Castleman's Disease of the Renal Sinus Presenting as a Urothelial Malignancy: A Brief Case Report
Article information
Abstract
Castleman's disease is a rare benign lymphoproliferative disorder that frequently affects lymph nodes of the mediastinal thorax and the neck. It very rarely affects the renal sinus. We report a case of Castleman's disease arising in the renal sinus in a 64-year-old man. The patient visited the hospital with the chief complaint of hematuria. Abdominal computed tomography revealed a homogeneous mass in the sinus of the left kidney, radiologically interpreted as a malignant urothelial tumor. Subsequently, nephroureterectomy was performed, after which microscopic examination of the specimen revealed a diffuse lymphoproliferative lesion with reactive lymphoid follicles of various sizes and prominent plasma cell infiltration of interfollicular spaces, highlighted by immunohistochemical staining for CD138. The lesion was diagnosed as Castleman's disease of the plasma cell type. Although preoperative diagnosis of Castleman's disease is difficult and the incidence is exceedingly rare, it should be considered in the differential diagnosis of renal sinus tumors.
Castleman's disease, also known as angiofollicular hyperplasia or giant lymph node hyperplasia, is an uncommon benign lymphoproliferative disorder, and can be histologically classified into two distinct types: the hyaline vascular type and the plasma cell type.1 The hyaline vascular type is the more common of the two, and presents microscopically with small hyaline follicles and intrafollicular capillary proliferation. In contrast, the plasma cell type exhibits larger follicles and intervening sheets of plasma cells, and takes on less of a vascular appearance.1 The disease can be further clinicopathologically divided into either the unicentric or multicentric type. The hyaline vascular type is usually unicentric, and involves a single lymph node or a regional group of nodes. The plasma cell type is more commonly multicentric.2 Castleman's disease is frequently found in the lymph nodes of the mediastinal thorax and the neck area,1,2 but is rarely in the renal sinus. Due to a lack of tumor-specific signs, diagnostic imaging alone is unable to differentiate Castleman's disease from others, rendering preoperative diagnosis thereof quite difficult.3 Here we present a case of Castleman's disease arising in the renal sinus, clinically misdiagnosed as a urothelial malignancy.
CASE REPORT
A 64-year-old man visited our hospital with the chief complaint of microscopic hematuria for the past 2 months. Laboratory tests were unremarkable and urine cytology was normal. Abdominal computed tomography (CT) revealed a homogeneous solid tumor with slightly low attenuation in the left renal sinus (Fig. 1). The left renal pelvis had marked wall thickening with peripelvic soft tissue infiltration. The left proximal ureter and major calyces also had thickened walls with infiltrative features. Altogether, these abdominal CT findings were suggestive of invasive urothelial carcinoma arising in the left pelvis with involvement of renal sinus soft tissue. Nephroureterectomy was performed, and the cut surface of the renal sinus revealed a grayish-white solid tumor of rubbery consistency. The tumor was primarily located in the renal pelvis, but extensions to the renal calyces and proximal ureter were suspicious. The pelvic tumor mass measured 4×2.5 cm and exhibited peripelvic infiltrative features (Fig. 2). However, the mucosal surfaces of the renal pelvis, ureter and calyces were smooth, and there was no evidence of urothelial malignancy. Additionally, the mucosal layers of the renal pelvis, calyces and ureter were intact without abnormal urothelial changes. Microscopically, the tumor occupying the renal sinus contained widely scattered, hyperplastic lymphoid follicles, characteristic of a lymphoproliferative lesion. The follicles varied in size and showed polarized germinal centers; moreover, interfollicular spaces were markedly infiltrated by mature plasma cells, highlighted by CD138 immunostaining (Fig. 3). Immunostaining for κ and λ immunoglobulin light chains indicated that the plasma cells were polyclonal in origin. Immunostaining for human herpes virus 8 (HHV-8) was performed, the results of which were negative. These histological and immunohistochemical findings were compatible with a diagnosis of Castleman's disease of the plasma cell type. Three months after the operation, there was no evidence of disease recurrence on follow-up abdominal CT.

Abdominal computed tomography reveals a homogeneous infiltrative mass in the left renal sinus with relative low attenuation compared to the renal parenchyma (arrows).

Gross findings. The resected kidney contains a 4×2.5 cm gray-whitish infiltrative pelvic mass (arrows) with marked thickening of the walls of the proximal ureter and major calyces.
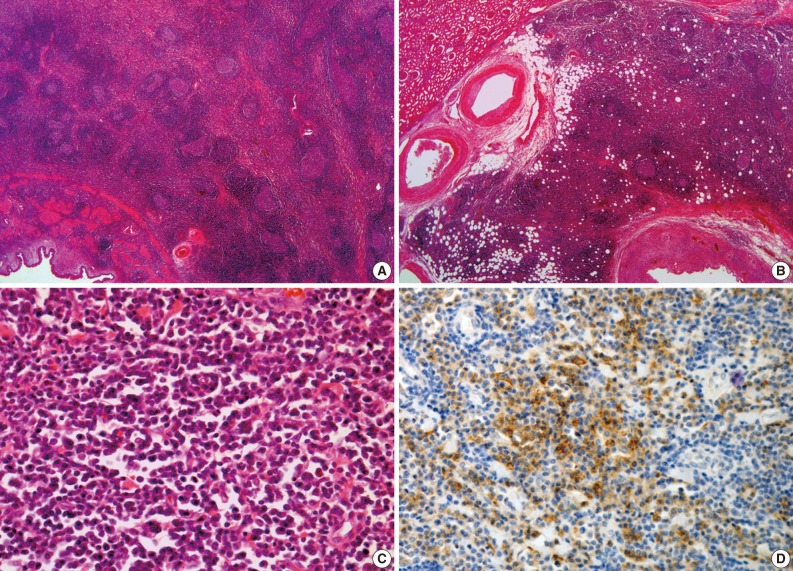
Histopathologic findings. (A) The pelvic tumor is a benign lymphoproliferative lesion with widely scattered, hyperplastic lymphoid follicles. The pelvic urothelium is intact. (B) The renal calyces also contain a submucosal lymphoproliferative lesion. (C) Marked plasma cell infiltration in interfollicular spaces. (D) The plasma cells are positive for CD138 upon immunostaining.
DISCUSSION
The occurrence of Castleman's disease in the renal sinus is exceedingly rare.1 To the best of our knowledge, only a few cases have been reported.1,3-6 The clinicopathological characteristics of the reported cases, involving six males and one female, are summarized in Table 1. Although Castleman's disease generally shows no gender preference,2 cases involving the renal sinus appeared to show a male predominance. The median age for Castleman's disease is in the fourth decade.2 However, the mean age of the cases involving the renal sinus was 65 years. The main presenting symptoms included abdominal pain, weight loss, anorexia, and microscopic hematuria. Three of the cases were clinically unicentric and four were multicentric. Five cases were of the plasma cell type, one of the hyaline vascular type and one of mixed type. The patient in the present case, a 64-year-old male, presented with symptoms of microscopic hematuria, and his disease was histologically classified as plasma cell type and clinically as unicentric type.
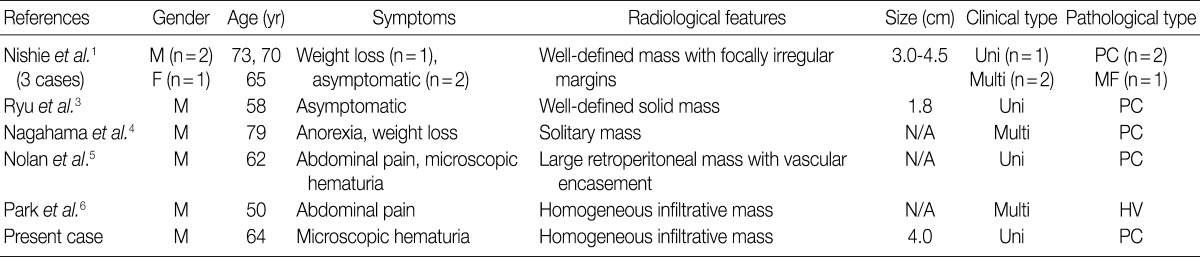
Clinicopathological characteristics of previously reported cases of Castleman's disease with renal sinus involvement
Although the exact pathophysiology of Castleman's disease is unknown, recent reports suggest that HHV-8 infection may stimulate B lymphocytes to induce interleukin 6 (IL-6) production in the mantle zone; IL-6 overproduction has been shown to be associated with the systemic manifestations of Castleman's disease, especially in cases of multicentric disease.7 In our case, immunostaining for HHV-8 was performed, but the result was negative.
Preoperative diagnostic imaging methods are not useful in differentiating Castleman's disease arising in the renal sinus from other diseases because of a lack of tumor-specific imaging features. Previously, Nishie et al.1 described the CT and magnetic resonance imaging features of three cases of Castleman's disease involving the renal sinus. They reported that the renal sinus lesions formed in Castleman's disease can appear as homogeneous masses with mild enhancement, such as is often observed in malignant lymphomas. Thus, it is difficult, on the basis of radiological findings, to differentiate Castleman's disease from malignant lymphomas infiltrating the renal sinus. Other differential diagnoses may include invasive urothelial carcinoma, granulomatous diseases, sarcomas, and metastases. Consequently, pathological evaluation is currently the only method of identifying Castleman's disease of the renal sinus.
Here we have described an extremely rare case of unicentric Castleman's disease of the plasma cell type arising in the renal sinus. Although preoperative diagnosis of Castleman's disease is difficult and accurate diagnosis is only possible by histopathologic evaluation, it should be considered in the differential diagnosis of renal sinus tumors.
Notes
No potential conflict of interest relevant to this article was reported.