Metastatic choroidal melanoma in the breast: a case report and review of the literature
Article information

Abstract
The breast is an unusual site for metastases, accounting for less than 2% of malignant breast lesions but include those from malignant melanomas, carcinomas, sarcomas, and lymphomas from various organs. We diagnosed a very rare case of metastatic choroidal melanoma for a 67-year-old female who presented with a right breast lump and who had been previously diagnosed with choroidal melanoma-monosomy 3 in 2017. To the best of our knowledge, only five such cases have been published so far, with one in a male patient.
The breast is an unusual site for metastases, which represent less than 2% of malignant breast lesions but include those from malignant melanomas, carcinomas, sarcomas, and lymphomas from various organs [1]. Due to their scarcity, metastatic lesions in the breast are often misdiagnosed as primary breast cancers, which can result in inappropriate treatment.
The most common sites of uveal melanoma (UM) are the choroidal melanocytes (85%–90%), the ciliary body (5%–8%), and the iris (3%–5%) [2]. UM affects approximately 500–600 patients every year in the United Kingdom, and age at presentation is approximately 60 years, except for iris melanomas which usually present at a younger age [3]. Outcomes for uveal melanomas are poor once metastasis occurs; median survival from the time of development of distant metastatic disease is 2–12 months and 1-year survival is 10%–15% [3]. A UM spreads exclusively hematogenously, unless it becomes large enough to infiltrate the conjunctival lymphatics. As per the Collaborative Ocular Melanoma Study, the most frequent sites of metastases at time of death are liver (93%), lung (24%), and bone (16%). More than 80% of cases had multiple sites of metastasis [4].
Here, we present a case of metastatic choroidal melanoma in the breast.
CASE REPORT
A 67-year-old female presented in 2017 with reduced vision in the left eye. A transscleral biopsy was performed, and a diagnosis of choroidal melanoma-monosomy 3 was made. The patient was treated by Ruthenium plaque brachytherapy, which was later complicated by retinal detachment. Almost a year later in follow-up, the patient underwent a computerized tomography scan of the thorax, abdomen, and pelvis and was found to have multiple lung and liver metastatic deposits. Unfortunately, the patient was lost to follow-up at this stage.
In 2021, the patient presented with right breast lump, and ultrasound of the right breast revealed an irregular hyperechoic mass measuring 21×18×19 mm at the 12 o’clock position with features suggestive of a malignant lesion (Fig. 1). A needle core biopsy was performed and revealed an invasive tumor with some spindle cell differentiation and areas of necrosis, as shown in Figs. 2 and 3. No normal breast tissue was seen in the biopsy sample received. A provisional diagnosis of invasive ductal carcinoma with spindle cell differentiation was made, and further immunohistochemistry was requested to confirm the breast primary. The tumor cells were weakly positive for hormone receptors estrogen receptor and progesterone receptor and negative for human epidermal growth factor receptor 2.

Ultrasound of the right breast showing an irregular hyperechoic mass.
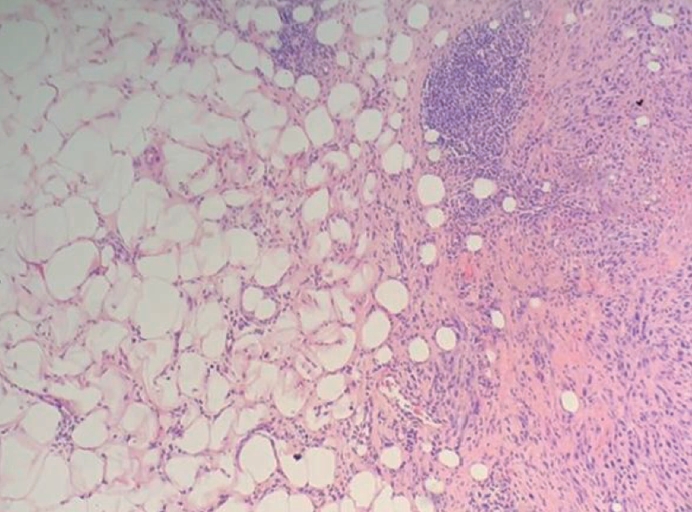
Core needle biopsy of the breast showed tumor with adjacent benign fibrofatty tissue.
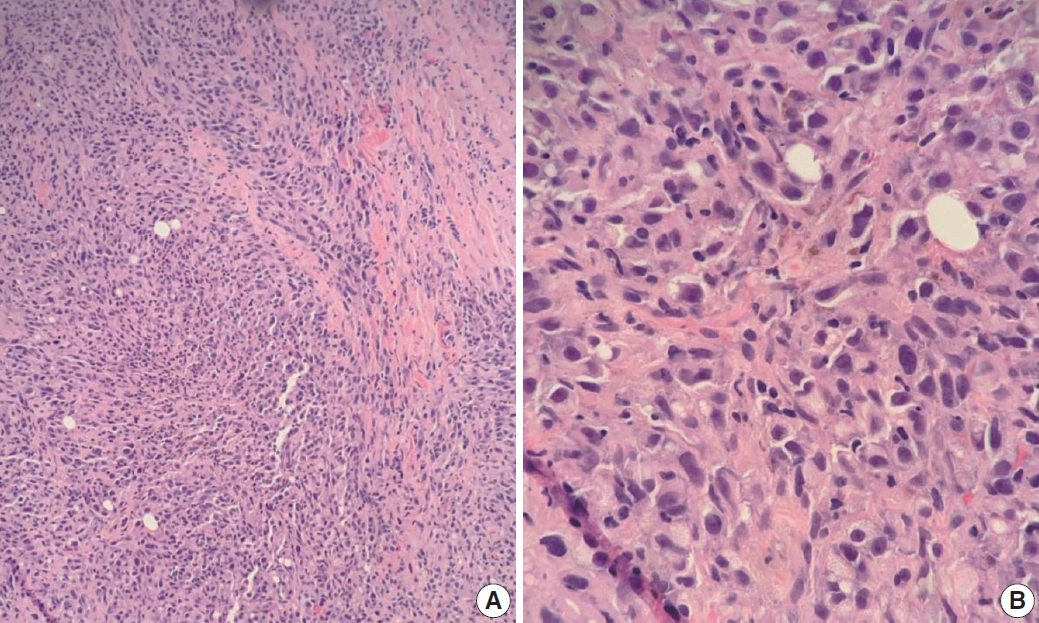
Core needle biopsy of the breast showed infiltrating tumor with spindle cell differentiation: (A) low power and (B) high power.
The case was discussed at a multidisciplinary team (MDT) meeting where more clinical information was provided. It was here revealed that the patient had a previous history of choroidal melanoma, and further immunohistochemistry was therefore performed to rule out a metastatic tumor.
As shown in Fig. 4, the tumor cells showed positive reaction for SOX10 (patchy), Melan-A, human melanoma black 45, and S100 (focal) and negative reaction for CK-AE1/AE3, CK5/6, CK-MNF16, thyroid transcription factor 1, CD31, p63, CD34, smooth muscle actin, desmin, and BCL2 immunostains. The overall findings were in keeping with metastatic malignant melanoma. BRAF codon 600 mutation testing was performed, and no mutation was identified. Later, head magnetic resonance imaging showed left posterior meningeal metastasis and a small enhancing lesion in the right occipital lobe, which were likely to be intracranial metastasis. The patient was referred to a specialist tumor center but refused further treatment.

Tumors cells showed positive reaction for (A) SOX10 (Patchy), (B) Melan-A, (C) human melanoma black 45, and (D) S100 (focal) immunostains.
DISCUSSION
Metastatic tumors of the breast are rare, but metastatic malignant melanomas comprise approximately 38.5% of metastatic tumors [5]. The histological features of the metastatic neoplasms may be non-specific or deceiving, particularly in cases of metastatic carcinoma and melanoma. The morphological diversity of melanomas and their presence at unusual sites make diagnosis even more difficult. Even with a history of non-mammary cancer, a breast lesion is most likely to represent a primary breast cancer [6]. Breast metastasis is generally a sign of disseminated disease, and systematic screening is needed to identify metastatic deposits elsewhere.
Malignant melanomas can be divided into primary or secondary. Primary malignant melanoma of the breast (PMMB) is a rare disease, accounting for 3%–5% of all melanomas and for less than 0.5% of malignant breast tumors. So far, 187 cases of PMMB have been reported in the literature [7].
A study by Zhou et al. [8] found that five out of nine cases of metastatic melanoma in the breast were misdiagnosed as primary poorly differentiated invasive breast carcinoma. Of these cases, four had a history of melanoma, one had none, and this history was not known to the reporting histopathologist in all five cases. In our case, a provisional diagnosis of primary breast tumor was made due to a lack of clinical information about the patient’s history of choroidal melanoma and the rarity of metastatic tumors in the breast.
The first case of breast metastasis from choroidal melanoma was reported by Chopra and Chandar in 1972 [9]. To the best of our knowledge, only five cases [9-13] have been published since, with one presenting in a male patient [11]. Most of the cases report breast metastasis as the first sign of metastatic disease, appearing between 50 and 60 months. In the present case, the patient presented with metastatic disease in the liver within 12 months and breast metastasis at 50 months, as in Table 1.

Comparison of all published cases of uveal melanoma including (age of patient, the sex, the age of the patient, the first presentation site of metastasis and the duration time in months between the primary site and breast metastasis) between period the 1972 till 2023
As per the literature, monosomy 3 is commonly found in most cases of uveal melanomas that metastasize to the liver [13], as seen in the current case. Breast metastasis from choroidal melanoma is extremely rare. Nevertheless, clinicians should be aware of this form of metastasis when treating patients with suspicious breast lesions and a history of choroidal melanoma. This case also emphasizes the importance of relevant clinical information being available to the reporting pathologist and further supports the vital role of MDT meetings and discussions in providing high quality patient care and avoiding erroneous diagnoses.
Notes
Ethics Statement
No patient consent was needed for publication as patient details were completely anonymised (neither the patient nor anyone else could identify the published information).
Availability of Data and Material
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Code Availability
Not applicable.
Author Contributions
Conceptualization: LA, ST. Data curation: LA, VM, ST. Formal analysis: LA, VM, ST. Investigation: LA, VM, NN, ST. Methodology: LA, VM, ST. Project administration: LA. Resources: LA. Supervision: LA, VM, ST. Validation: LA, VM, ST. Visualization: LA, VM, ST. Writing—original draft: LA, VM, ST. Writing—review & editing: LA, VM, NN, ST. Approval of final manuscript: all authors.
Conflicts of Interest
The authors declare that they have no potential conflicts of interest.
Funding Statement
No funding to declare.