Potential Role for a Panel of Immunohistochemical Markers in the Management of Endometrial Carcinoma
Article information

Abstract
Background
In order to improve the efficacy of endometrial carcinoma (EC) treatment, identifying prognostic factors for high risk patients is a high research priority. This study aimed to assess the relationships among the expression of estrogen receptors (ER), progesterone receptors (PR), human epidermal growth factor receptor 2 (HER2), Ki-67, and the different histopathological prognostic parameters in EC and to assess the value of these in the management of EC.
Methods
We examined 109 cases of EC. Immunohistochemistry for ER, PR, HER2, and Ki-67 were evaluated in relation to age, tumor size, International Federation of Gynecology and Obstetrics (FIGO) stage and grade, depth of infiltration, cervical and ovarian involvement, lymphovascular space invasion (LVSI), and lymph node (LN) metastasis.
Results
The mean age of patients in this study was 59.8 ± 8.2 years. Low ER and PR expression scores and high Ki-67 expression showed highly significant associations with non-endometrioid histology (p = .007, p < .001, and p < .001, respectively) and poor differentiation (p = .007, p < .001, and p <. 001, respectively). Low PR score showed a significant association with advanced stage (p = .009). Low ER score was highly associated with LVSI (p = .006), and low PR scores were associated significantly with LN metastasis (p = .026). HER2 expression was significantly related to advanced stages (p = .04), increased depth of infiltration (p = .02), LVSI (p = .017), ovarian involvement (p = .038), and LN metastasis (p = .038). There was a close relationship between HER2 expression and uterine cervical involvement (p = .009). Higher Ki-67 values were associated with LN involvement (p = .012).
Conclusions
The over-expression of HER2 and Ki-67 and low expression of ER and PR indicate a more malignant EC behavior. An immunohistochemical panel for the identification of high risk tumors can contribute significantly to prognostic assessments.
Endometrial carcinoma (EC) is the most common gynaecologic malignancy among women worldwide with 287,000 new cases and 74,000 mortalities per year [1]. EC is the fourth most common type of cancer in females [2,3]. Traditionally, ECs have been classified into two types. The more common is type I, mostly endometrioid carcinomas, which are estrogen-dependent cancers with a relatively good prognosis. On the other hand, type II tumours are not estrogen-driven and affect older age groups. These tumours have a poor prognosis and demonstrate more common extrauterine spread. The prototype for this group is serous carcinoma [1,4,5]. In order to improve the efficacy of EC treatment, identification of high-risk prognostic factors is a high research priority. Early assessment could enable conservative therapy in patients with favorable prognosis as well as reserve effective and more radical therapy for patients with aggressive forms of the tumor [6]. The use of estrogen receptor (ER), progesterone receptor (PR), human epidermal growth factor receptor 2 (HER2), and Ki-67 have been routinely used in breast cancer cases for molecular subtyping and guiding treatment. However, unlike breast cancer, there is no molecular classification for EC based on such markers [7]. Recently, integrated genomic characterization of EC revealed four genomic classes; however, receptor status is not involved in this molecular classification [8].
Numerous studies showed that the EC prognosis is closely related to patient age, tumour grade, depth of invasion and/or cervical involvement, and the occurrence of lymph node metastases [9]. Some potential biological markers including hormone receptors, oncogenes, and tumour suppressor genes are also involved. However, no single marker was found to be indicative of EC often enough to allow routine use in the sub-classification of EC [10]. Therefore, in the current study, a panel of immunohistochemical markers (ER, PR, Her-2, and Ki-67) was tested to ascertain their relationships with the histopathological prognostic parameters of EC. The aim was to identify suitable markers to guide treatment and assess prognosis of EC patients.
MATERIALS AND METHODS
Sample selection
Archival material of randomly-selected hysterectomy specimens of 109 EC cases were retrieved from the Pathology Department. These cases were diagnosed in the period between 2005 and 2017. Corresponding files of these cases were retrieved from the Clinical Oncology and Nuclear Medicine Departments at Mansoura University. The histological types were endometrioid (89 cases), serous (12 cases), undifferentiated (one case), dedifferentiated (one case), and carcinosarcoma (three cases). The remaining three cases showed mixed patterns. The major component in two was endometrioid; the other was serous carcinoma. Hematoxylin and eosin (H&E) stained slides for every case were reviewed by two independent pathologists. International Federation of Gynecology and Obstetrics (FIGO) revised criteria in 2009 were used for grading and staging of cases [11]. All procedures performed in the current study were approved by the ethical committee of Mansoura University (Institutional Review Board [IRB] code number MD15.09.08, dated 18/09/2015) in accordance with the 1964 Declaration of Helsinki and its later amendments. Formal written informed consent was not required with a waiver by the IRB.
Tissue microarray construction
The tissue microarray (TMA) was constructed as previously published [12]. Briefly, a representative slide for each tumor was selected and an area of the tumor was circled. Using the manual tissue arrayer (MTA-1, Estigen, Tartu, Estonia), the areas of interest of a donor block were cored using tissue punches of 0.6 mm diameter. The cores were then transferred into the recipient block. Three cores were taken from each tumour. In carcinosarcoma cases, only the epithelial component was assessed. Sections from these microarrays were then H&E stained and tested for spot adequacy.
Immunohistochemistry
Sections from the microarray were stained with antibodies against ER, PR, HER2 (Rabbit, monoclonal, Genemed, South San Francisco, CA, USA) and Ki-67 (mouse, monoclonal, Genemed) according to the instructions of the manufacturers. The positive control for ER and PR in this study was normal endometrial glands and stroma where these receptors show nuclear expression. The positive control for HER2 was positive breast carcinoma tissue. The positive internal control for Ki-67 was tonsillar lymphoid follicles.
Evaluation of the staining
Slides were examined by two independent pathologists blinded to patient characteristics and outcome. For ER and PR, we applied a scoring system that depended on immunoreactivity distribution and intensity [13,14]. The percentage of stained cells was scored as follows: 1, 0%–25%; 2, 26%–75%, and 3, ≥ 76%. The intensity of staining was also reported as 1, absent or weak; 2, moderate; and 3, strong. The sum of the two values equalled the score. Tumours were then subdivided into three categories depending on this immunohistochemical score. Category I corresponded to a score of 2, category II to a score of 3–4, and category III to a score of 5–6.
U.S. Food and Drug Administration criteria were used for evaluation of HER2 scoring [15]. The scoring was 3+ if complete with strong membranous staining in more than 10% of tumor cells; 2+ if complete, weak to moderately intense staining of the membrane was seen in greater than 10% of tumor cells; 1+ if incomplete staining of the membrane was found in more than 10% of tumor cells and a score of 0 was assigned when no staining or membranous staining in less than 10% of tumor cells was present. A score of 3+ was considered positive, a score of 2+ was equivocal positive and scores of 1+ and 0 were negative.
Ki-67 was evaluated as the percentage of cells showing positive nuclear reactivity in at least 500 histologically recognized tumour cells counted at × 400 magnification.
For TMA validation purposes, the originally recorded immunohistochemical results from the initial routine histopathology reports of ten patients were compared to those of the current experiment. Similar findings were observed in the TMAs compared to full tissue sections.
Statistical analysis
Data were analysed by IBM SPSS software package ver. 20.0 (IBM Corp., Armonk, NY, USA). Qualitative data were described as number and percent. Quantitative data were described using median (minimum and maximum) and interquartile range for non-parametric data and mean and standard deviation for parametric data after testing for normality using the Kolmogrov-Smirnov test. The significance of the results obtained was judged at the 5% level. The tests used were chi-square, Monte Carlo, Fisher exact, Student t-, F- (ANOVA), Mann-Whitney, Kruskal-Wallis, and Spearman correlation.
RESULTS
Clinicopathological features of the studied cases
Patient ages ranged from 37 to 79 years with a mean age of 59.8 ± 8.2 years. Most of the cases (88 patients, 80.7%) in this study were postmenopausal.
Tumors ranged from 1 to 14 cm in largest dimension with a median value of 3 cm. There were 36 cases of grade 1 (33%), 43 cases of grade 2 (39.4%), and 30 cases were high grade carcinomas (27.5%) including grade 3 endometrioid, serous, mixed, undifferentiated and dedifferentiated carcinomas, and carcinosarcomas. In three cases (2.7%) the tumour was limited to the endometrium, 69 (63.3%) cases showed infiltration of the inner myometrial half, the tumour infiltrated the outer half in 26 cases (24%), and the serosa was infiltrated in three cases (2%). Cervical involvement was found in 20 cases (18%), 71 cases (65%) were free from cervical infiltration and in 14 cases (12.8%) cervical involvement was not determined due to suboptimal surgery. Adnexal metastases were found in 11 cases (10%), 83 cases (76%) were free from adnexal infiltration, and in 15 cases (13.7%) adnexal infiltration was unknown due to suboptimal surgery. There were 71 cases (65.1%) in stage I (56 stage IA and 15 stage IB), 15 cases in stage II (13.8%), 10 cases (9%) in stage IIIA, only two cases were stage IIIB, and one case was stage IVA. Lymphovascular emboli were found in 29 cases (26.6%).
The association of immunohistochemical results with histopathological prognostic parameters
The distribution of immunohistochemical data in relation to individual histopathological parameters is presented in Tables 1–4. The relationships among ER, PR expression, and other markers (HER2-neu and Ki-67) as well as the relationship between HER2-neu expression and Ki-67 expression are presented in Tables 5. Representative examples of the different expression patterns are show in Fig. 1.
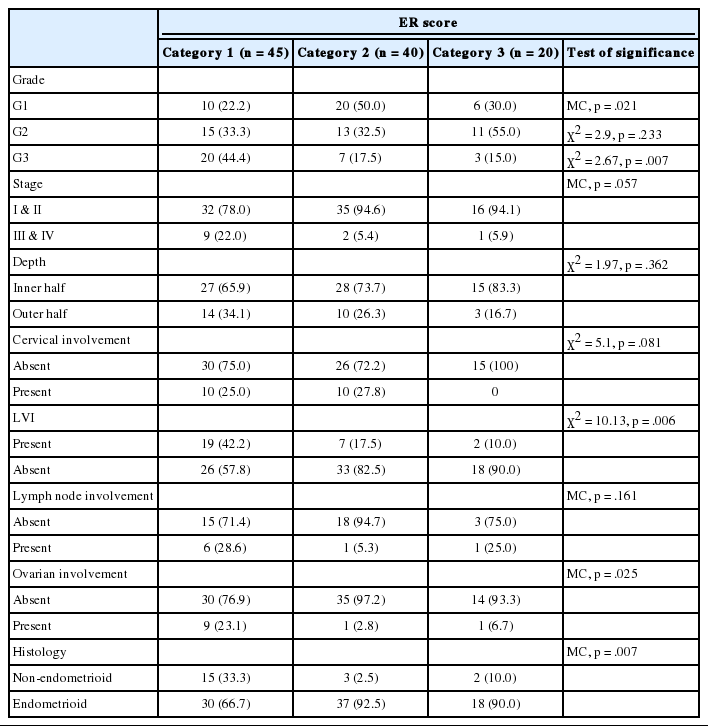
ER expression score in relation to histopathological parameters
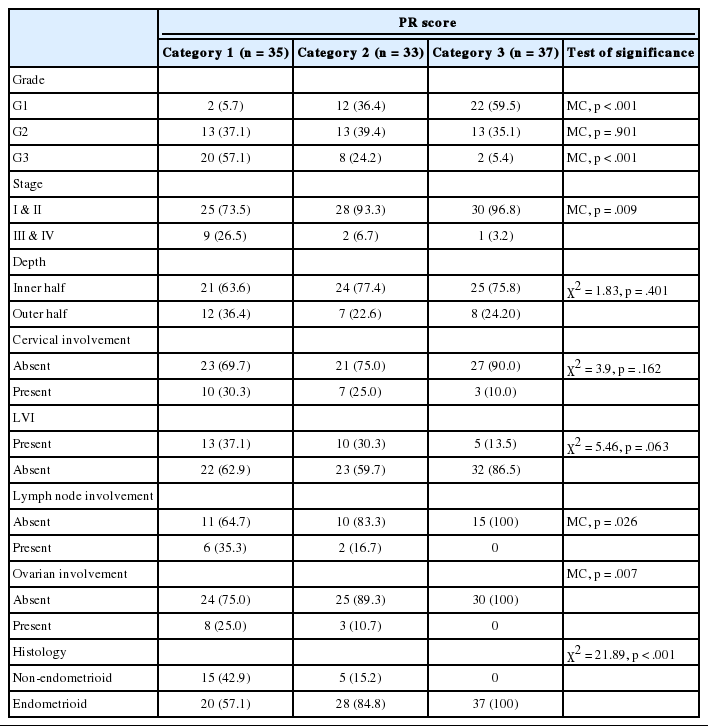
PR expression score in relation to histopathological parameters
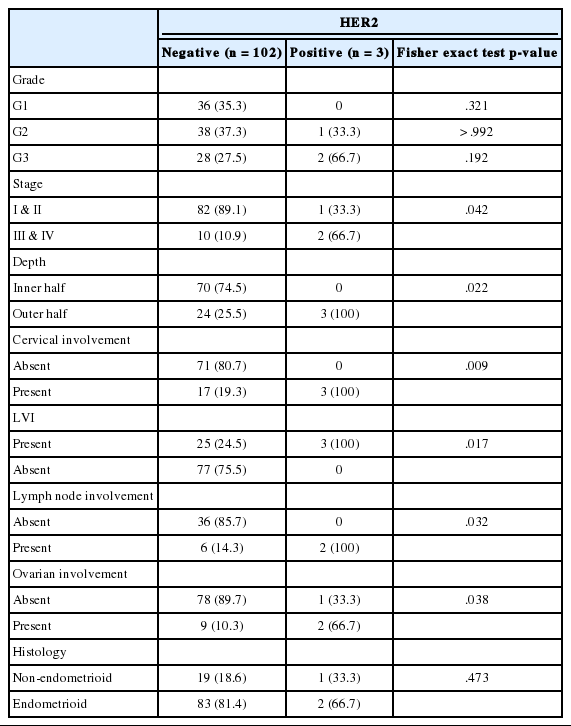
The expression of HER2 in relation to histopathological parameters
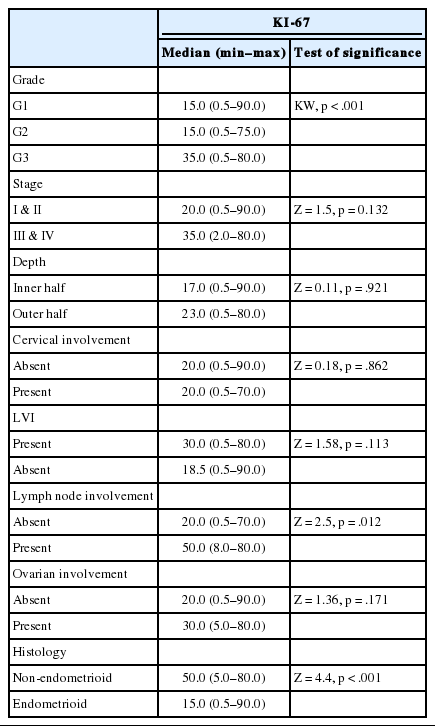
The expression of Ki-67 in relation to histopathological parameters

Relationship between ER, PR expression and other markers (HER2 and Ki-67)
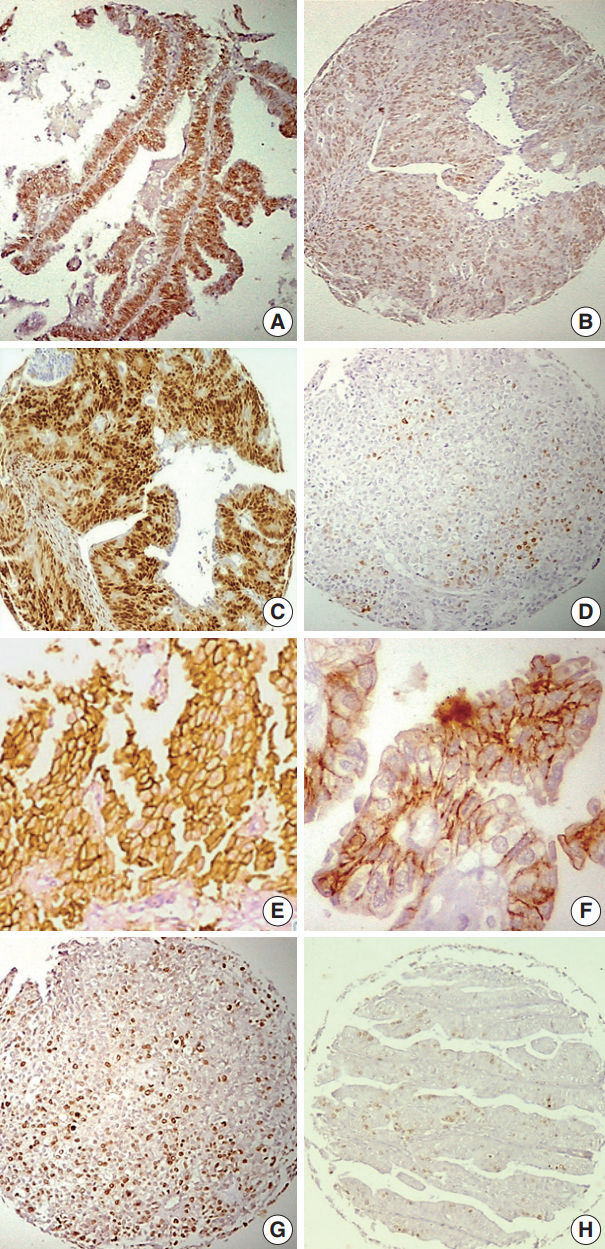
Examples of different patterns of immunohistochemical expression in endometrial carcinomas. (A) Estrogen receptor (ER) expression score (6) in a case of well differentiated endometrial carcinoma (EC). (B) ER expression score (4) in a poorly differentiated EC. (C) progesterone receptor (PR) expression score (6) in a moderately differentiated EC. (D) PR expression score (2) in a poorly differentiated EC. (E) Positive human epidermal growth factor receptor 2 (HER2) overexpression (score +3) in a case of poorly differentiated EC. (F) HER2 score (+ 1), which is considered negative, in a well differentiated EC. (G) High Ki-67 index in a poorly differentiated EC. (H) Low Ki-67 index in a well differentiated EC.
ER and PR scores were statistically associated (p < .001). There were significant relationships between low ER scores and nonendometrioid histology (p = .007) and higher grade of endometrial cancer (p = .007). The ER score tended to decrease with advanced stage (p = .057). Low ER score was associated with ovarian involvement (p = .025), lymphovascular space invasion (LVSI) (p = .006), and higher Ki-67 values (p = .024).
Low PR expression score was associated with non-endometrioid histology (p < .001), higher tumour grade (p < .001), advanced stage (p = .009), and ovarian involvement (p < .007). The PR score decreased with LVSI (p = .06), and lower score was associated with lymph node metastasis (p = .026). Ki-67 values were higher with low PR score (p = .025).
HER2 expression was significantly associated with advanced tumour stages (p = .04), increased depth of myometrial infiltration (p = .02), greater incidence of LVSI (p = .017), ovarian involvement (p = .038), and lymph node metastasis (p = .038). There was a notable relationship between HER2 expression and cervical involvement (p = .009).
A positive correlation was found between tumour size and Ki-67 index (p = .02). Higher Ki-67 index was linked to more aggressive features such as non-endometrioid histotype (p < .001) and poor differentiation grade (p < .001). There was a strong relationship between higher Ki-67 values and lymph node involvement (p = .012).
Median Ki-67 index value was higher in HER2-neu–positive cases than that of negative cases (p = .482, Mann-Whitney test).
DISCUSSION
EC is the most common gynaecologic cancer worldwide and the incidence is increasing [2,3,16]. EC may not always fit into the dual model of type I and type II cancers: those can be vague clinicopathological designations rather than firm diagnostic entities. Tumours display varying degrees of conformity with both types and have different behaviours and prognoses [17-19]. According to the National Cancer Comprehensive Network guidelines for management of EC, the treatment strategy depends on surgical staging, depth of infiltration and the presence of adverse risk factors such as age, tumour size, LVSI and lower uterine involvement. Adjuvant therapy determinations are made on the basis of pathologic findings in the postoperative specimen. Superficially invasive, low grade (G 1–2) carcinomas in the absence of adverse risk factors can be treated by surgery with post-operative observation. However, in the presence of adverse risk factors, patients need adjuvant radiotherapy. High grade carcinomas with no adverse risk factors may be spared from adjuvant chemotherapy [20].
Both breast and endometrial cancers are among the commonest cancers in females, and both are largely considered to be hormonedependent tumours. In breast cancer, a simple immunohistochemical panel of ER, PR, HER2, and Ki-67 is routinely performed on preoperative or postoperative specimens yielding valuable therapeutic and prognostic information. Similar to breast cancer, this panel may be of value when assessing EC specimens. The information attained may be helpful in guiding patient management and in providing prognostic information about tumour behaviour [7].
In the current work, we assessed the immunohistochemical expression of the same panel of biological markers (ER, PR, HER2, and Ki-67) on 109 cases of EC and their association with histopathological prognostic characteristics. The presence of hormone receptors in ECs correlates with the clinical disease stage, histological grade, and overall survival. The absence of hormone receptors is considered to indicate aggressive tumour behaviour and poor prognosis [21,22]. A recent systematic review and meta-analysis revealed that higher levels of ER and PR were associated with favourable prognosis and longer overall survival [23]. This study showed close associations between low ER and PR scores, nonendometrioid histology and high grade endometrial cancer. Moreover, low PR score was significantly associated with advanced tumour stage. These findings agree with previous studies [21,24,25]. While not statistically significant, the ER score tended to be lower with advanced stage. Some studies failed to show associations between ER and PR expression and tumour stage [26,27]. Our data revealed significant associations between ovarian involvement and low ER and PR scores, an observation in contrast to previous observations [6,28]. This discrepancy may be due to differences in sample size, primary antibody used, and the method of scoring the immunohistochemical results. ER and PR did not show significant association with the depth of myometrial invasion or cervical infiltration as previously reported [25,26]. Low ER score was significantly associated with LVSI; low PR score tended to be associated with LVSI as well, but the strength of the low PR association did not match that of low ER. This agrees with the findings of a previous study [24]. Low PR scores were significantly associated with lymph node metastasis as reported earlier [26]. Consistent with previous studies, high ER and PR scores were highly associated while lower scores were associated with higher Ki-67 values [24,27,29].
The increased expression of HER2 correlates with worse prognosis in various malignant tumours. In their extensive study (483 cases), Morrison et al. [30] demonstrated that the over-expression of HER2 was an independent prognostic factor that correlated with worse survival. Our work confirms a close relationship between HER2 overexpression and some of the traditional prognostic factors of endometrial cancer. In partial agreement with previous studies, we found HER2 expression to be associated with advanced tumour stages and increased depth of myometrial invasion [31-33]. We have not observed, however, any substantial relationship between HER2 overexpression and the grading of ECs. Some previous studies did not show a significant association between HER2 expression and the prognostic parameters [6,33]. In contrast to this, our study revealed that HER2 overexpression was significantly associated with a greater incidence of ovarian and cervical involvement, lymphovascular emboli and LN metastasis, findings in line with a previous observation [4]. We did not find HER2 over-expression to be significantly associated with ER, PR, or Ki-67 expression, a finding inconsistent with that of a study showing significant correlation between HER2 over-expression and high Ki-67 index [4].
Increased Ki-67 expression indicates higher mitotic activity and greater tumour cell proliferation. Some studies revealed that Ki-67 could be an independent prognostic marker of survival in EC [34,35]. On the other hand, Pansare et al. [36] did not find correlations between Ki-67, histological type, grading, and tumour clinical staging. An elevated Ki-67 expression in this study was strongly related to non-endometrioid histotype and poor differentiation. Higher Ki-67 index was also found to be associated with lymph node involvement but not tumour stage, depth of myometrial invasion, cervical infiltration, or ovarian involvement.
Our proposed immunohistochemical panel (ER, PR, HER2, and Ki-67) may be of value for preoperative biopsies. Results may indicate tumour behaviour characteristics, presence of adverse risk factors such as lymphovascular emboli and cervical involvement, and the necessity for more radical surgery with pelvic and para-aortic lymph node dissection [37]. Moreover, the panel may also be performed on postoperative specimens. The panel may be included routinely as an adjunct consideration in the postoperative treatment decision making process. Low risk patients with low grade, superficially invasive tumours may be spared the morbidity of lymphadenectomy as well as the cost and morbidity of radiotherapy. The panel results can also assist in identifying high risk patients requiring more radical surgery, post-operative radiotherapy, and/or chemotherapy [38].
In conclusion, low ER and PR expression scores (category I), together with HER2 overexpression (score + 3) and Ki-67 indices of more than 20%, were associated with more malignant behaviour of ECs. Further studies involving larger numbers of patients are needed to investigate the correlation between this immunohistochemical panel’s results and the recent molecular classification of EC.
Notes
Author contributions
Conceptualization: MA.
Data curation: AS, MA, AAF, SAA.
Formal analysis: AS, MA, AAF, SAA.
Funding acquisition: MA.
Investigation: AS, MA, AAF, SAA.
Methodology: AS, MA, AAF, SAA.
Project administration: MA, SAA, RH, AG, KZ, ESMAH.
Resources: MA, SAA, RH, AG, KZ, ESMAH.
Software: AS, MA, SAA.
Supervision: MA, AMS, EE, AAEHA.
Validation: AS, MA, SAA.
Visualization: AS, MA, AAF, SAA.
Writing—original draft: AS.
Writing—review & editing: AS, MA, AAF, SAA.
Conflicts of Interest
The authors declare that they have no potential conflicts of interest.
Acknowledgements
This study is the outcome of a research project (entitled: Impact of Genetic Alterations on the Management of Endometrial Carcinoma) supported by the research fund unit of Mansoura University.