Mediastinal Thymolipoma with Striated Myoid Cells: Report of a Peculiar Case
Article information
Thymolipoma is a rare anterior mediastinal tumor composed of mature adipose tissue and benign thymic tissue, and is a benign neoplasm for which complete surgical excision is curative.1 Literature has reported that the thymic parenchyma of thymolipoma exceptionally contain myoid cells that are immunoreactive for desmin, muscle-specific actin and myoglobin.2,3 Herein, we describe a very rare case of thymolipoma with myoid cells. To the best of our knowledge, this is the sixth case of thymolipoma containing striated myoid cells in the English literature since 1972.
CASE REPORT
A 54-year-old man had a large asymptomatic anterior mediastinal mass incidentally discovered by chest radiograph during a regular health check-up. He had no history of autoimmune diseases including myasthenia gravis, aplastic anemia, hypogammaglobulinemia, lichen planus, or Graves' disease. A computed tomography scan of the chest demonstrated a large mediastinal mass consisting of a mixture of fat and soft tissue contents, radiologically suggesting thymolipoma (Fig. 1).
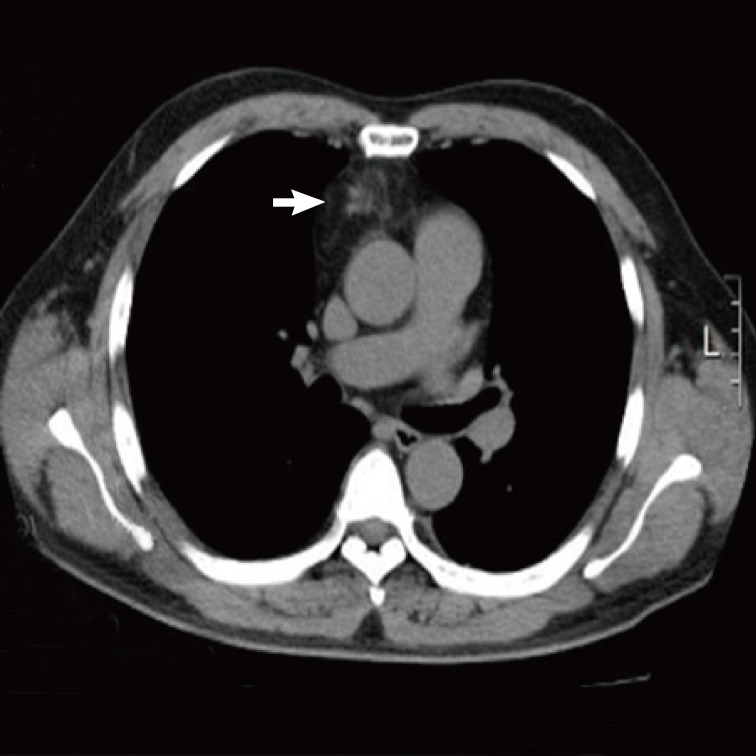
A computed tomography scan of the chest demonstrates a large mediastinal mass (white arrow) consisting of a mixture of fat and soft tissue contents and suggesting thymolipoma.
The tumor was surgically removed. Grossly, it was fairly wellcircumscribed by a thin fibrous capsule, and measured 12.0×10.0×3.5 cm. The outer surface was soft, yellow fatty tumor with focal solid areas (Fig. 2). Histologically, the mediastinal mass was characterized by the presence of abundant mature adipose tissue admixed with areas containing remnants of thymic tissue (Fig. 3A). The thymic tissue component varied from strands of atrophic thymic epithelium to large areas containing thymic parenchyma with medullary epithelial hyperplasia (Fig. 3B, C). In areas, the tumor showed a frequent occurrence of polygonal, striated myoid cells with abundant eosinophilic cytoplasm (Fig. 3D). These cells showed positive immunoreaction for desmin (1:200, clone D33, Dako, Glostrup, Denmark) and myoglobin (1:800, RB-9068-R7, Thermo, Fremont, CA, USA) in immunohistochemical study (Fig. 3E, F), but negative reaction for alpha smooth muscle actin (1:400, Dako). The myoid cells also lacked cytological atypia and mitotic figures.
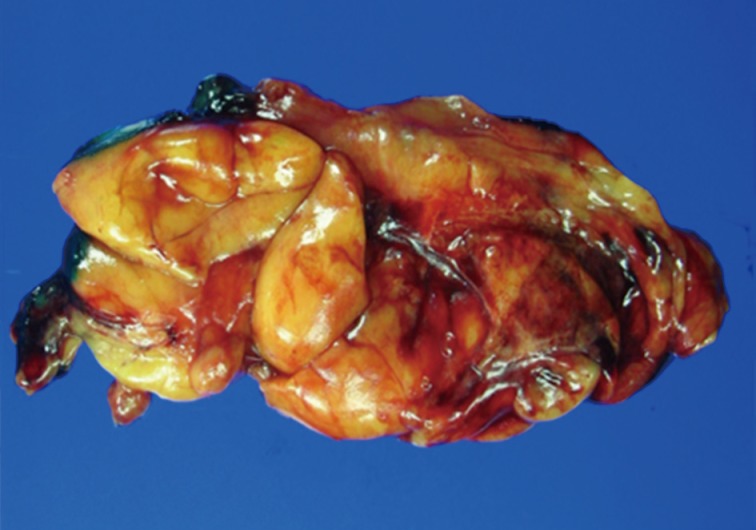
Grossly, the mass is a fairly well-circumscribed, soft, yellow fatty tumor with a focal solid area, measuring 12.0×10.0×3.5 cm.
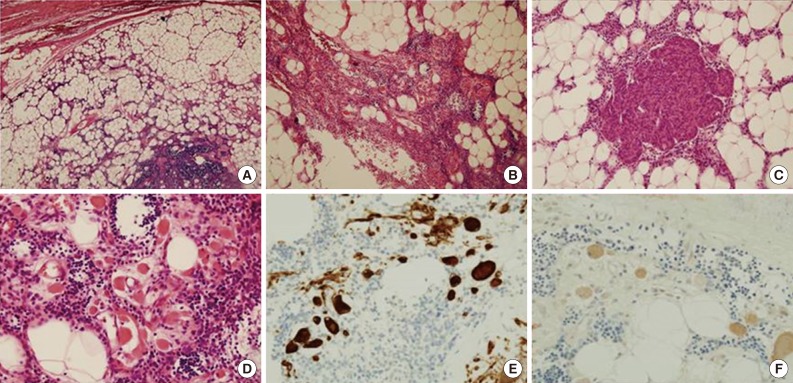
(A) The mass shows abundant mature adipose tissue admixed with areas containing remnants of thymic tissue. (B, C) The thymic tissue component varies from strands of atrophic thymic epithelium to large areas containing thymic parenchyma with medullary epithelial hyperplasia. (D) The tumor shows a frequent occurrence of polygonal striated myoid cells. (E, F) Myoid cells are immunoreactive for desmin (E) and myoglobin (F).
DISCUSSION
Thymolipomas are rare, benign mesenchymal tumors of the mediastinum that are often asymptomatic.1 Thymolipomas may adhere to the adjacent structures and displace organs within the chest cavity, but invasion into adjacent structures has not been documented in the literature. The encapsulated and lobular nature of thymolipomas and the lack of invasion into adjacent structures usually allow for a relatively uncomplicated surgical excision of the tumor. Regarding the unique appearance of myoid cells in the thymus, this tumor was originally thought to be confined only to the fetal and perinatal periods, but thymic striated myoid cells have now been described in healthy adults and adults with myasthenia gravis and thymic hyperplasia.3 However, there have been only five reported cases of adults with thymolipomas containing striated myoid cells.2,4-6
Immunohistochemically, the myoid cells of the present case revealed positivity for desmin and myoglobin but negativity for alpha smooth muscle actin. Smooth muscle actin is a ubiquitous contractile protein responsible for muscle cell motility. It is an extremely useful marker for the identification of smooth muscle cells, myofibroblasts, and myoepithelial cells. Desmin, a muscle-type intermediate filament, is found in cells of smooth and striated muscle and in a lesser amount in myofibroblasts. Therefore, it has been primarily used for the identification of smooth muscle and skeletal muscle tumors. Especially, positivity for desmin and negativity for actin may be a feature of a subset of cells of myofibroblastic appearance. However, the myoid cells of the present case also showed definite positive cytoplasmic staining for oxygen-binding protein myoglobin, which is apparently specific for striated (skeletal and myocardial) muscle and is, therefore, of utility for the identification of rhabdomyosarcomas and other tumors exhibiting skeletal muscle differentiation.7 Therefore, we conclude that thymic myoid cells demonstrate immunophenotypic features of skeletal muscle differentiation.
There are controversial theories concerning the histogenesis of thymic myoid cells: 1) derivation from the neural crest, 2) transformation from epithelial cells, and 3) originating from perithymic mesenchymal cells that become incorporated into the thymus.4 Regardless of origin, most thymic myoid cells, as in our cases that were identified by surgical excision, are benign, although their recognition as a benign entity may be difficult in limited biopsy material. Thymic myoid cells demonstrate immunophenotypic and ultrastructural features of skeletal muscle differentiation, which may be useful in their specific identification.2
The histologic differential diagnosis for thymolipomas includes thymic hyperplasia, thymic neoplasm including lipoma, extragonadal germ cell tumors or teratoma and well-differentiated liposarcoma.1 Thymic hyperplasia classically has unremarkable thymic architecture without the presence of abundant adipose tissue. The distinction between a lipoma and a predominantly fatty thymolipoma may be difficult. In the latter, extensive sectioning and immunohistochemical staining for cytokeratin may highlight any hidden thymic epithelial tissues in a thymolipoma. Teratomas commonly arise in the anterior mediastinum, are often associated with residual thymic tissue and may contain mature adipose tissue.4 Scattered myoid cells in thymic tumors, including thymolipomas, should not be confused with teratomatous elements of a germ cell tumor. Thymolipomas can be distinguished from teratomas by the absence of ectodermal tissues commonly associated with mature teratomas, such as skin and neuroglia. Anterior mediastinal liposarcomas have been described, and liposarcomas of thymic origin do exist. Mediastinal liposarcomas may grossly resemble benign thymolipomas and may be associated with thymic tissue. Thymolipomas can be distinguished from thymoliposarcomas by the absence of prominent areas of sclerosis, characteristic lipoblasts, scattered atypical stromal cells and other features of classic liposarcoma. Thymoliposarcomas containing striated myoid cells have not been described to date.
To our knowledge, this is the sixth reported case in the English literature of thymolipoma containing striated myoid cells. In the present case, myoid cells were observed, but there were no symptoms of myasthenia gravis. The myoid cells in thymolipoma were identified by immunophenotype and demonstrated a benign morphology. Thymolipomas containing myoid cells should be differentiated from other thymic neoplasms, including germ cell tumors and liposarcomas. Studies on more of these cases are necessary to elucidate the relationship between thymolipoma and myoid cells. Thus, exhaustive testing of all thymic neoplasms is vital for classifying these tumors and providing patients with proper treatment.
Acknowledgments
This work was supported for two years by Pusan National University Research Grant.
Notes
No potential conflict of interest relevant to this article was reported.