Renal Histologic Parameters Influencing Postoperative Renal Function in Renal Cell Carcinoma Patients
Article information
Abstract
Background
Pre-existing non-neoplastic renal diseases or lesions may influence patient renal function after tumor removal. However, its description is often neglected or omitted in pathologic reports. To determine the incidence and clinical significance of non-neoplastic lesions, we retrospectively examined renal tissues obtained during 85 radical nephrectomies for renal cell carcinoma.
Methods
One paraffin-embedded tissue block from each case containing a sufficient amount of non-tumorous renal parenchyma was cut and processed with hematoxylin and eosin and periodic acid-Schiff methods. Non-neoplastic lesions of each histological compartment were semi-quantitatively and quantitatively evaluated.
Results
Among the various histologic lesions found, tubular atrophy, arterial intimal thickening, and glomerulosclerosis were the most common (94.1%, 91.8%, and 88.2%, respectively). Glomerulosclerosis correlated with estimated glomerular filtration rate at the time of surgery, as well as at 1- and 5-years post-surgery (p=.0071), but tubulointerstitial fibrosis or arterial fibrous intimal thickening did not. Post-hoc analysis revealed that glomerulosclerosis of more than 20% predicted post-operative renal function. However, its significance disappeared when gender and age were considered.
Conclusions
In conclusion, non-neoplastic lesions, especially with regard to glomerulosclerosis percentage, should be described in pathology reports to provide additional information on renal function decline.
In the histologic evaluation of nephrectomy specimens containing renal cell carcinoma (RCC), pathologists describe tumor size, extent, and histology, including grade, tumor cell type, nuclear grade, and the presence and proportion of necrosis or sarcomatoid changes. However, few surgical pathologists describe abnormal findings in non-neoplastic renal tissue submitted along with the tumor.
In RCC patients, renal parenchyma remaining in situ after surgery may not be as healthy as expected. The prevalence of chronic kidney disease was reported to be as high as 26% in one cohort study of RCC patients prior to nephrectomy.1,2 The incidence of diabetes mellitus, which negatively impacts renal function, is higher in RCC patients.3,4 Bijol et al.5 reported that renal histologic findings were unremarkable in only 10% of 110 patients with tumor nephrectomy and patients with severe pathologic findings showed significantly increased serum creatinine levels six months after surgery. In that regard, patients who previously underwent radical nephrectomy are at greater risk for chronic kidney and cardiovascular diseases than those who underwent partial nephrectomy2,6,7 because nephrons cannot repopulate after they are severely injured or removed.
In this study, we explored the prevalence of non-neoplastic kidney lesions in RCC patients and searched for histologic factors influencing renal function at surgery and one and five years postsurgery in radical nephrectomy specimens removed for RCC at our institution.
MATERIALS AND METHODS
Case selection
We consecutively screened entire glass slides of 105 radical nephrectomy specimens diagnosed with RCC from the archives of the Pathology Department, that were collected between January 2000 and December 2007. From among these, cases containing sufficient nontumorous area were initially selected. Tissue sufficiency was defined as the presence of renal parenchyma that contained more than 50 glomeruli located at least 5-mm from the tumor tissue to avoid tumor effects. Electronic medical charts were reviewed to exclude cases with other pre-existing or concurrent neoplasms (except for the presence of hypertension or diabetes). A total of 85 cases were selected for the final study group. The study was approved by the Institutional Review of Boards of our institution.
Histologic assessment
One paraffin tissue block was retrieved for each case fulfilling the definition of tissue sufficiency described above. Sections were cut 4-µm thick and stained with hematoxylin and eosin and periodic acid-Schiff methods. The histologic review was performed without knowledge of clinical information (by M.J.K. and B.J.L.). Non-neoplastic lesions in glomerular, tubular, interstitial, and vascular compartments were evaluated quantitatively and semi-quantitatively. The percentage of globally and segmentally sclerosed glomeruli and the presence of glomerular hyalinosis were recorded. The extent of global glomerulosclerosis was graded as follows: grade 0, no global glomerulosclerosis; grade 1, global glomerulosclerosis <10%; grade 2, global glomerulosclerosis from 11% to 20%; and grade 3, global glomerulosclerosis >20%. Tubular atrophy, interstitial fibrosis, interstitial inflammation, and arteriolar hyalinosis were semi-quantitatively graded from 0 to 3 according to the Banff classification.8,9 The presence of nephrocalcinosis was also recorded.
Arteries were evaluated in two ways. First, arterial intima fibrous thickening was graded from 0 to 3 as follows: grade 0, no sub-intimal fibrosis; grade 1, mild sub-intimal sclerosis without significant occlusion of the arterial lumen (<10%); grade 2, moderate sub-intimal sclerosis with arterial lumen occlusion <50%; and grade 3, severe occlusion of >50% arterial lumen associated with thinning of the muscle layer and replacement by fibrous tissue.5 Secondly, intimal thickness and outer diameter (OD) were measured in arteries with an OD between 150 and 300 µm, and the ratio was expressed as a percentage of OD, which is referred to as R.10,11 The OD was measured along the shortest axis from one outer media to the other, excluding the adventitia. The intimal thickness was also measured along the shortest axis.
Diabetic nephropathy was diagnosed and classified according to Tervaert et al.12: class I, glomerulomegaly and isolated glomerular basement membrane thickening; class II, mesangial expansion; class III, nodular glomerulosclerosis; and class IV, advanced diabetic glomerulosclerosis.
Clinical data evaluation
Clinical information was obtained from patients' electronic charts in a blinded fashion. Gender and age at the time of surgery and the presence of hypertension or diabetes were recorded. Serum creatinine levels were obtained preoperatively, and one and five years after surgery in 69, 59, and 45 cases, respectively. Estimated glomerular filtration rate (eGFR) was calculated using the abbreviated Modification of Diet in Renal Disease equation: 175×plasma creatinine-1.154×age-0.203 (×0.742 if female).13 Chronic kidney disease was defined as eGFR<60 mL/min/1.73 m2.
Statistical analysis
Data was analysed using SAS ver. 9.2 (SAS Institute Inc., Cary, NC, USA). A linear mixed model was used to assess correlations among histologic findings, clinical features, and eGFR. Post-hoc analysis was used to assess the impact of global glomerulosclerosis on eGFR. We performed t-tests and chi-square tests to compare features between genders. Differences were considered statistically significant at p<.05.
RESULTS
Patient characteristics
The study group included 57 males (67.1%) and 28 females (32.9%). The mean age was 55.4 years (range, 31 to 75 years). Stages of RCC at diagnosis for T1, T2, and T3 were 56 cases (65.9%), 15 cases (17.6%), and 14 cases (16.5%), respectively. Hypertension was diagnosed before surgery in 26 patients and after surgery in six patients. Diabetes was diagnosed before surgery in seven patients and after surgery in three patients. Six patients (7.1%) had both hypertension and diabetes at the time of operation. Preoperative eGFR was less than 60 mL/min/1.73 m2 in 12 cases.
Non-neoplastic pathologic findings
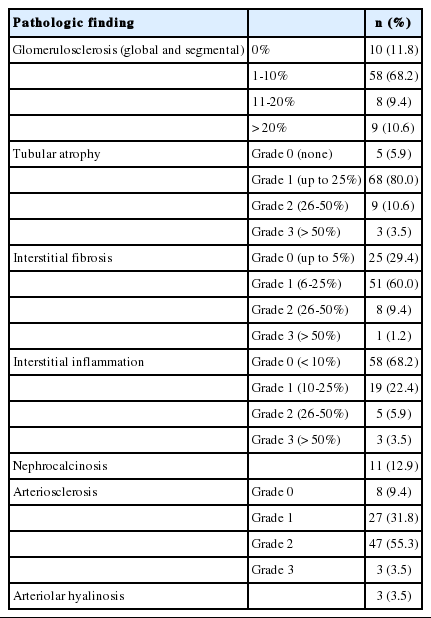
Various non-neoplastic lesions were observed in the renal parenchyma (Table 1). The most common findings were tubular atrophy, arteriosclerosis, and glomerulosclerosis, which were present in 94.1%, 90.6%, and 88.2%, respectively.
Non-neoplastic pathologic findings
The percentage of glomerulosclerosis was >10% in 17 cases (20.0%). Focal segmental glomerular sclerosis was observed in 10 cases (11.8%) and associated with hyalinosis in three cases. Enlarged glomeruli greater than 250 µm in Bowman's diameter were frequently found in the cortex of four cases (4.7%). Tubular atrophy and interstitial fibrosis involving more than 25% of the cortical area (grades 2 and 3) were present in 14.1% and 10.6% of cases, respectively. Interstitial inflammation occupying more than 25% of the cortical interstitium was observed in 9.4% of patients. Arteriosclerosis was moderate to severe in 58.8% of the cases. The ratio of arterial intimal thickness to the arterial wall, revealed as R, in 150- to 300-µm arteries was 12:43. Arteriolar hyalinosis was present in three cases. Chronic pyelonephritis was observed in four cases, revealing focal destructive tubular atrophy, interstitial inflammation, and interstitial fibrosis. Small bluish calcium deposits were observed in the renal inner medulla in 11 cases. Diabetic nephropathy was diagnosed in two cases, while advanced nodular glomerulosclerosis (class III) and an early lesion (class I) were each noted in one case.
Correlation of histological parameters with postoperative renal function
Among the original 85 cases, 69, 59, and 45 had preoperative data and 1- and 5-year follow-up data, respectively. Chronic kidney disease was present in 12 cases preoperatively and 21 cases five years after surgery. Twenty cases were lost to follow-up after surgery. Of the remaining cases, we could find a record of death in three cases with stage T1b at the time of surgery. Two cases died of cancer with distant metastasis at seven and 10 years after nephrectomy. One case died of newly developed breast cancer eight years after radical nephrectomy.
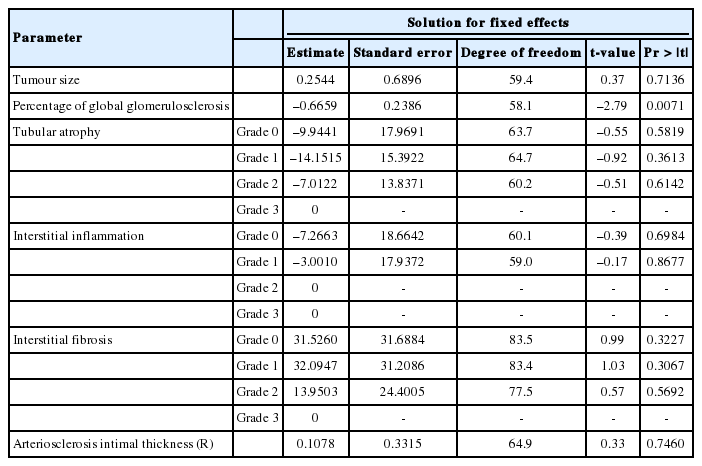
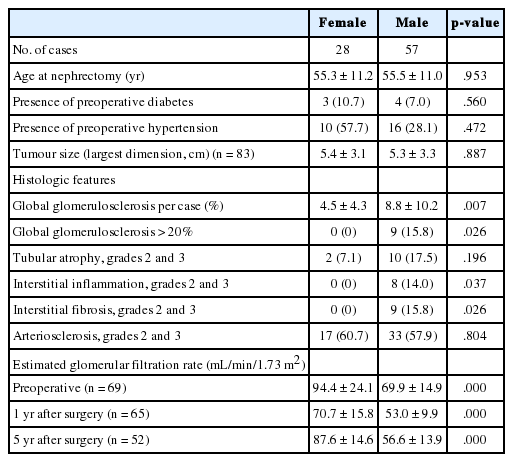
The linear mixed model was applied to examine histologic factors that might predict eGFR at surgery and one and five years after radical nephrectomy. Among these, only the percentage of global glomerulosclerosis was significantly correlated with eGFR. Global glomerulosclerosis >20% was significant by post-hoc analysis. Tumor size and other histologic parameters, including the grades of tubular atrophy, interstitial inflammation, interstitial fibrosis, arteriosclerosis, and small arterial intimal thickness (R) were not correlated with eGFR (Table 2). Nine patients (10.6%) had glomerulosclerosis >20%. They were all males with an average age of 61.7 years (median, 65 years). Six of them had diabetes or hypertension before surgery. Except for one case, they also had moderate to severe degrees of arteriosclerosis. Excluding two cases without available eGFR values, four of the seven cases had chronic renal disease defined by eGFR<60 mL/min/1.73 m2 at the time of surgery (cases 1, 3, 6, and 9). In the remaining three cases, two cases (cases 2 and 5) progressed to chronic renal disease one year after surgery (Table 3). When histologic features were compared between genders, males showed significantly more severe renal histologic injuries than females. Preoperative and postoperative eGFR values were significantly lower in males than in females (Table 4). Females had a 22-fold lower risk of decreased eGFR compared to males. Consequently, in the analytic model including both clinical and histologic parameters, age and gender were significantly correlated with eGFR (p=.0038 and p<.001, respectively), but glomerulosclerosis was not (p=.0964).
The impact of pathologic findings on eGFR

Clinicopathologic features of patients with global glomerulosclerosis of more than 20%
The comparison of clinical and histologic features between genders
DISCUSSION
Recently published renal cancer checklists recommend that abnormal histologic findings in non-neoplastic kidney be reported.14 In practice, however, concurrent non-neoplastic lesions/diseases are often neglected or omitted in pathologic reports. In a review of our original surgical pathology reports, only seven cases (8.2%) had records of non-neoplastic findings. The major reason for omission is that pathologists probably consider the renal parenchyma relatively well preserved or with minimal alterations in most cases. However, RCC patients are older and have a high prevalence of hypertension and diabetes, which may negatively impact postoperative renal function.15,16 Although partial nephrectomy is advocated, especially in patients with hypertension or diabetes,17 radical or total nephrectomy is still a major surgical procedure for RCC. Nonetheless, patient survival rate after surgery has progressively increased as tumors are being detected early, and also as new therapeutic target drugs are used for advanced cases.18 Obesity and hyperlipidemia are also frequently found in older patients and may jeopardize renal function as they live longer. In that regard, nephrectomy tissue provides a good opportunity to examine the non-neoplastic renal parenchyma to obtain information on the histologic factors influencing postoperative renal function.
Chronic kidney disease was not rare in this population. It was present in 17.4% preoperatively and its proportion increased to 46.7% five years after surgery. Among the histologic parameters assessed, only global glomerulosclerosis correlated with eGFR at one and five years postsurgery. Global glomerulosclerosis >20% was significant by post-hoc analysis. Six of the seven patients with >20% glomerulosclerosis had eGFR values <60 mL/min/1.73 m2 at one year after surgery. Two-thirds of them had other clinical risk factors that could affect renal function. However, the presence of hypertension and diabetes did not correlate with eGFR (p=.705 and p=.515, respectively).
Although glomerulosclerosis was correlated with eGFR, its significance disappeared when age and gender were considered. Gender was the strongest factor influencing eGFR (p<.001). Preoperative and postoperative eGFR values were significantly higher in females, likely due to the higher percentages of glomerulosclerosis, interstitial inflammation, and fibrosis in males (Table 4). This gender difference may be attributable to sex hormones. Estrogen has been shown to protect renal endothelial barrier function in vitro and in vivo.19 Estrogen exerts beneficial effects on the kidney by decreasing renin levels, angiotensin-converting enzyme activity, and aldosterone production.20 Age also correlated with declining eGFR. According to the formula (age/2)-10,21 nine cases presented glomerulosclerosis over the age limit. To our surprise, all patients with >20% glomerulosclerosis were male and also had glomerulosclerosis percentages over the age limit; these overlaps might obscure the effects of glomerulosclerosis in the study results.
Contrary to our hypothesis, tubulointerstitial fibrosis or arteriosclerosis did not correlate with eGFR. Interstitial fibrosis was moderate to severe in 10.6% and one-third of cases were associated with >20% glomerulosclerosis. Cases with moderate to severe arterial intimal thickening were more frequently observed and associated with hypertension, but did not correlate with renal histology either. We hypothesized that sampling error might be a major factor explaining for discrepancy with other studies.5 Although we set a point of 5-mm from the tumor margin to exclude tumoral effects, it is not clear whether 5-mm is a safe limit, regardless of tumor size or associated conditions. In a study of hepatocellular carcinoma, parenchyma within 10-mm of tumor tissue still showed significant histologic changes related to the tumor.22 There has been no consensus on the size of specimen sufficient for the evaluation. We selected cases that contained more than 50 glomeruli, but tissue composition was variable. Some cases were composed of exclusively superficial cortical tissue, which showed subcapsular fibrosis. Vascular lesions were frequently focal and segmental. Since we graded vascular wall thickening in the mostly affected arteries rather than according to average wall thickness, the grade may not represent the fibrotic areas affected by the vessel. Sampling more tissue and examining larger areas may reduce some of the histologic discrepancies.
Diabetic nephropathy is the most common cause of end-stage renal disease in Korea.23 Although diabetes is reported to be frequent in RCC patients, only seven patients were diagnosed with diabetes before surgery, and just two of them showed morphologic features of diabetic nephropathy: one exhibited nodular glomerulosclerosis (class III) and the other only showed glomerulomegaly (class I). In addition, glomerulomegaly was present in two cases without a history of diabetes at the time of surgery. We suspected these two cases as having early diabetic nephropathy, as they were diagnosed with diabetes during follow-up. Nephromegaly, including glomeruli and tubules, is an early feature of diabetic nephropathy and may appear even before the clinical recognition of glucose intolerance. However, clinicopathologic correlation is necessary because glomerulomegaly may develop in obesity24 as a secondary adaptation or a congenitally low number of nephrons.25 Nephrocalcinosis was not rare in our study, but calcified lesions were not extensive and had no specific causes.
Our study has several limitations. It is a retrospective study with a relatively small number of cases. Tissue sampling was not standardized, which resulted in size variation. Clinical work-up was not complete in several cases. Another limitation is the method used to evaluate vascular wall thickness. We did not measure the thickness of arteries of all calibers. As we measured the thickness of vessels with ODs of 150 to 300 µm, we might have missed histologic changes in smaller resistance vessels. However, arteriolar hyalinosis was rare, and glomerulosclerosis was well correlated with eGFR. Finally, it is not clear whether age and gender factors are more important than histologic factors. We considered that the small sample size might have obscured the effects of glomerulosclerosis. A larger prospective study may be needed to answer this question.
In summary, non-neoplastic lesions are not rare in radical nephrectomy specimens. Non-neoplastic lesions and the percentages of glomerulosclerosis should be described in surgical pathology reports to provide additional information on post-operative renal functional decline.
Notes
No potential conflict of interest relevant to this article was reported.