Fine Needle Aspiration Cytology of Hepatic Hydatid Cyst: A Case Study
Article information
Abstract
Hydatid cysts (echinococcosis) are caused by an infestation with larval tapeworms of the genus Echinococcus. The disease is extensively distributed worldwide, and it has been rarely reported in Korea. We describe the cytologic features of a case of hepatic hydatid cyst in a 28-year-old male. Computed tomography revealed a cystic mass in the right lobe of the liver. A right hemihepatectomy was performed. The aspirated fluid from the hepatic cystic mass was clear. The smears showed protoscolices, hooklets, and a laminated membrane.
Hydatid cyst (echinococcosis) is a parasite disease caused by the larval stage of the genus Echinococcus. The disease is endemic in sheep-raising regions, especially Mediterranean countries, the Middle East, Eastern Europe, South America, Australia, and New Zealand.1 Due to increasing migration and traveling, this disease now has a worldwide distribution. In Korea, hydatid cysts have rarely been reported in travelers or workers from endemic areas.2-4 Fine needle aspiration cytology (FNAC) of hydatid cysts has been described.5-8 However, to our knowledge, the aspiration cytologic features of hepatic hydatid cysts has not previously been reported in Korea. In this report, we described the cytologic features of hepatic hydatid cysts examined by FNAC in a 28-year-old male.
CASE REPORT
A 28-year-old man presented with abdominal pain that had persisted for the past three months. The patient was a foreign worker from Uzbekistan. Physical examination revealed no abdominal mass. He had undergone partial hepatic resection due to a hydatid cyst 14 years ago. Abdominal computed tomography scan revealed a cystic mass in the right hepatic lobe (Fig. 1). Serologic testing for hydatid cysts was not performed. However, the clinical impression was a hydatid cyst. A right hemihepatectomy was performed, and the resected specimen was sent for intraoperative consultation. FNAC of the cystic mass was performed. The aspirated fluid was clear. Both smears and a cell block preparation were carried out. The smears were stained using Papanicolaou and hematoxylin and eosin stains.
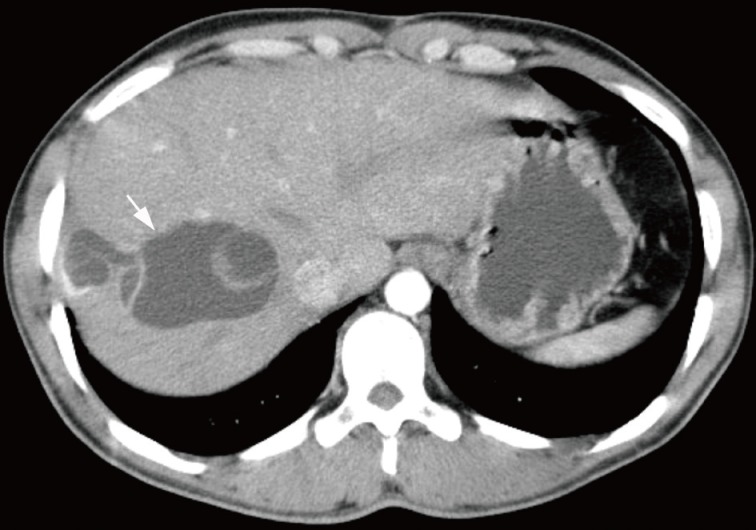
Abdomen computed tomography scan. A cystic mass with internal septation is present in the right hepatic lobe.
The smears showed many protoscolices in the shape of a mushroom, with hooklets (Fig. 2). Amorphous necrotic debris and inflammatory cells were present in the background. Degenerated protoscolices were also found. Detached hooklets with refractile structures were seen. Fragments of laminated membranes stained pinkish-red on hematoxylin-eosin stain. Therefore, the diagnosis of a hydatid cyst was made.
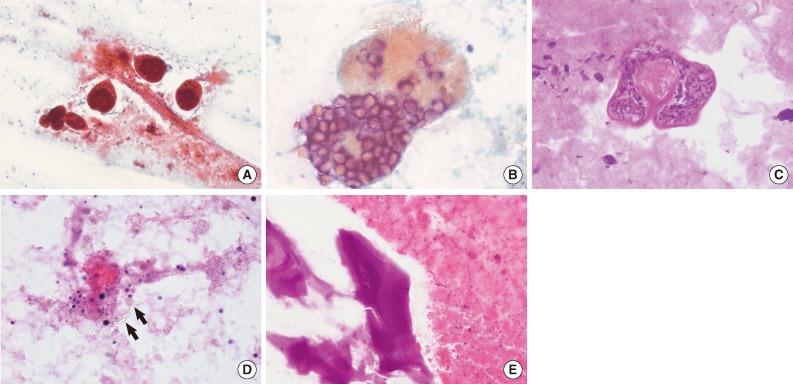
Cytologic findings. (A) There are many protoscolices in the shape of a mushroom. The necrotic debris is seen in the background. (B, C) Higher magnification of the protoscolices reveals hooklets. (D) Isolated refractile hooklets (arrows) are present. (E) Fragments of a laminated membrane are present.
On gross examination, the right hemihepatectomy specimen measured 15.3×14.8×8.5 cm in size. A 6.5×5.0×4.5 cm hepatic cyst was present (Fig. 3). The cyst contained multiple daughter cysts of variable sizes. The wall of the cyst was grayish white. Histologic examination revealed that the cyst wall was composed of an outer laminated membrane and an inner germinal layer (Fig. 4). Protoscolices and a brood capsule were seen. The laminated membrane was acellular and the germinal layer contained nuclei. The surrounding liver parenchyma showed a fibrinous wall and inflammatory cells infiltration including lymphocytes, eosinophils, and histiocytes. The patient has been alive for 16 months following this surgery without evidence of recurrence.
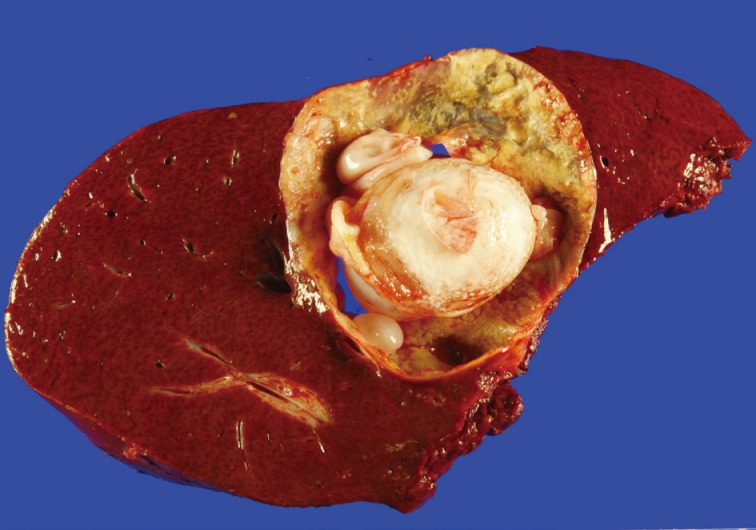
Gross finding. The hepatic cyst contains multiple daughter cysts.
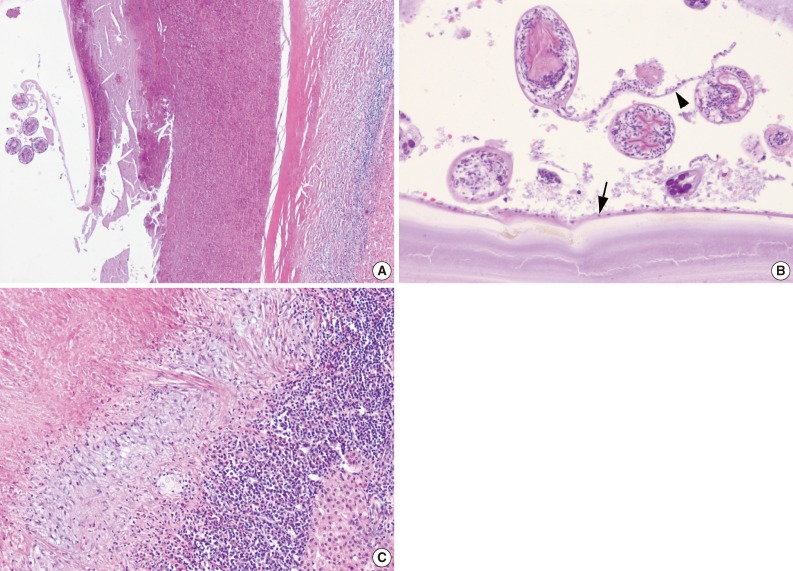
Histologic findings. (A) A hydatid cyst and adjacent liver parenchyma are seen. (B) The cyst wall is composed of an acellular laminated membrane and an inner nucleated germinal layer (arrow). Protoscolices and brood capsule (arrowhead) are present. (C) The liver shows a fibrinous wall and inflammatory cells infiltration, including lymphocytes, eosinophils, and histiocytes.
DISCUSSION
Hydatid cyst is a parasite disease caused by the larval forms of Echinococcus tapeworms. Infections by E. granulosus are the most common. Humans are accidental intermediate hosts and become infected by ingestion of food contaminated with eggs shed by dogs or foxes. After ingestion, the eggs of E. granulosus hatch, and the larval oncospheres pass to the liver by the portal vein. Three quarters of infected individuals develop one or more hepatic cysts. The majority occurs in the right lobe, but they may be multiple and involve all lobes of the liver. A hydatid cyst is white, spherical, and filled with fluid. It varies from a few millimeters to many centimeters in diameter.1 Because of its slow growth, the diagnosis may be delayed for months to years after the initial infection. Clinical manifestations include hepatomegaly, obstructive jaundice, and cholangitis. Complications include cholangitis and rupture. If the patient is untreated, the hydatid cyst can be fatal.
The adult E. granulosus is a small tapeworm capped by a scolex at the anterior terminus, and measures 3 to 5 mm in length. Four suckers and a double crown of 28-50 hooks emerge from the scolex.9 The cyst wall has a laminated membrane lined by a germinal layer. This membrane is about 1 mm thick and has no nuclei. The germinal layer is 10 to 25 µm in thickness and contains nuclei. In Korea, hydatid cysts are uncommon and are typically imported by travelers or workers from endemic areas.2-4 In the present case, the patient was a foreign worker who had lived the first 26 years of his life in an endemic area. Therefore, this infection probably originated in an endemic area.
Cytologically, protoscolices, hooklets, and fragments of the laminated membrane are commonly found in hydatid cysts.5-8 In some cases, only laminated membranes were present in the inflammatory background.10-12 In the current case, protoscolices, hooklets, and laminated membranes were identified and the background showed necrotic debris and inflammatory cells. The liver is the most frequently involved organ. In cases of hydatid cysts that involve atypical locations and other organs, the diagnosis can be difficult. FNAC appears to be a safe and useful method in the diagnosis of hydatid cyst, although arguments regarding this issue persist.13 Cytologic diagnosis of hydatid cysts has been reported in the lung,14 omentum,15 muscle,16 soft tissue,10,12 brain,17 orbit,18 and joints.11
The differential diagnosis of hepatic hydatid cyst includes abscess, hemangioma, and non-parasitic cysts such as solitary bile duct cyst and hepatobiliary cystadenoma. It may be difficult to find protoscolices in FNAC. Hydatid cyst should be considered when fragments suggestive of a laminated membrane are present on smears without evidence of protoscolices.12 A definite diagnosis of hydatid cyst is confirmed by identification of protoscolices, refractile hooklets or fragments of a laminated membrane. Surgical excision of the intact hydatid cyst without rupture is the treatment of choice, to reduce the chance of seeding and recurrence.9
There have been significant advances in the knowledge of Echinococcus biology and the development of more specific and sensitive immunological tests.19 Early diagnosis of hydatid cyst by serology may provide opportunities for early treatment and more effective chemotherapy.20
In conclusion, we presented the cytological features in a case of a hepatic hydatid cyst. FNAC is useful in making a diagnosis of a hydatid cyst of the liver. It is important to include hydatid cyst in the differential diagnosis of cystic lesions in the liver, particularly in those who have lived or traveled in endemic areas.
Notes
No potential conflict of interest relevant to this article was reported.