Fine Needle Aspiration Cytology of Postoperative Spindle Cell Nodule in Neck after Thyroidectomy: A Case Report
Article information
Although postoperative spindle cell nodules have occasionally been found in the lower genitourinary tract,1-3 their presence in post thyroidectomy sites has been reported in only one case.4 In addition, diagnosis by fine needle aspiration (FNA) has not been established.
Here, we report on characteristic cytologic findings for a postoperative spindle cell nodule arising in the post-thyroidectomy site.
CASE REPORT
A 53-year-old female patient visited the hospital for evaluation of an asymptomatic right lateral neck mass. She had undergone a right thyroid lobectomy for treatment of a papillary microcarcinoma 22 months prior. The tumor measured 0.7×0.6 cm in size with a clear resection margin. After the operation, she was followed regularly, and there were no events.
A hypoechoic mass with multiple calcifications was observed on thyroid ultrasonography, and ultrasonography guided-FNA was performed. The smear of the FNA cytology showed fragments of fibrocollagenous connective tissue and scattered spindle cells (Fig. 1A). Some histiocyte-like cells were aggregated forming vague granulomas (Fig. 1B, C). Loosely scattered young fibroblast-like cells with plump nuclei were observed (Fig. 1D). The cytologic diagnoses were suggestive of nodular fasciitis or a granulomatous reaction to a foreign body.

Cytologic findings. (A) Fragments of fibrocollagenous tissue and scattered spindle cells and (B, C) vague granulomas are observed. (D) On high power view, spindle cells with plump nuclei and indistinctive nucleoli are observed.
The patient had undergone a complete thyroidectomy and neck mass excision. Severe adhesions were observed in the postoperative thyroid bed, and the residual thyroid left lobe was normal in appearance on gross examination.
Grossly, the neck mass measured 4.3×3.5×2.6 cm, with a round, firm, and whitish surface. The cut surface was a homogenous yellow-tan color and was focally hemorrhagic (Fig. 2A). There were no pathologic findings in the thyroid left lobe.
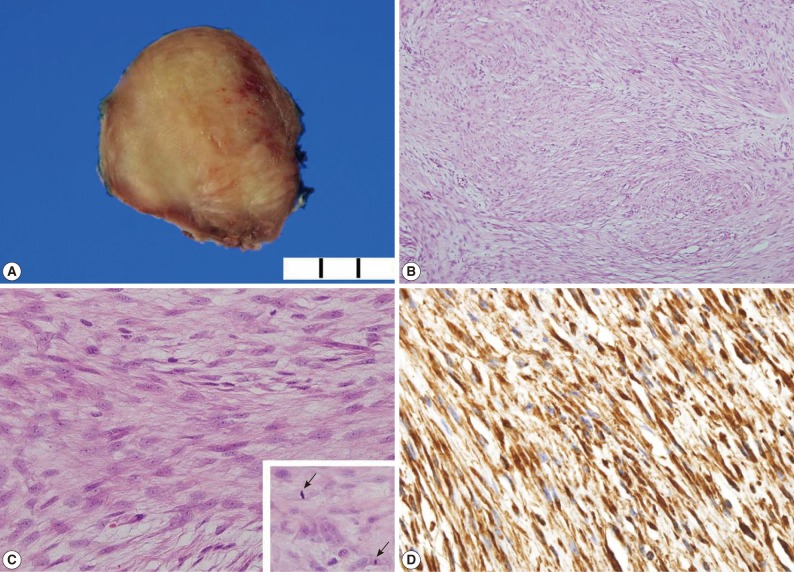
Gross and microscopic findings. (A) The cut surface of the mass is a homogenous yellow-tan color. (B) The tumor consists of a spindle cell proliferation. (C) The high power view shows homogenous bland-looking spindle cells with plump nuclei and indistinctive nucleoli (inset). Mitoses are occasionally observed (arrows). (D) Spindle cells are reactive in vimentin.
Microscopically, the mass was found to be composed of bland-looking spindle cells (Fig. 2B), with an indistinct cell border, eosinophilic cytoplasm, and oval nuclei. The nucleoli were inconspicuous (Fig. 2C). Mitotic counts were 6 per 10 high power field without atypism (Fig. 2C, inset). Adhesions on adjacent structures were observed, but did not show an infiltrative pattern.
The spindle cells were fully reactive in vimentin (prediluted, V9, Dako, Glostrup, Denmark) and focally positive for α-smooth muscle actin (prediluted, 1A4, Dako); however, they were negative for anaplastic lymphoma kinase (ALK; 1 : 50, ALK1, Dako), Cam 5.2 (prediluted, Becton Dickinson, CA, USA), desmin (prediluted, D3, Dako), epithelial membrane antigen (prediluted, E29, Dako), and pancytokeratin (prediluted, AE1/AE3, Dako) (Fig. 2D). Ki-67 labeling index was less than 5%.
DISCUSSION
Postoperative spindle cell nodules in the thyroidectomy bed are extremely rare.4 According to the literature, the reported sites of postoperative spindle cell nodule included the genitourinary tract, oral cavity, breast, and skin.1-3 Except for cases arising in the skin, all other cases have arisen in previous biopsy or operation sites,1-4 and the cases arising in the skin all had a history of trauma. In 1984, Proppe et al.1 reported eight cases of spindle cell nodules with benign features arising in the lower genitourinary tract. These lesions showed elongated spindle cells that are reactive in vimentin. The stains for muscle specific actin, smooth muscle actin, desmin, and cytokeratin were inconclusive with only some showing positivity.
There has been controversy with regard to whether lesions containing spindle cell nodules are reactive or neoplastic.2,3,5 ALK gene rearrangement and immunohistochemical positivity for ALK were found in approximately 50% of cases, suggesting that postoperative spindle cell nodules are neoplastic. However, the history of trauma or surgical treatment and the microscopic findings of high vascularity and inflammation support that the nodules are a reactive process.2 There is one report of describing trisomy 7 in postoperative spindle cell nodules.5 However, trisomy 7 is a controversial aberration, which has been found in non-neoplastic tissue as well as in a variety of neoplasms.5
Due to its high diagnostic accuracy and minimal invasiveness, FNA aspiration is widely used for evaluation of neck masses. The possible spindle cell lesions in neck include schwannoma, nodular fasciitis, fibrous tumor, and sarcoma.6 Schwannomas, which are the most common spindle cell lesion in the neck, consist of spindle cells with moderate cytoplasm and slender, wavy, pointed-end nuclei. These cells are different from postoperative spindle cell nodules. The aspiration specimens of nodular fasciitis are characteristically cellular and single scattered fibroblast-like cells with occasional multinucleated giant cells. Collagen fragments and myxoid substances can often be observed. Neutrophils, eosinophils, lymphocytes, and plasma cells are present in various proportions. However, postoperative spindle cell nodules do not show myxoid substances and inflammatory cells. Sarcomas may show cellular pleomorphism in necrotic backgrounds.6 Metastatic or recurrent cancers should be also investigated in patients with a history of malignancy. Although there is one report of a postoperative spindle cell nodule in the thyroid bed after surgery,4 no articles describing cytologic findings were found. These cytologic findings are different from those for other spindle cell lesions, and are useful for differential diagnosis.
In conclusion, awareness of postoperative spindle cell nodules as part of the patient history is helpful in making a diagnosis of spindle cell lesions by FNA.
Acknowledgments
This work was supported by the Gachon University Research Fund.
Notes
No potential conflict of interest relevant to this article was reported.