What’s new in breast pathology 2022: WHO 5th edition and biomarker updates
Article information

Abstract
The 5th edition WHO Classification of Breast Tumours (2019) has introduced changes to our practices. Highlights are presented below, with a focus on modifications to morphological subtype categorization. In addition, we summarize important updates to ER and PR testing made in the 2020 ASCO/CAP guidelines, and briefly discuss PD-L1 and Ki-67 testing in breast cancer.
RARE VARIANTS OF INVASIVE BREAST CARCINOMA OF NO SPECIAL TYPE (IBC-NST)
• The prior WHO (4th ed. 2012) classified several tumors as separate entities (listed below). Breast tumors with these “special morphological patterns” now fall under the umbrella category of IBC-NST and are no longer considered to be the following clinically distinct subtypes: oncocytic, lipid-rich, glycogen-rich, clear cell, sebaceous, carcinomas with choriocarcinomatous and pleomorphic patterns, melanocytic, and carcinomas with osteoclast-like stromal giant cells.
INVASIVE BREAST CARCINOMA WITH MEDULLARY PATTERN
• Medullary carcinoma, atypical medullary carcinoma, and carcinoma with medullary features were listed as special subtypes of breast carcinoma in the prior WHO. This diagnostic category has poor interobserver reproducibility; these tumors also show overlapping histologic features with carcinomas that have basal-like molecular profiles and carcinomas with BRCA1 mutations.
• Tumor infiltrating lymphocytes (TILs) may explain the good prognosis of these cancers.
• Carcinomas with a basal-like or medullary pattern (i.e., well-circumscribed, high-grade, syncytial architecture, necrosis, prominent TILs, Fig. 1) now represent one end of the spectrum of TIL-rich IBC-NST; “IBC-NST with medullary pattern” has been proposed to replace “medullary carcinoma.”
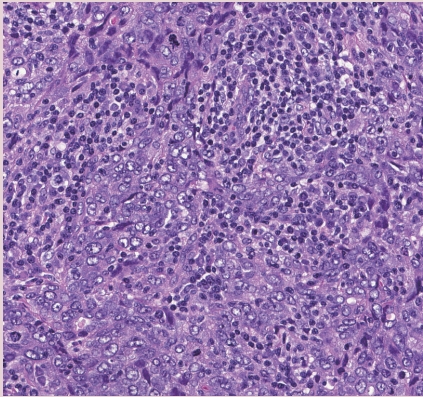
IBC-NST with medullary pattern. High-grade tumor with a syncytial growth pattern and prominent TILs.
NEUROENDOCRINE TUMORS
• True primary neuroendocrine (NE) neoplasms of the breast are rare. They are classified as well-differentiated NE tumors (carcinoid-like and atypical carcinoid-like) and poorly differentiated NE carcinomas (small cell neuroendocrine carcinoma and large cell neuroendocrine carcinoma).
• Distinct NE features and expression of NE markers by IHC are needed for diagnosis, since varying degrees of NE differentiation may be seen in IBC-NST, mucinous carcinomas, solid papillary carcinomas, and others.
• Metastasis must be ruled out before considering a primary breast NE tumor.
• Routine staining on IBC-NST that lacks characteristic NE morphological features is not recommended, due to the lack of clinical relevance.
WELL-DIFFERENTIATED LIPOSARCOMA IN PHYLLODES TUMOR
• Malignant heterologous elements are among the diagnostic criteria for malignant phyllodes tumor.
• Adipocytic differentiation in the stromal component of phyllodes tumor, that is morphologically indistinguishable from well-differentiated liposarcoma of soft tissue, has been found to lack the characteristic MDM2 and CDK4 amplifications seen in well-differentiated liposarcoma (Fig. 2).
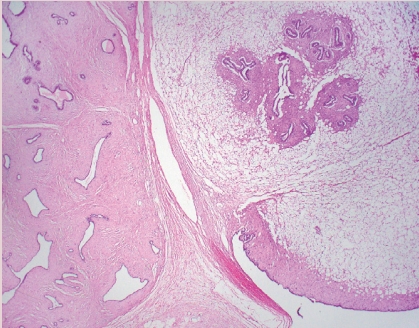
Phyllodes tumor with liposarcomatous differentiation. Other features (stromal atypia, mitotic activity) in this tumor supported the designation as malignant phyllodes tumor.
• Based on recent molecular findings and evidence supporting low metastatic risk, the single criterion of well-differentiated liposarcomatous differentiation is no longer recommended for establishing the diagnosis of malignant phyllodes tumor.
MUCINOUS CYSTADENOCARCINOMA
• This recently described, rare, invasive breast cancer subtype is characterized by cystic spaces lined by neoplastic columnar epithelium with papillae and abundant intracellular and extracellular mucin.
• The tumor border is rounded/encapsulated but there is lack of myoepithelium throughout.
• Coexistent DCIS may be present and is helpful in supporting a breast origin.
TALL CELL CARCINOMA WITH REVERSE POLARITY (TCCRP)
• This recently described, rare, invasive breast cancer subtype has characteristic features that include solid nests of tumor, set in fibrous stroma, that have delicate fibrovascular cores lined by bland columnar epithelial cells (Fig. 3).
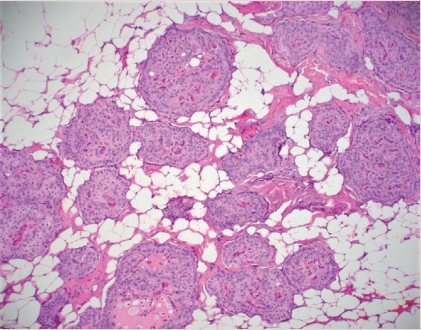
Tall cell carcinoma with reverse polarity (TCCRP). The tumor is characterized by infiltration of nests of tumor cells with fibrovascular cores and bland columnar cells with apically-located nuclei and abundant eosinophilic cytoplasm.
• Cells have abundant eosinophilic cytoplasm with nuclei present at the apical poles (i.e., reverse polarity) that may have grooves and inclusions.
• Despite low grade morphology, these tumors are positive for CK 5/6 and are triple negative for ER, PR, and HER2. IDH2 p.Arg172 hotspot mutations have been reported in 84% of tumors studied.
PROGNOSTIC AND PREDICTIVE BIOMARKERS UPDATE
• PD-L1 (clone 22C3)
- On July 26, 2021, the United States Food and Drug Administration (FDA) approved pembrolizumab for high-risk early-stage triple-negative breast cancer (TNBC) in combination with chemotherapy as neoadjuvant treatment; subsequently it was approved as a single agent adjuvant treatment.
- The FDA converted the accelerated approval of pembrolizumab, in combination with chemotherapy, for the treatment of locally recurrent unresectable or metastatic TNBC tumors that express PD-L1 (clone 22C3) with a combined positive score (CPS) ≥ 10.
- CPS is the number of PD-L1 staining cells (tumor cells, lymphocytes, macrophages) divided by the total number of viable tumor cells, multiplied by 100.
• PD-L1 (clone SP142)
- On August 27, 2021, Genentech withdrew its accelerated indication for atezolizumab plus nab-paclitaxel for the treatment of PD-L1 (clone SP142) positive advanced/ metastatic TNBC.
• Ki-67 (clone MIB-1)
- On October 13, 2021, the FDA approved abemaciclib plus endocrine therapy for hormone receptor positive, HER2 negative, node positive early breast cancer patients with a Ki-67 index ≥ 20%, who are at high risk for recurrence.
- The FDA approved companion diagnostic to abemaciclib is Ki-67 using the MIB-1 PharmDX/Dako Omnis antibody clone.
• 2020 ASCO/CAP ER/PR Guideline Update Highlights [1]
- ER low-positive new reporting recommendation: “The cancer in this sample has a low level (1%–10%) of ER expression by IHC. There are limited data on the overall benefit of endocrine therapies for patients with low level (1%–10%) ER expression, but they currently suggest possible benefit, so patients are considered eligible for endocrine treatment. There are data that suggest invasive cancers with these results are heterogeneous in both behavior and biology and often have gene expression profiles more similar to ER-negative cancers.”
- PR testing is optional in DCIS.
- There is a new recommendation for laboratories to establish a specific protocol to ensure the validity of ER low-positive (1–10%) or negative (0 or < 1%) interpretations and results.
Meet the Authors
Dr. Muller has been an author for PathologyOutlines since 2020 and part of the PathologyOutlines editorial board since 2021. She is currently an Assistant Professor at Dartmouth-Hitchcock Medical Center where she practices Breast and Gynecologic Pathology.
Dr. Jorns has been an author for PathologyOutlines since 2014 and part of the PathologyOutlines editorial board since 2020. She is currently an Associate Professor at the Medical College of Wisconsin where she primarily practices Breast Pathology.
Dr. Tozbikian has been an author for PathologyOutlines since 2018, part of the PathologyOutlines editorial board since 2019, and Deputy Editor in Chief for Breast Pathology since 2021. He is currently an Associate Professor at The Ohio State University Wexner Medical Center where he practices Breast and Genitourinary Pathology.