Human Cutaneous Protothecosis: Report of a Case and Literature Review
Article information
Abstract
The Prototheca species is achlorophyllic algae and rarely causes human infection. Human protothecosis presents clinically as a cutaneous infection, olecranon bursitis, and disseminated systemic disease. We report a case of human cutaneous protothecosis involving the left wrist. A 68-year-old man presented with an ill-defined erythematous lesion with crust at the dorsal aspect of his left wrist. A punch biopsy was performed to reveal the histologic features of granulomatous inflammation with necrosis at the upper dermis, containing Prototheca organisms, of which, the characteristic features were highlighted by special staining. Through a molecular study, the Prototheca zopfii species was identified.
The Prototheca species is classified as achlorophyllic algae that does not possess chloroplast or pyrenoids and behaves as saprophytes. It rarely causes human infection, and clinically, protothecosis presents as a cutaneous infection (66%), olecranon bursitis (15%), and disseminated systemic disease (19%).1,2 Since the first description of human protothecosis in 1964 by Davies et al.,3 approximately 100 cases of human cutaneous protothecosis have been reported in the English literature.2,4 Among the various species of Prototheca, human cutaneous infection by Prototheca zopfii is an extremely rare event and only a few cases have been reported in the English literature. We report a case of human cutaneous protothecosis involving the left wrist identified as Prototheca zopfii.
CASE REPORT
A 68-year-old man presented with an ill-defined erythematous lesion with crust at the dorsal aspect of his left wrist (Fig. 1). The skin lesion developed approximately a month ago without any traumatic history, and the patient complained of poor oral intake and diarrhea for a week. He had been suffering from osteoarthritis and had taken medications for twenty years. He was surgically treated for small bowel perforation, adhesion, and panperitonitis 3 years ago. His occupation was gathering trash for recycling.

Erythematous nodular lesion with crust is seen on the left wrist.
A punch biopsy was performed to reveal the histologic features of granulomatous inflammation with confluent necrosis at the upper dermis containing many Prototheca organisms (Figs. 2, 3). On periodic acid-Schiff after diastase digestion special staining, non-budding spherical organisms with multiple sporangia containing endospores were observed with a morula- or cartwheel-like appearance, which is the characteristic feature of the Prototheca species (Fig. 4). The organisms were approximately 20 µm in diameter and had a thick cell wall. Upon crystal violet staining, the organisms exhibited multiple small bluish dots (Fig. 5).
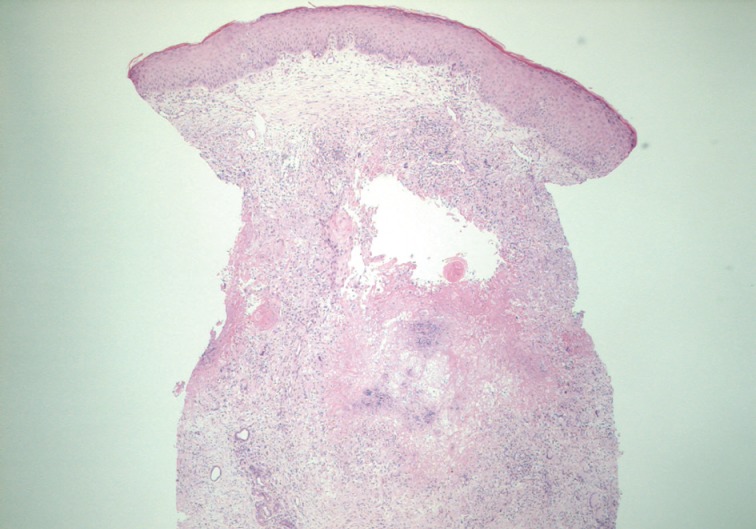
An ill-defined granulomatous inflammation is noticed in the dermis.
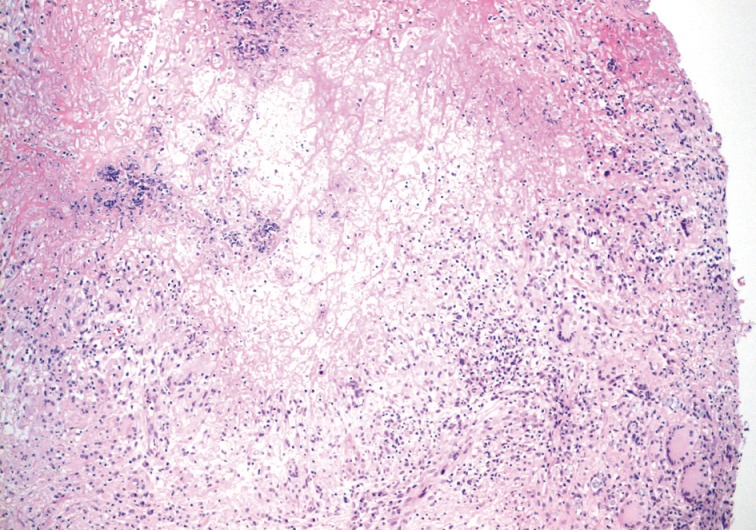
Granulomatous inflammation presents with epithelioid histiocytes, giant cells, and necrosis.
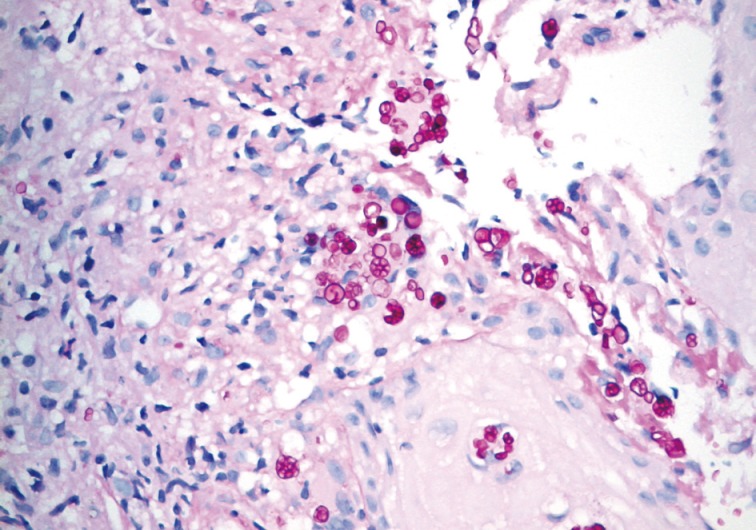
Prototheca sporangia exhibiting a morula-like appearance are highlighted on a periodic acid-Schiff after diastase digestion.
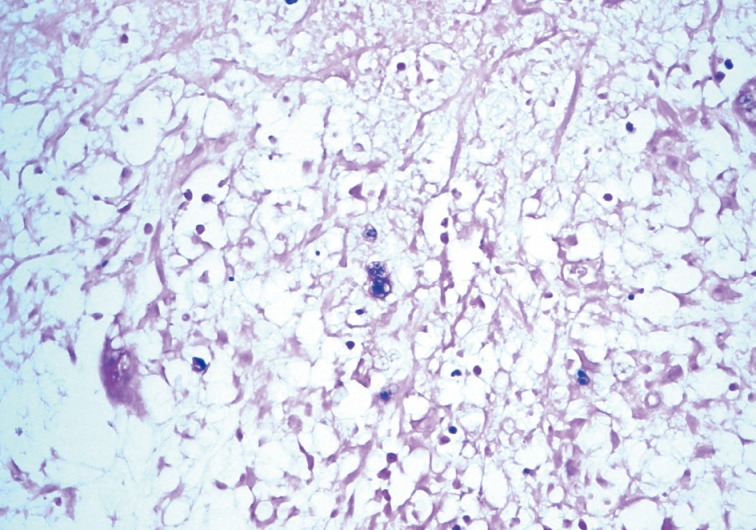
Crystal violet staining demonstrates multiple small bluish dots in the organisms.
For specification of the species, small subunit ribosomal DNA (SSU rDNA) was amplified by polymerase chain reaction using the universal primers NS3 (5'-GCAAGTCTGGCCAGCAGCC-3') and NS8 (5'-TCCGCAGGTTCACCTACGGA-3'). The sequences were submitted to a BLASTn search by using the National Center for Biotechnology database (NCBI; http://www.ncbi.nlm.nih.gov/BLAST).5 The sequences of the SSU rDNA regions of the isolate were 99% identical with Prototheca zopfii.
The patient was given antifungal agent itraconazole, and the symptoms were relieved.
DISCUSSION
Prototheca is ubiquitously isolated from tap water, freshwater streams, swimming pools, soil, stables, and foodstuffs, such as shrimp, cow's milk, butter, potato peel, and bananas.2 A traumatic inoculation plays a role in protothecal infections.2 The major sites of involvement are the exposed areas, including the upper and lower extremities. In the upper extremities, the distal parts are mainly infected, such as fingers, wrists, dorsum of hands, and forearms.6 Other sites of involvement include the forehead, cheek, eyelid, nose,6 scalp, chest, and neck. The patient in this case had no history of trauma, but his occupation involved collecting trash for recycling. The patient's level of hygiene therefore may be poor.
Cutaneous protothecosis can be associated with an underlying disease or immunosuppression in the form of kidney transplantation, malignancy with chemotherapy or radiotherapy, diabetes mellitus,6 steroid administration, systemic lupus erythematosus, chronic obstructive pulmonary disease, myasthenia gravis, congestive heart failure, acquired immunodeficiency syndrome, gout arthritis,6 and rheumatoid arthritis. Malignancies associated with the protothecal infection involve the hematologic system (acute myelogenous leukemia, Hodgkin lymphoma, and chronic lymphocytic leukemia), breast, and uterus.2
Cutaneous lesions are described as ulcerations, erythematous plaques, subcutaneous papules, vesicles, erythematous nodules, verrucous or herpetiform lesions,3 infiltrating nodules, and pyoderma-like lesions.6 The tissue reaction can exhibit a minimal cellular response, a chronic granulomatous reaction, or a mixed acute and chronic granulomatous infiltrate with eosinophilic infiltration.1
The Prototheca species consists of large nonbudding cells with spherical to oval contours and a prominent cell wall. They exhibit the characteristic endospores with a cartwheel-like appearance on a periodic acid-Schiff stain. However, the non-sporulating cells may resemble common pathogens, such as Blastomyces dermatitidis, Cryptococcus neoformans, Paracoccidioides brasiliensis, and Pneumocystis carinii. The different sizes of the sporangia is helpful to discriminate the Prototheca species from these non-sporulating organisms.4 The Prototheca species measures 3 to 30 µm, have double-layered walls, and multiple endospores with a morula-like appearance. The size of Blastomyces species ranges from 8 to 15 µm and exhibits double-refractile cells. The Cryptococcus species is the smallest species (2 to 15 µm) and has a polysaccharide capsule highlighted by mucin stain and demonstrates budding without endospores. The Paracoccidioides species measures 5 to 60 µm and exhibits a mariners-wheel appearance. The sporangia of Coccidioides are larger than the Prototheca species in size, and the endospores are smaller. Electron microscopic findings are helpful in distinguishing the Prototheca species from the Chlorella species which have chloroplasts and a triple-layered cell wall in contrast to the double-layered wall in the Prototheca species.7
Various species have been classified as Prototheca wickerhamii, Prototheca zopfii, Prototheca stagnora, Prototheca ulmea, and Prototheca blaschkeae.2 The human protothecosis is caused by only two species (Prototheca wickerhamii and Prototheca zopfii), and Prototheca wickerhamii is the most common agent. Prototheca zopfii mainly causes bovine mastitis and canine systemic infection. It infects humans rarely with a relatively poor prognosis. About 10 cases of human protothecosis clarified as Prototheca zopfii have been reported in the English literature (Table 1).8 In Korea, 9 cases of cutaneous protothecosis have been reported and all of them were identified as the Prototheca wickerhamii species.9 This is the first report of human cutaneous infection caused by Prototheca zopfii in Korea.

Cases of human protothecal infection caused by Prototheca zopfii
Prototheca wickerhamii infections exhibit a susceptibility to antifungal agents and are easily treated. The prognosis of Prototheca zopfii infections is relatively poor. Therefore, the precise identification of this species is challenging and important both pathologically and clinically. The sporangia of Prototheca wickerhamii (7 to 13 µm) are small and round with symmetrical morula formation, while those of Prototheca zopfii (14 to 16 µm) are oval and cylindrical with relatively asymmetrical random internal segmentation.2,7 The confirmative diagnosis on the species can be made by a culture on Sabouraud's dextrose agar, a carbohydrate assimilation test, a yeast biochemical card, or an immunofluorescence study using species-specific antibodies and a molecular study assessing SSU rDNA.2,5,19,20
The Prototheca species is an uncommon cause of human infection in both immunocompetent and immunocompromised patients. The clinical presentation and tissue reaction of cutaneous infections are similar to the lesions caused by a common deep fungal infection. Although most of the cutaneous protothecosis exhibit an indolent course, disseminated cutaneous lesions can develop under immunosuppressive conditions. The characteristic structures, detected upon histopathologic examination, aid in the precise diagnosis of protothecosis in differential diagnosis with a common cause of fungal infection.
Notes
No potential conflict of interest relevant to this article was reported.