Myxoid Solitary Fibrous Tumor of the Central Nervous System
Article information
Solitary fibrous tumors (SFTs) most commonly occur in the pleura, but may also occur in the central nervous system (CNS). Among the numerous cases of CNS SFT that have been reported, totaling to more than 220 cases, the myxoid SFT of the CNS has been the least recognized and most misleading subtype.1 Differential diagnosis from chordoid or myxo-chordoid meningioma, myxoid peripheral nerve sheath tumor, metastatic or primary low-grade fibromyxoid sarcoma, primary intracranial myxoma, and metastatic tumor from a cardiac primary tumor is therefore necessary. Here, we present a case of a myxoid SFT located in the tentorium cerebelli. A 45-year-old woman presented with headache, general weakness, and impaired vision. A magnetic resonance imaging scan revealed a lunulating, contoured, enhancing mass measuring 7.0×6.0×2.0 cm with hemorrhagic foci, located in the right posterior parietal and temporooccipital convexities. Under the diagnosis of meningioma, open craniotomy, right parietotemporooccipital, and subtotal tumor removal was performed.
Upon observation, many firm, rubbery, and bosselated tumor fragments, tan-white in color, were identified. The cut surface was relatively homogeneous, with a whitish fibrotic appearance and softer areas of gelatinous myxoid change, approximately 50%. Necrotic areas were not observed. Microscopic examination revealed a predominantly hypocellular area in the myxoid stroma, intervening with foci of a morphologically typical, densely cellular SFT with spindle cells and collagenous stroma (Fig. 1). In the hypocellular and myxoid areas, a proliferation of cytologically bland spindled cells was randomly arranged in a loose myxoid matrix, forming interconnecting strands, and resulting in degeneration. The neoplastic cells had oval to elongated nuclei, with evenly distributed chromatin, inconspicuous nucleoli, and scant pale cytoplasm. Immunohistochemically, the tumor cells showed a strong expression of CD34, vimentin, Bcl2 and CD99, but were negative for epithelial membrane antigen (EMA), pan-cytokeratin, and glial fibrillary acidic protein (GFAP). The Ki-67 labeling index was lower than 4%. On the basis of these findings, the final diagnosis was myxoid SFT.
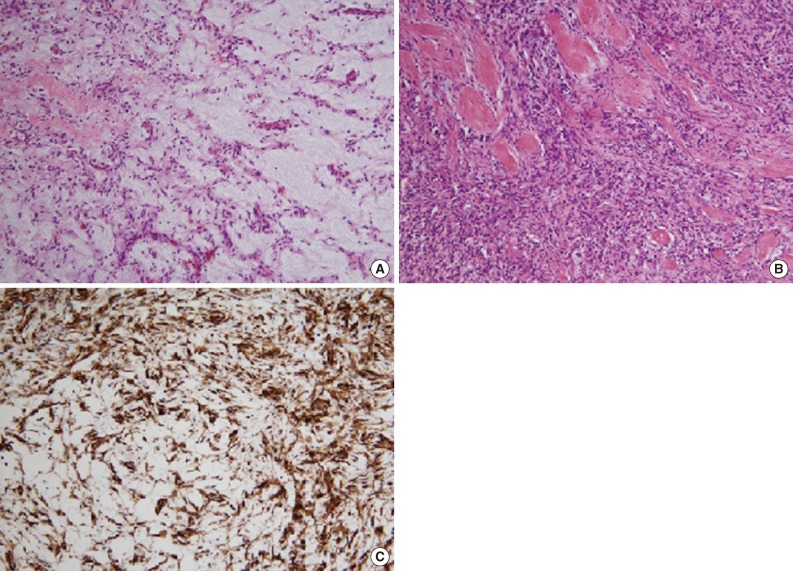
Histologic findings. Myxoid stroma with focal ropy collagen in a rich vascularized tumor (A), moderately cellular area exhibiting spindle cells and collagenous stroma (B), and strong immunoreactivity for CD34 (C).
Myxoid SFT of the CNS is an extremely rare tumor and differential diagnosis may be difficult to achieve owing to confusion with several other myxoid spindle cell neoplasms. Indeed, myxoid SFT of the CNS must be differentiated from chordoid or myxo-chordoid meningioma, myxoid peripheral nerve sheath tumor, metastatic or primary low-grade fibromyxoid sarcoma, primary intracranial myxoma, meningeal hemangiopericytoma and metastatic tumor from a cardiac primary.
Immunohistochemistry has proven to be a useful tool in attaining an accurate diagnosis. SFT of the CNS commonly shows strong positivity for CD34, Bcl2, and vimentin, but is negative for S-100 protein, GFAP, and EMA. Negativity for S-100 rules out chordoid or myxo-chordoid meningioma (vimentin+/EMA+/CD34+/S-100-), myxoid peripheral nerve sheath tumor (vimentin+/S-100+/EMA-/CD34-), metastatic or primary low-grade fibromyxoid sarcoma, and primary intracranial myxoma. Positivity for CD34 and Bcl2 may rule out the meningeal hemangiopericytoma (vimentin+/EMA-/CD34-/Bcl2-).2 Through clinical correlation, metastatic cardiac myxoma may be easily suspected.
The histogenesis of SFT is still unclear; however, tumor cells were shown to share similar histological features with fibroblasts. Microscopically, there are 3 common elements that appear in SFTs: spindle cells, a dense collagenous matrix, and prominent blood vessels.1 Spindle cells have oval nuclei with scant cytoplasm, and the cell borders are unclear. They may arrange into fascicles with no specific direction, creating a swirling pattern. The collagenous area is variable in size, and takes the form of ropy collagen. Cell density also varies, with hypercellular and hypocellular areas.3 Our case also shows a predominantly hypocellular area with myxoid stroma, and a hypercellular area with collagenous stroma. When fibrous tumors with myxoid nature involve the CNS, proper immunostaining and histologic differentiation should be done for differential diagnosis.
Notes
No potential conflict of interest relevant to this article was reported.