Lipoma within Inverted Meckel's Diverticulum: A Case Report
Article information
Meckel's diverticulum is the remnant of the vitello-intestinal duct that persists in about 2% of the population.1,2 It is the most common congenital anomaly of the gastrointestinal tract in children.1-3 While the majority of Meckel's diverticula remain asymptomatic, there is a 4-6% rate of symptomatic complications such as bleeding in children and intestinal obstruction in adults.4 Tumors within Meckel's diverticula occur infrequently, and the incidence of benign tumors developing within Meckel's diverticula is extremely rare.1 We present a case of ileo-ileal intussusception due to a lipoma within a Meckel's diverticulum in a young adult.
CASE REPORT
A 33-year-old man presented with recurrent episodes of abdominal pain. He had experienced intermittent epigastric pain for about 10 months, which developed into pain of the entire abdomen for 3 months. The abdominal pain was not associated with any other symptoms and resolved spontaneously, so he did not seek medical attention. There was no significant past medical or family history. Laboratory findings on admission were unremarkable. Abdominal computed tomography revealed slightly dilated loops of small bowel and a hypo-dense, irregularly contoured polypoid mass in the ileum (Fig. 1). Radiological features were suggestive of intussusception. However, there was a difficulty in finding the cause of the ileo-ileal intussusception in this patient. He had no history of previous operations or malignancy and was relatively healthy. During the operation to address the intussusception, a dimple was noted in the antimesenteric ileal wall, 40 cm proximal to the ileocecal valve. Gentle reduction of the intussusception demonstrated a large polypoid mass attached to a stalk at the corresponding mucosa of the dimpled area. Segmental resection of small bowel was performed. Grossly, the resected specimen showed a large pedunculated mass (6×4×3 cm) with surface ulceration. The stalk portion was connected to adjacent mucosa. On sectioning, the mass was homogenous, soft, and yellow with some white fibrotic tissue in the stalk (Fig. 2). The preliminary gross diagnosis was a submucosal lipoma. Microscopic findings revealed that the mass consisted of mature fat cells with scattered pancreatic acinar and ductal cells in the periphery. The mucosa overlying the mass was gastric type epithelium and showed focal ulceration.
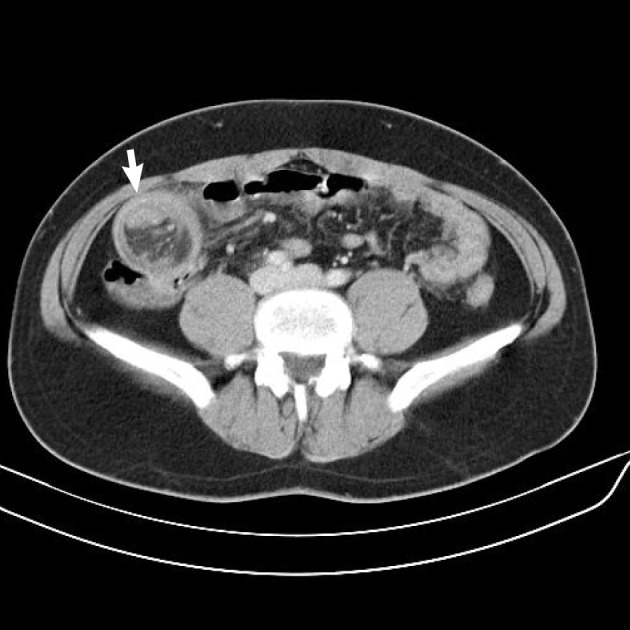
Abdominal computed tomography shows a heterogeneous target-shaped mass in the right abdomen.
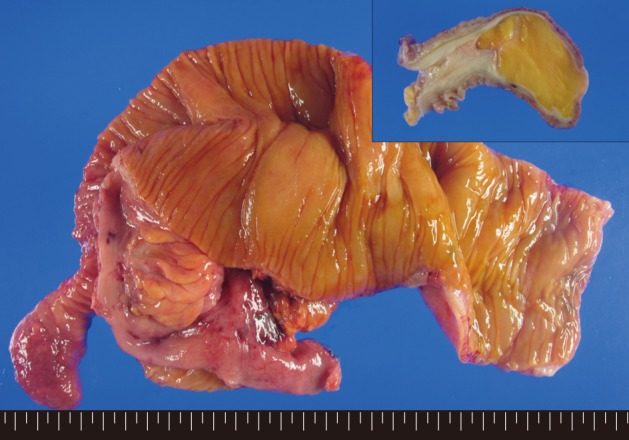
Intussuscepted portion of small bowel exposing an inverted Meckel's diverticulum (6 cm in length) is identified. The cut surface of the mass shows a relatively homogenous soft yellow mass, resembling a lipoma (inset).
The proper muscle was obliterated. The final diagnosis was a lipoma within an inverted Meckel's diverticulum (Fig. 3). The patient was discharged on postoperative day 7 without any complications.
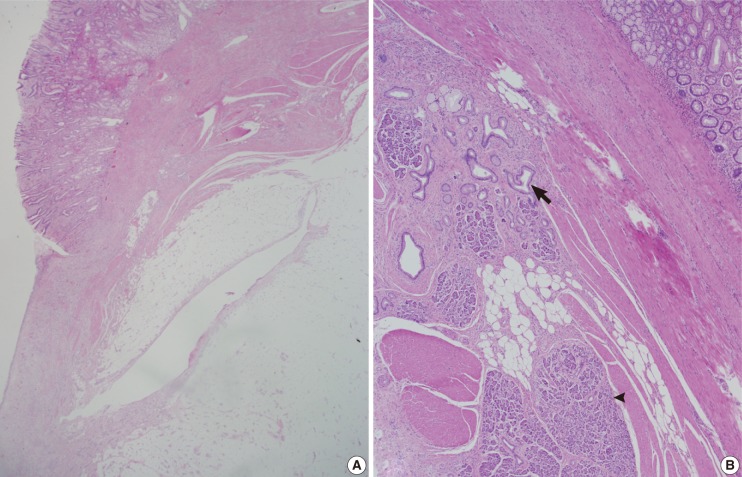
(A) The mass consists of mature fat cells, and the overlying mucosa is gastric type epithelium. (B) Scattered pancreatic acinar and ductal cells are identified among fat cells (arrowhead, acinus; arrow, duct).
DISCUSSION
Meckel's diverticulum is the most prevalent congenital abnormality of the intestinal tract among children. This anomaly is due to the incomplete obliteration of the omphalomesenteric duct during the 7th week of gestation.1,2 It is classically located 100 cm proximal to the ileocecal valve. While Meckel's diverticula remain mostly asymptomatic in affected individuals, there is a 4-6% probability of symptomatic presentation, including intestinal obstruction, intussusception, and bleeding.2 Clinical presentations are quite different between children and adults. Hemorrhage is the most common complication in children because of the presence of gastric epithelium in the diverticulum.2,3 This explains why it is most commonly found in children and why early detection of the diverticulum is possible. Intestinal obstruction is the most common complication in adults, with incidence rates varying from 22% to just over 50%. In these cases, early diagnosis is relatively difficult.3 One cause of obstruction is intussusception or inversion, with a Meckel's diverticulum acting as the lead point.3 The cause of inversion of Meckel's diverticulum has not been explained clearly. One hypothesis is that abnormal peristaltic movement derived from the ulcer or ectopic tissue may cause the diverticulum to become inverted.4 Also, if a tumor develops within a Meckel's diverticulum, the tumor component tends to press into the bowel wall or through the luminal area, which could lead to inversion of the diverticulum. In our case, the patient presented only with recurrent episodes of abdominal pain, with aggravation of the pain and no bleeding. We think this may have been due to the growing lipomatous component, which may have caused inversion of the diverticulum and finally intestinal obstruction.
Tumors occurring within a Meckel's diverticulum are rarely observed.2 Lowenfels and Maisonneuve5 reported that the risk of cancer developing within an ileum with a Meckel's diverticulum was higher than in an ileum without a Meckel's diverticulum.6 The incidence of benign tumors developing within Meckel's diverticula is extremely rare,1,2 though common histologic types are lipomas and leiomyomas.2 On review of the literature for cases with lipomas, all patients were young adults, and the presenting symptom was intestinal obstruction rather than bleeding, similar to our case.1,3,4,6 The location of the fat component within the Meckel's diverticulum was in the sub-mucosal layer.1 This finding is important to differentiate a lipoma from a pseudolipoma in an inverted Meckel's diverticulum. In some cases, invaginated mesenteric fat in an inverted Meckel's diverticulum can be misdiagnosed as a lipoma. However, identification of the subserosal location of fat cells in those cases will prevent a misdiagnosis.
The pathologic finding of an uncomplicated and typical Meckel's diverticulum is not difficult to recognize. However, pathologists should be aware of the possibility of tumor development within the Meckel's diverticulum. When this complication is found in a young adult, it may cause inversion and intestinal obstruction. Correlation of the clinical and pathologic features allow for the correct diagnosis.
Notes
No potential conflict of interest relevant to this article was reported.