Melanotic Oncocytic Metaplasia of the Nasopharynx: A Report of Three Cases and Review of the Literature
Article information
Abstract
Melanotic oncocytic metaplasia of the nasopharynx is a rare condition which is characterized by the presence of usually a small, brown to black colored pigmented lesion around the Eustachian tube opening. Although it is a benign lesion, it may be clinically misdiagnosed as malignant melanoma. Microscopically, melanotic oncocytic metaplasia is a combination of oncocytic metaplasia of the epithelium of the gland and melanin pigmentation in its cytoplasm. In our present study, we report three cases of melanotic oncocytic metaplasia of the nasopharynx. All the three cases occurred in men and were presented as multiple black pigmented lesions around the torus tubarius. Microscopically, mucous glands with diffuse oncocytic metaplasia and numerous black pigments were observed. No cellular atypia was observed. Immunohistochemically, the scattering of S-100 protein-positive, and human melanoma black 45-negative dendritic melanocytes was evident. This is the first report of cases of melanotic oncocytic metaplasia of the nasopharynx in Korea.
Melanotic oncocytic metaplasia of the nasopharynx is a rare lesion, first described by Shek et al.1 in 1995. Since then, seventeen cases have been reported in the English literature.2,3 Macroscopically, it is presented as a small brown to black colored mucosal lesion. Microscopically, the characteristic feature is the presence of glands with oncocytic metaplasia and melanin pigments in their cytoplasm. In this review, we report three additional new cases and review the current literature. To the best of our knowledge, this is the first report of cases of melanotic oncocytic metaplasia of the nasopharynx in Korea.
CASE REPORTS
Case 1
A 72-year-old man presented with a 3-month history of headache and mild hearing impairment. His family and past medical history were unremarkable except for a smoking history of 40 cigarettes per day for the past 50 years. To evaluate the symptoms, a nasoscopic examination was carried out. Nasoscopic examination revealed the presence of multiple dark blue colored mucosal lesions around the bilateral torus tubarius (Fig. 1). Clinician's impression about the lesions was that of melanotic dysplasia. The lesions were biopsied to establish the definitive diagnosis. Follow-up for three months after diagnosis was uneventful, but the lesions remained unchanged.
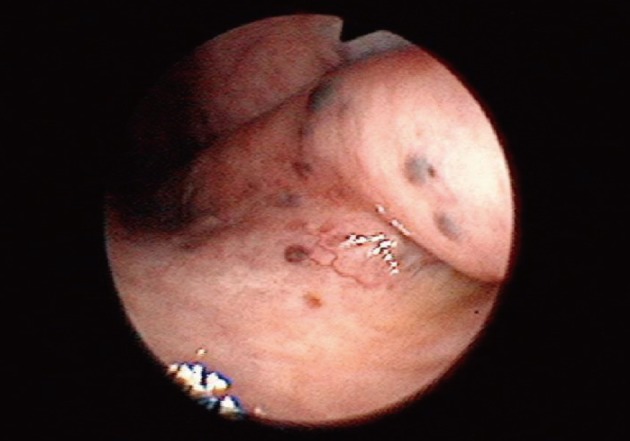
Nasoscopic appearance of melanotic oncocytic metaplasia of the nasopharynx. Multiple, dark blue colored mucosal lesions around the bilateral torus tubarius are noted.
Case 2
A 71-year-old man presented with a 1-day history of hoarseness. His past history was unremarkable but, he had a smoking history of 20 cigarettes per day for the past 40 years. Macroscopically, multiple black mucosal lesions around the left torus tubarius and soft palate were apparent. Clinician's impression of the lesion was that of a nasopharyngeal pigmented lesion. Biopsy was done for establishing the definitive diagnosis. After the biopsy, there was some relief from hoarseness, but at the six-month follow-up, the condition of the lesions remained unchanged.
Case 3
A 51-year-old man presented with a 3-month history of tongue pain. He had type C hepatitis but his other past medical history was unremarkable and smoking history was unknown. Nasoscopy was carried out and multiple, dark colored spots around the right torus tubarius were noted. Clinician's impression of the lesion was that of melanotic oncocytic metaplasia of the nasopharynx. Biopsy was performed, but the symptoms persisted. The contact with the patient was lost and hence follow-up after two months was not feasible in the third case.
The clinical information about each patient is summarized in the Table 1 below.
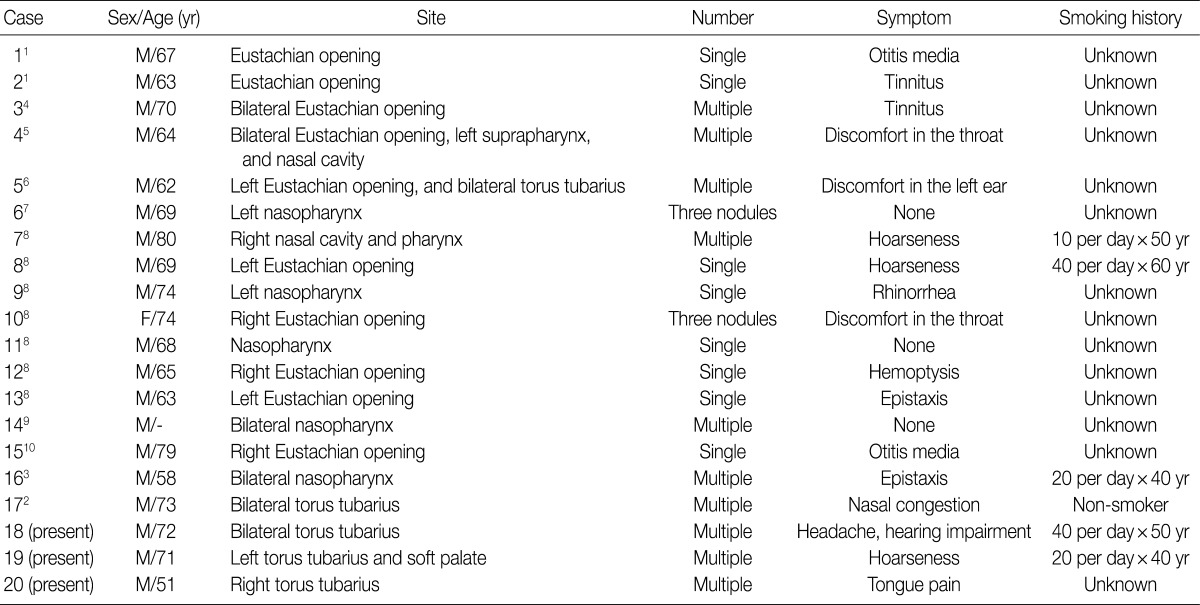
Clinical findings of cases with melanotic oncocytic metaplasia of the nasopharynx
Pathological findings
The histology of all the three cases was similar. Microscopically, the lesions were well circumscribed, but were not encapsulated. In case 1, the surface of the lesion was covered by normal respiratory epithelium. All the three lesions were composed of mucous glands with diffuse oncocytic metaplasia. Oncocytes comprised of abundant eosinophilc granular cytoplasm. Brown pigments were also observed in the cytoplasm of most of the oncocytic cells (Fig. 2). The brown pigments stained positive for Fontana-Masson staining and negative for Berlin blue staining, which were indicative of melanin pigmentation. Mitotic figures or atypia were not observed in the epithelial cells of the gland. Upon immunohistochemical study, dendritic cells in the basal layer of glands were found to be positive for S-100 protein (1:1,000, Dako, Glostrup, Denmark), but were negative for human melanoma black-45 (HMB-45; 1:200, Dako, Carpinteria, CA, USA) (Fig. 3). Based on the above findings, all the lesions were diagnosed as melanotic oncocytic metaplasia of the nasopharynx.
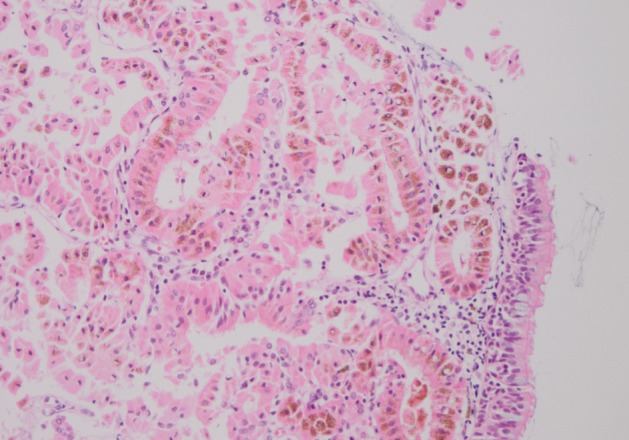
Histological findings of melanotic oncocytic metaplasia of the nasopharynx. The lesion is located in the subepithelial area and consists of mucous glands with diffuse oncocytic metaplasia and numerous brown colored melanin pigments.
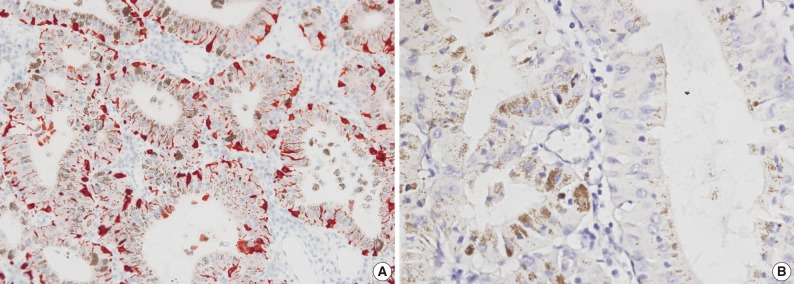
Immunohistochemical staining of melanotic oncocytic metaplasia. Dendritic melanocytes, which are positive for S-100 (A), but are negative for human melanoma black-45 (B), are interspersed among the pigmented oncocytic cells.
DISCUSSION
We have described three cases of melanotic oncocytic metaplasia of the nasopharynx. Till date, only 17 cases of melanotic oncocytic metaplasia of the nasopharynx have been reported in the English literature.1-10 Melanotic oncocytic metaplasia of the nasopharynx predominantly occurred in males (16/17), with an average age of 68 years (range, 56 to 80 years).2,3 All the patients were identified to be of Asian origin. Clinically, the diagnosis was incidental in majority of cases, but some melanotic oncocytic metaplasia of the nasopharynx may occasionally cause symptoms such as otitis media, tinnitus, hoarseness, rhinorrhea, epistaxis, discomfort of the throat, and hemoptysis. These symptoms may be due to the obstruction of the Eustachian tube opening. However, some of the symptoms were thought to be unrelated with the lesions. Macroscopically, all the lesions were a few millimeters in size, single or multiple, and brown to black in color. Bilateral lesions were also seen sometimes (6/17). Clinician's impression of the lesion ranged from a malignant tumor, such as melanoma or carcinoma, to a benign melanocytic nevus. All the reported cases pursued a benign clinical course.3 Till date, there has been no case of disease recurrence or progression in the cases. Simple excision is usually a sufficient treatment for melanotic oncocytic metaplasia of the nasopharynx.6
All our three patients were males, between fifty-one to seventy-two years of age. They complained of headache, mild hearing impairment, hoarseness, and tongue pain. All of them showed multiple black pigmented lesions around the torus tubarius, and one of them had bilateral lesions. After biopsy, symptoms such as mild hearing impairment and hoarseness disappeared in two of the three patients, but it was not clear whether the symptoms were related to the lesions. Moreover, some complaints such as headache and tongue pain remained unchanged and were considered to be unrelated with the lesions.
Histologically, melanotic oncocytic metaplasia is characterized in terms of coexistence of oncocytic metaplasia and melanin pigmentation in the same gland. Oncocytic metaplasia is most commonly encountered in certain epithelial organs such as the salivary glands, the lacrimal glands, and the thyroid glands. However, occurrence of oncocytic metaplasia in the upper respiratory tract is an uncommon finding. The origin of the melanin pigment in the oncocytic glands is still unclear. Melanocytes as a melanin source, have been reported to exist in the stroma and epithelium of the nasal cavity, paranasal sinus, and larynx.11 The melanin pigment in the oncocytic glands may be derived from the adjacent melanocytes through their dendrites.5 This hypothesis is supported by the immunohistochemical findings of our three cases. There was the presence of numerous S-100-positive, and HMB-45-negative melanocytes with dendritic processes stretching between the epithelial cells of the glands. Dong et al.12 found Platts bacilli and Cryptococcus neoformans in the nasopharyngeal secretions of patients with melanotic oncocytic metaplasia. As these two types of bacteria can produce melanin, they suggested that the nasopharynx bacteria produced melanin, which was phagocytosed by oncocytes, leading to the formation of melanin containing oncocytes.
The exact pathogenesis of melanotic oncocytic metaplasia of the nasopharynx is still unknown. However, Sakaki et al.8 postulated that this lesion could be related to the age, smoking, ethnic, and neuro-immuno-endocrine network of the subject. Moreover, in some cases, stimulation by factors such as smoking may play a role in progression of melanotic oncocytic metaplasia. Neuropeptides may cause the oncocytic metaplasia or melanocyte to proliferate and produce melanin through neuro-immuno-endocrine network. Two of our three patients had a smoking history of 40 cigarettes per day from the past 50 years and 20 cigarettes per day from the past 40 years, respectively. However, smoking history in the third patient was not studied. Therefore, in further studies, it is important to clarify the pathogenesis and histogenesis of melanotic oncocytic metaplasia of the nasopharynx.
In summary, we have described three cases of melanotic oncocytic metaplasia of the nasopharynx with review of relevant literature. Although this is a rare clinical and pathological entity, it is not so difficult for the pathologists and clinicians to make the diagnosis if they have had some experience in handling such cases. The recognition of this lesion is clinically important, since it might be misdiagnosed as a malignancy, such as malignant melanoma by the unwary.
Notes
No potential conflict of interest relevant to this article was reported.