction, which suggested partial maintenance of the myoepithelial cells, findings that can mimic ductal carcinoma in situ (DCIS) of comedo type. The tumor cells were negative for CK7 (Fig. 5), HER2, gross cystic disease fluid protein 15, estrogen receptor, and progesterone receptor. The abovementioned immunoprofile confirmed the diagnosis of metastatic adenocarcinoma from a colorectal primary source. These findings excluded other primary tumors from the breast, lung, stomach, esophagus, endometrium, and ovary, which are usually positive for CK7 and negative for CK20 and CDX2. A detailed review of previous medical records was carried out and revealed that only ten days before presenting to the Breast Clinic, the patient underwent an urgent colonoscopy after she complained of severe weight loss, poor appetite, and diarrhea with blood and mucous. There was no family history of any bowel cancers. In addition, computed tomography scan exhibited a 3.6-cm metastatic deposit in the liver and a mass lesion in the recto-sigmoid junction with no evidence of lung deposits or enlarged lymph nodes. Histology of the colonic biopsies showed a moderately differentiated adenocarcinoma. This finding helped to reach a final diagnosis of metastatic adenocarcinoma to the breast from a primary sigmoid tumor.
- Treatment options for the patient were discussed at several multidisciplinary team (MDT) meetings, including breast, colorectal, and hepatobillary MDT meetings. The patient underwent anterior resection of the rectum. The primary lesion was revealed to be a perforated adenocarcinoma, with advanced clinical disease of pT4N2M1 and Dukes C1. The patient subsequently received chemotherapy; however, the breast and hepatic lesions were not removed due to the multi-focality nature of the disease.
CASE REPORT
- Rectal carcinomas are very uncommon in a younger age group.2 To our knowledge, there is not a single case report of a secondary breast metastasis from simultaneous primary rectal cancer in a 28-year-old patient. The incidence of concurrent primary colorectal cancer with secondary breast metastasis is very low, with only three cases reported so far.4 These cancers usually occur more commonly in an older age group, generally presenting at a very late stage and as such are associated with a poor prognosis. The peak age incidence is reported to be in the fifth decade (median age, 54.3 years; range, 32 to 86 years).4
- The occurrence of breast metastases from extramammary sites is 0.5% to 6%. Such tumors are even rarer from colonic adenocarcinomas with just 19 cases reported in the literature.2 The incidence is 6.6% to 7% in autopsy studies.2 The majority of these malignancies occur in women: only 5% to 8% occur in men.5
- Recent medical and surgical interventions have improved the survival rate in colorectal carcinoma. Distant metastasis is usually associated with either recurrent or advanced disease,6 and the most common sites for metastasis are local lymph nodes, the liver, and lungs.7
- Secondary breast neoplasms are difficult to identify. They present as palpable, discrete, rapidly growing small nodules, most commonly in the upper outer quadrant of the breast.6,8 On mammogram, they have specific features and can mimic benign lesions. Their appearance ranges from well to poorly circumscribed lesions that are not associated with microcalcifications.5,9 In our case, microcalcification was seen within the lesion.
- It is important to distinguish primary from metastatic breast disease in order to offer the patient appropriate treatment. An ultrasound-guided core needle biopsy of the lesion is the standard of care for establishing an accurate diagnosis, and hence full clinical details at the time of histology examination are paramount.10 The differentiation between primary breast carcinoma and colorectal metastatic adenocarcinoma can be difficult on routine hematoxylin and eosin staining. On the other hand, the presence of an unusual pattern of tumor morphology, which can be quite different from primary breast carcinoma, and an absence of in situ ductal carcinoma in the surrounding breast indicates a metastatic lesion. Back-to-back glands along with a cribriform-like formation may occur in colorectal adenocarcinoma, but such lesions usually show epithelial stratification, higher cellular atypia, mitotic activity, and polymorphs within the lumen. A cribriform breast carcinoma usually has low-grade cellular pleomorphism and insignificant mitotic activity. Intestinal type mucosa with goblet cells is a helpful feature, but unfortunately this was not seen in our case. The impression of a 'foreign type' tumor, which is not seen in day-to-day practice, should raise suspicions of metastasis. Immunohistochemical studies help establish the histological type as well as the tumor origin. In our case, the final diagnosis was achieved by using a small panel of immunohistochemistry. The majority of primary breast cancers are CK7 positive and CK20 negative, whereas metastatic colonic adenocarcinomas are CK7 negative and CK20 positive.11 The strong nuclear positivity with CDX2 is highly sensitive and specific for colonic cancers.12 In addition, estrogen and progesterone receptors are usually negative in metastatic breast cancers. A patchy reaction for CK5/6 and comedo-like necrosis can mimic DCIS, as was described in our case. Careful examination of tumor histomorphology features such as epithelial stratification, high nuclear atypia, significant mitotic activity, and positive reactions for CK20 and CDX2 can help to overcome this difficulty.
- Metastatic carcinomas in the breast are associated with a poor prognosis with a survival rate of less than 12 months from the time of breast tumor diagnosis.5,13 Patient management is complex and depends upon multiple factors, including extent of the primary tumor, lymph node status, distant metastasis, age, and other comorbidities. Proper clinical correlation and immunohistochemistry helps to reach the final correct diagnosis in the majority of cases. These tools play a vital part in patient management and can help avoid unnecessary mastectomies. With limited treatment options available, surgical resection of the primary lesion with chemotherapy at an early stage can improve the prognosis.
DISCUSSION
Acknowledgments
Acknowledgments
- 1. Mihai R, Christie-Brown J, Bristol J. Breast metastases from colorectal carcinoma. Breast 2004; 13: 155–158. PMID: 15019699. ArticlePubMed
- 2. Sanchez LD, Chelliah T, Meisher I, Niranjan S. Rare case of breast tumor secondary to rectal adenocarcinoma. South Med J 2008; 101: 1062–1064. PMID: 18791504. ArticlePubMed
- 3. Bhirangi KS, Pinto DJ, Crosbie JJ. Solitary breast metastasis from carcinoma of colon. Ulster Med J 1997; 66: 138–139. PMID: 9414946. PubMedPMC
- 4. Shackelford RE, Allam-Nandyala P, Bui MM, Kiluk JV, Esposito NN. Primary colorectal adenocarcinoma metastatic to the breast: case report and review of nineteen cases. Case Rep Med 2011; 2011: 738413PMID: 21738536. ArticlePubMedPMCPDF
- 5. Ho YY, Lee WK. Metastasis to the breast from an adenocarcinoma of the colon. J Clin Ultrasound 2009; 37: 239–241. PMID: 18461602. ArticlePubMed
- 6. Lal RL, Joffe JK. Rectal carcinoma metastatic to the breast. Clin Oncol (R Coll Radiol) 1999; 11: 422–423. PMID: 10663337. ArticlePubMed
- 7. Singh T, Premalatha CS, Satheesh CT, et al. Rectal carcinoma metastasizing to the breast: a case report and review of literature. J Cancer Res Ther 2009; 5: 321–323. PMID: 20160374. ArticlePubMed
- 8. Fernández de Bobadilla L, García Villanueva A, Collado M, et al. Breast metastasis of primary colon cancer. Rev Esp Enferm Dig 2004; 96: 415–419. PMID: 15230671. ArticlePubMed
- 9. van Rossen ME, Westenend PJ, Plaisier PW. Response to "Breast metastases from colorectal carcinoma" by R. Mihai et al. The Breast 2004; 13, 155-8. Breast 2005; 14: 80–81. PMID: 15695089. ArticlePubMed
- 10. Selcukbiricik F, Tural D, Bay A, Sahingoz G, Ilvan S, Mandel NM. A malignant mass in the breast is not always breast cancer. Case Rep Oncol 2011; 4: 521–525. PMID: 22125523. ArticlePubMedPMC
- 11. Noh KT, Oh B, Sung SH, et al. Metastasis to the breast from colonic adenocarcinoma. J Korean Surg Soc 2011; 81(Suppl 1):S43–S46. PMID: 22319737. ArticlePubMedPMC
- 12. Cabibi D, Cipolla C, Valerio MR, Ingrao S. Metastatic seeding of colon adenocarcinoma manifesting as synchronous breast and chest wall localization: report of a case. Surg Today 2011; 41: 242–246. PMID: 21264761. ArticlePubMed
- 13. Perin T, Canzonieri V, Memeo L, Massarut S. Breast metastasis of primary colon cancer with micrometastasis in the axillary sentinel node: a metastasis that metastasized? Diagn Pathol 2011; 6: 45PMID: 21619688. ArticlePubMedPMC
References
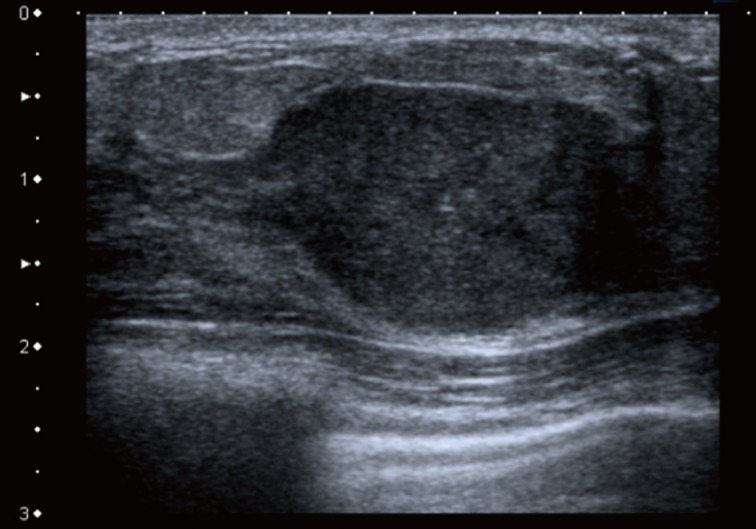
Fig. 2Breast core biopsy of the adenocarcinoma shows marked nuclear atypia, significant mitotic activity, cribriform formation and comedo-like necrosis within dilated glandular structures.
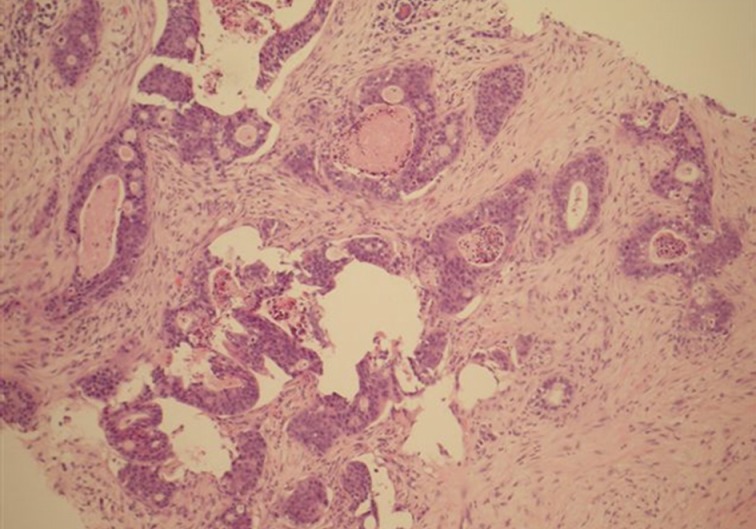
Fig. 3Breast core biopsy shows colorectal metastatic adenocarcinoma with diffuse positive nuclear staining for CDX2.
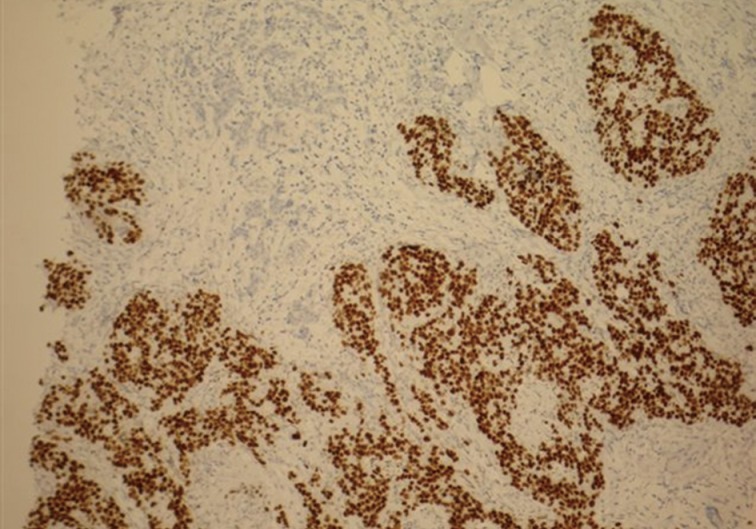
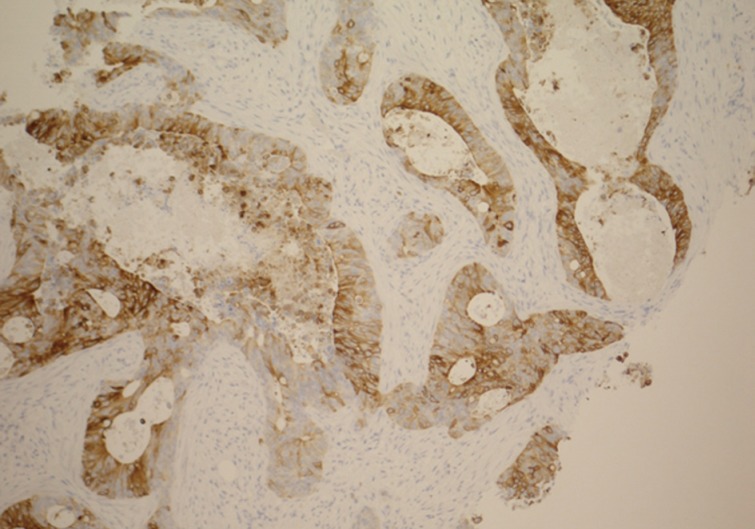
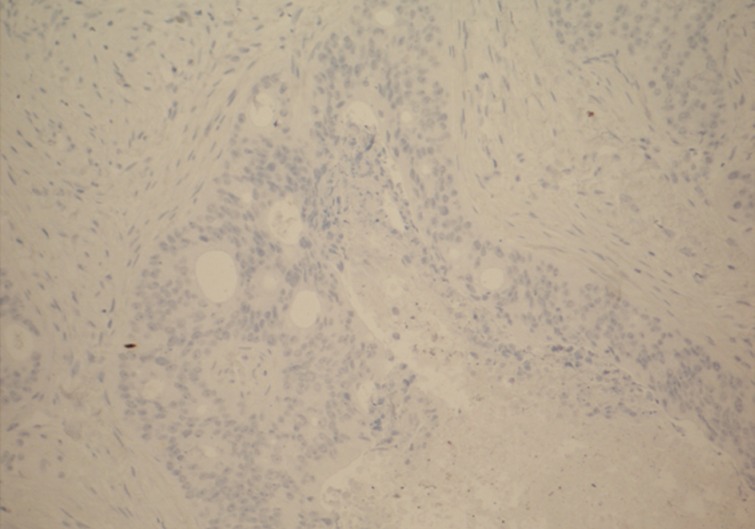
Figure & Data
References
Citations
Citations to this article as recorded by 
- Breast mass as the first sign of metastasis from rectal carcinoma: a case report and review of the literature
Jiawei Xu, Chao Liu, Chengdong Yu, Tenghua Yu, Fan Fan, Xiaofang Zhang, Chuansheng Huang, Wen Chen, Zhengkui Sun, Meng Zhou
Frontiers in Oncology.2023;[Epub] CrossRef - A case report of multiple bilateral breast metastases after colorectal cancer
Khaled Arnaout, Nouran Hawa, Sarab Agha, Lama Kadoura, Marwa Aloulou, Kusay Ayoub
International Journal of Surgery Case Reports.2021; 81: 105759. CrossRef - Metastatic Breast Signet-Ring Cell Carcinoma from a Colonic Primary: Review of a Rare Case Report
Ghazaleh Shaker, Hayedeh Haeri, Behnaz Jahanbin
International Journal of Cancer Management.2021;[Epub] CrossRef - Breast metastasis from rectal cancer with BRAF V600E mutation: a case report with a review of the literature
Hiroko Hasegawa, Yoko Nagata, Yuko Sakakibara, Masakazu Miyake, Kiyoshi Mori, Norikazu Masuda, Masayuki Mano, Shoichi Nakazuru, Hisashi Ishida, Eiji Mita
Clinical Journal of Gastroenterology.2020; 13(2): 153. CrossRef - Colonic mucinous adenocarcinoma with secondary in the breast: A case report and literature review
Ameera Balhareth, Abdullah A. AlQatari, Fozan Aldulaijan, Amani Joudeh
International Journal of Surgery Case Reports.2020; 76: 364. CrossRef - Breast metastasis from colorectal cancer treated by multimodal therapy
Tien-Chan Hsieh, Chao-Wen Hsu
Medicine.2019; 98(51): e18016. CrossRef - A case series of metastases to the breast from extramammary malignancies
Tanvi Vaidya, Subhash Ramani, Ashita Rastogi
Indian Journal of Radiology and Imaging.2018; 28(04): 470. CrossRef - Metástasis mamaria de un adenocarcinoma mucinoso de colon: descripción de un caso y revisión de la literatura
Marta Seoane Vigo, María Berdeal Díaz, Lourdes Galán Raposo, Fabio Ares Farpón, Alejandro García Varona, Luis González Crespo
Revista de Senología y Patología Mamaria.2017; 30(1): 28. CrossRef - Metastases of transverse colon cancer to bilateral ovaries (Krukenberg tumor) and the left breast: A case report
Xin-Yu Luo, Jue Wang, Jia Zhao, Rui Chen, Xiao-Ming Zha
Oncology Letters.2017; 14(1): 31. CrossRef - Metastasis of rectal signet ring adenocarcinoma to the breast in a young woman after 10 years, a rare case report and review of the literature
Bita Geramizadeh, Ali Mohammad Bananzadeh, Mohammad Reza Sasani, Asieh Khorshidi, Mahsa Marzban
Cancer Treatment Communications.2016; 7: 58. CrossRef - Metastatic Colonic Adenocarcinoma in Breast: Report of Two Cases and Review of the Literature
Jiten P. Kothadia, Rezina Arju, Monica Kaminski, Arvind Ankireddypalli, Sushil Duddempudi, Jonathan Chow, Shah Giashuddin
Case Reports in Oncological Medicine.2015; 2015: 1. CrossRef
 PubReader
PubReader Cite this Article
Cite this Article