Pigmented Perivascular Epithelioid Cell Tumor (PEComa) of the Kidney: A Case Report and Review of the Literature
Article information
Abstract
Heavily pigmented perivascular epithelioid cell tumors (PEComa) are rare, only eight cases of which have been reported. Unlike typical epithelioid angiomyolipoma, most of these tumors have been encountered in female patients without tuberous sclerosis. The long-term prognosis thereof is undetermined. Cytological similarity and heavy melanin pigment make it difficult for pigmented PEComa to be differentiated from pigmented clear cell renal cell carcinoma or malignant melanoma. The immunoprofile of tumor cells, such as human melanoma black-45 expression, as well as the absence or presence of other melanocytic or epithelial markers, are helpful in determining a differential diagnosis. Here we report a case of heavily pigmented PEComa of the right kidney and review the literature describing this tumor. In this case, the immunoprofile and clinical features corresponded well to those described in the literature. Since the prognosis of such disease has not yet been established, close follow-up of this patient was recommended.
Perivascular epithelioid cell tumors (PEComa) comprise a family of tumors including angiomyolipoma, lymphangiomyomatosis, clear cell "sugar" tumor of the lung, and other visceral and soft tissue lesions composed of distinctive perivascular epithelioid cells.1 Among these, angiomyolipomas are traditionally characterized as common mesenchymal tumors of the kidneys composed of spindle or epithelioid smooth muscle-like cells, abnormally thick-walled and hyalinized blood vessels, and adipose tissue. However, unusual cases of angiomyolipoma composed purely of epithelioid cells without adipocytes or blood vessels have been reported.2,3 Additionally, this atypical form was previously shown to be composed of epithelioid cells that distinctively reacted with human melanoma black-45 (HMB-45) monoclonal antibody along with antibodies against smooth muscle, and was described as a variant of angiomyolipoma called epithelioid angiomyolipoma. Although the World Health Organization suggested using the unifying term "PEComa" to describe these tumors, various terms such as epithelioid angiomyolipoma, clear cell epithelioid angiomyolipoma, and perivascular epithelioid clear cell tumor have been used as synonyms of PEComa in the literature. Heavily pigmented PEComa of the kidney is very rare and only a few cases have been reported.4-6 Here we report a case of heavily pigmented PEComa of the right kidney.
CASE REPORT
A 37-year-old woman was referred to our institution with a right renal mass that was incidentally found during an evaluation for hypertension. Abdominal computerized tomography revealed a well-demarcated non-enhanced cystic mass at the lower pole of the patient's right kidney (Fig. 1A). Radical nephrectomy was performed under suspicion of malignancy. The patient had no history of tuberous sclerosis and has not shown any evidence of recurrence at 12 months after surgery.
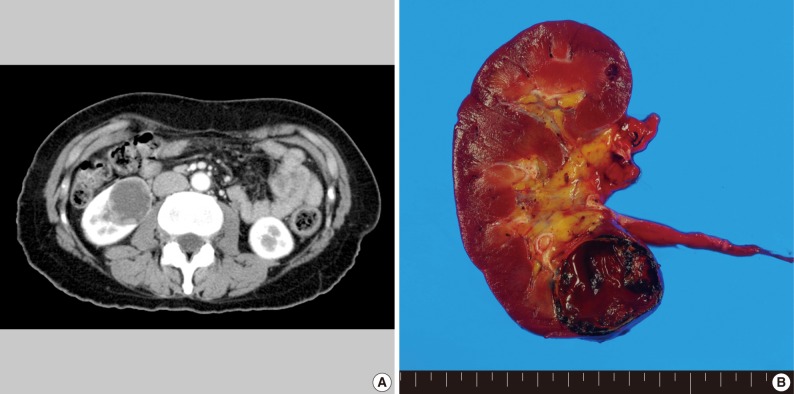
(A) Abdominal computed tomography. A well-demarcated cystic tumor, 3.5 cm in diameter, on the right kidney is noted. (B) The tumor is a black-pigmented mass with cystic change and is filled with blood clots and thick brownish fluid.
Pathologic findings
Macroscopic examination
The kidney measured 11×5.5×3.5 cm and weighed 146 g. Located in the cortex of the lower pole of the right kidney, the tumor measured 3.5 cm in size, was well-circumscribed, appeared as a black pigmented mass with cystic changes and was filled with blood clots and chocolate-like fluid (Fig. 1B).
Light microscopic examination
The tumor was well demarcated from the renal parenchyma and was partially encapsulated by a thick fibrous capsule (Fig. 2A). The solid portion of tumor was composed of sheets or nests of large polygonal tumor cells. These cells had round to oval nuclei with prominent nucleoli, and eosinophilic or clear cytoplasm. Also, they contained brown pigment in their cytoplasm, which reacted strongly with Fontana-Masson stain (Fig. 2B). Mitotic figures were rare and nuclear pleomorphism was only occasionally detected. Delicate fibrovascular septa were interspersed among the tumor cell nests.
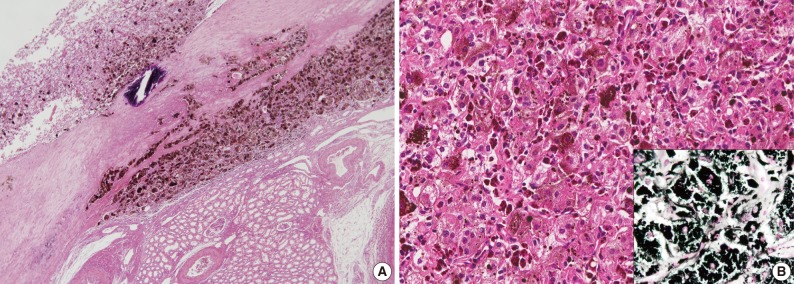
(A) The tumor is well demarcated from the renal parenchyma and partially encapsulated by a thick fibrous capsule. (B) The tumor is composed of sheets of large polygonal tumor cells with eosinophilic or clear cytoplasm. The brown pigments in the cytoplasm strongly reacts with Fontana-Masson stain (inset).
Immunohistochemical examination
The tumor cells were positive for HMB-45 (Fig. 3), but negative for other melanocytic markers (S-100 protein and melan A), cytokeratin (AE1/AE3), epithelial membrane antigen, CD10, vimentin, smooth muscle actin, CD68, c-kit and neuroendocrine markers (CD56, synaptophysin, and chromogranin). Also, the Ki-67 labeling index was low (<1%).
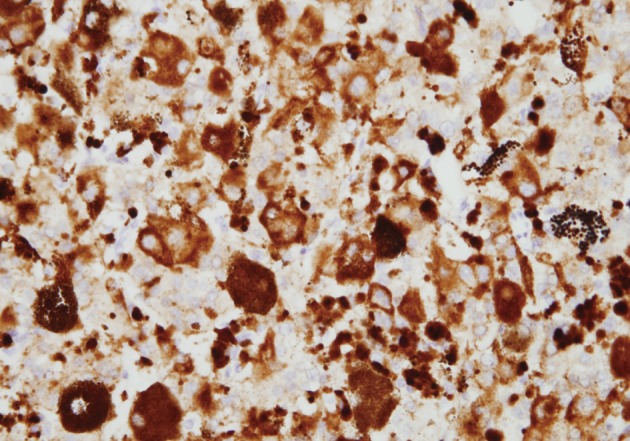
The tumor cells strongly reacted with human melanoma black-45 monoclonal antibody.
DISCUSSION
In contrast to reports of epithelioid angiomyolipoma, the black cut-surface due to heavy melanin pigmentation was a distinguishing feature in this case; the differential diagnoses considered for this case included malignant melanoma, pigmented clear cell renal cell carcinoma, and composite paraganglioma. Malignant melanoma in the kidneys is usually located in the renal pelvis and in cases of metastatic lesions, multifocal metastasis is common.7 However, our patient did not exhibit a primary lesion and the tumor was located in the cortex. In addition, the tumor cells did not express other melanocytic markers such as S-100 protein and melan A. Accordingly, the clinical features and immunoprofile did not indicate the presence of malignant melanoma. Furthermore, we were able to differentiate the PEComa in our case from pigmented clear cell renal cell carcinoma according to its immunoprofile. Conventional renal cell carcinoma distinctively expresses epithelial markers, such as cytokeratin or epithelial membrane antigen and others, CD10, and vimentin. Similar to the present case, paragangliomas are composed of sheets or nests of large polygonal cells with intervening fibrovascular septa. Moreover, this type of tumor shares many similar cytomorphological features with PEComa. However, paragangliomas express neuroendocrine markers, which were not observed in the present case.
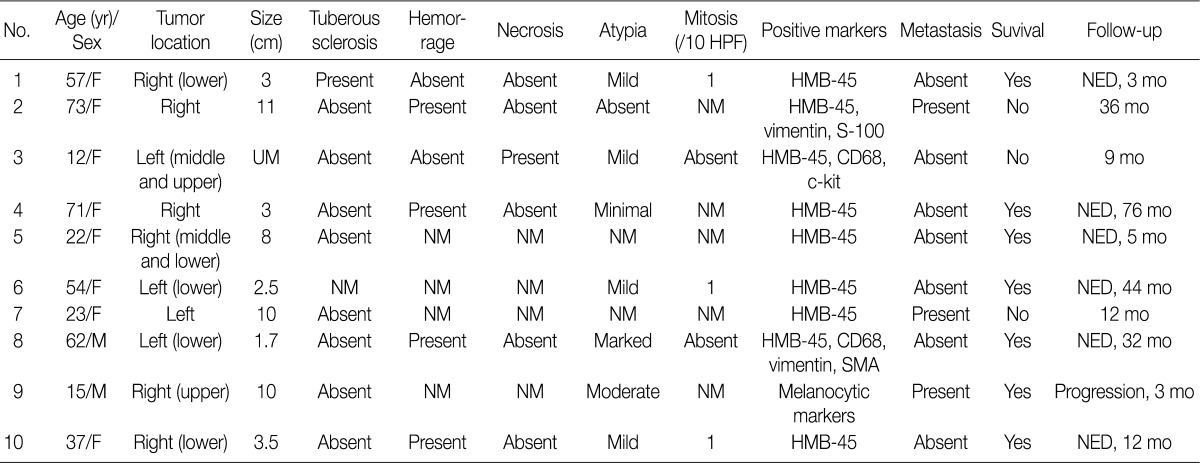
In the literature, only a few heavily pigmented PEComa of the kidney have been reported (Table 1).3-6,8-11 Interestingly, among ten reported cases, including our case, eight cases occurred in women, ranging in age from 12 to 73 years old. One of the cases that occurred in a male patient presented as a component of a triple synchronous neoplasm in one kidney, of which the other two components were clear cell and chromophobe renal cell carcinomas.12 Unlike typical epithelioid angiomyolipomas that are frequently associated with tuberous sclerosis, only one pigmented PEComa patient exhibited tuberous sclerosis.13 In the literature, tumors ranged in size from 2.5 to 11 cm. Among seven cases which the tumor was located in the kidneys, five cases were located in the lower pole of the kidneys. All of the tumors were composed of sheets of eosinophilic to clear epithelioid cells, and they distinctively exhibited immunohistochemical reaction with HMB-45. Although long-term follow-up data have not yet been established, three patients showed metastasis and three patients, including two with recurrence, died of the disease.
According to a study by Brimo et al.,14 among 40 cases of renal epithelioid angiomyolipoma, nine showed local recurrence or distant metastases and four died of the disease. Their study also devised a predictive model comprising four atypical features of epithelioid angiomyolipoma including the proportion of atypical epithelioid cells, mitotic figures, atypical mitotic figures, and necrosis.14 In the present case, mitotic figures were rare and nuclear pleomorphism was mild. Moreover, necrosis was not found.
Recently, Nese et al.15 analyzed 41 cases of pure epithelioid PEComa of the kidney, and found five adverse prognostic parameters associated with disease progression (recurrence, metastasis, or death due to the disease), which included an associated tuberous sclerosis complex or concurrent angiomyolipoma, necrosis, tumor size>7 cm, extrarenal extension and/or renal vein involvement, and carcinoma-like growth pattern characterized by large cells arranged as a cohesive nest, broad alveoli, and compartmentalized sheets separated by thin vascular-rich septae. Among them, only a carcinoma-like growth pattern and extrarenal extension and/or renal vein involvement were independent parameters associated with unfavorable outcomes.15 In this regard, the histologic findings of our case, which included sheets or nests of large polygonal tumor cells with delicate fibrovascular septa between tumor cell nests, could be characterized as demonstrating a carcinoma-like growth pattern and may suggest an increased risk of disease progression. Although the patient has not shown any evidence of recurrence at 12 months after surgery, long-term follow-up is warranted.
In summary, we report a rare case of heavily pigmented PEComa presented as a solitary mass in the kidney. When a pigmented tumor with epithelioid cytologic features is encountered in the kidney, differential diagnosis thereof should be thoughtfully undertaken, and immunohistochemical staining with HMB-45 and other melanocytic markers or epithelial markers would be helpful in differentiating PEComa from malignant melanoma or pigmented renal cell carcinoma.
Notes
No potential conflict of interest relevant to this article was reported.