Proto-oncogene Pokemon in thyroid cancer: a potential promoter of tumorigenesis in papillary thyroid carcinoma
Article information

Abstract
Background
Pokemon is an oncogenic transcription regulator that plays a critical role in cellular differentiation. Although it has been found to be overexpressed in several types of cancer involving different organs, its role in thyroid gland has yet to be reported. The objective of this study was to evaluate the expression of Pokemon in papillary thyroid carcinoma (PTC) based on clinicopathological parameters.
Methods
Tissue microarray samples derived from patients with PTC or benign thyroid disease were used to evaluate Pokemon expression based on immunohistochemical analysis. Correlations of its expression with various clinicopathological parameters were then analyzed.
Results
Pokemon expression was observed in 22.0% of thyroid follicular cells from the normal group, 44.0% from the group with benign thyroid diseases, and 92.1% from the group with PTC (p < .001). The intensity of Pokemon expression was markedly higher in the PTC group. Pokemon expression level and PTC tumor size showed an inverse correlation. T1a tumors showed strong expression levels of Pokemon. However, larger tumors showed weak expression (p = .006).
Conclusions
Pokemon expression is associated with tumorigenesis of PTC, with expression showing an inverse correlation with PTC tumor size. This might be related to the negative regulation of aerobic glycolysis by Pokemon.
Thyroid cancer is the most common endocrine malignancy. It represents 1% of all malignancies [1]. Papillary thyroid carcinoma (PTC) is the most common cancer among these malignant tumors, accounting for about 85% of thyroid cancers. Patients with PTC have an excellent prognosis with a 10-year survival rate greater than 90% [1]. One single institutional long-term follow-up study in 2018 reported that 10-, 15-, and 20-year overall survival rates of PTC patients were 97%, 95%, and 90%, respectively [2]. However, some PTCs display aggressive features. Several clinicopathological parameters such as old age, large tumor size, presence of extrathyroidal extension, and cervical lymph node metastasis have been suggested as poor prognostic factors [3,4].
Recent studies have identified specific molecular alterations involved in the formation of PTC [5], including BRAF V600E mutations and changes in mitogen-activated protein kinase pathway, RAS mutations and changes in phosphoinositide 3 kinase-AKT (PI3K-AKT) pathway, RET/PTC rearrangement, PAX8/PPARγ rearrangement and changes in PTEN-activated PI3K-AKT pathway, and TRK rearrangements [5]. Pokemon (POK erythroid myeloid ontogenic factor), also known as ZBTB7a (zinc finger and BTB domain-containing protein 7a) or FBI-1 (factor binding inducer of short transcripts of human immunodeficiency virus type 1), is a transcriptional regulator that belongs to the POK protein family. It plays a critical role in cellular differentiation [6,7]. Pokemon protein is a transcriptional regulator of several genes. Pokemon can specifically repress the transcription of the tumor suppressor gene ARF via direct binding [6]. Genes such as RB1 [8], CDKN1A [9], nuclear factor-kB responsive genes [10], survivin [11], CDK2 and E2F4 [12], ADH5/FDH [13], and FASN [14] are also regulated by Pokemon. Dysfunctional POK proteins can cause disorders in cellular development and trigger oncogenic processes [6]. Overexpression of Pokemon has been detected in several types of cancer, such as breast cancer, liver cancer, prostate cancer, and malignant glioma [6,11,15–17]. However, the carcinogenic effect of Pokemon overexpression in thyroid gland has yet to be reported. Thus, the objective of this study was to analyze the expression of Pokemon in PTC and evaluate correlations between Pokemon expression and clinicopathological parameters of PTC using tissue samples obtained from 90 cases of PTC and 25 cases of benign thyroid disease.
MATERIALS AND METHODS
Tissue specimens
We selected 90 cases of PTC and 25 cases of benign thyroid diseases such as nodular hyperplasia, follicular adenoma, Hashimoto’s thyroiditis, and Graves’ disease from archival cases in Kangbuk Samsung Hospital (Seoul, Republic of Korea). Controls included 68 normal thyroid tissues identified from selected cases. Tissues resected by surgeons were examined by pathologists before fixation in 10% neutral-buffered formalin for 12–24 hours, followed by thorough macroscopic evaluation and sectioning. After automatic tissue processing, sections were embedded in paraffin blocks. Four-micrometer-thick sections were cut from each formalin-fixed, paraffin-embedded (FFPE) tissue block using a rotary microtome, stained with hematoxylin and eosin, covered with a glass coverslip, followed by analysis and diagnosis by two board-certified pathologists. Clinical and pathological information were obtained from pathology reports and electrical medical information systems. Information collected included age, sex, multifocality, the greatest dimension of the tumor, presence of lymphovascular invasion, extrathyroidal extension, lymph node metastasis, number of metastatic lymph nodes, BRAF mutational status, and presence of background thyroiditis. One out of these 90 PTC patients was excluded from statistical analysis due to insufficient data (Table 1).

Clinicopathological parameters of subjects in the PTC group
Tissue microarray construction
Tissue microarray (TMA) blocks were constructed in following orders. Briefly, all hematoxylin and eosin-stained slides were reviewed and the two most representative tumor areas were marked on the corresponding FFPE tissue blocks. Two 2-mm-diameter tissue cores were obtained from each block and manually arrayed into recipient TMA blocks. Only one 2-mm-diameter tissue cores were obtained from blocks with largest tumor size less than 5 mm. The assembly was held in an X-Y position with a 1-mm increment between individual cores. Modified biopsy needle was used to bore holes in a recipient block with defined array cores and to transfer the cores into the recipient block. The percentage of tumor volume in each core was > 70%. Two TMA blocks were prepared for each case.
Immunohistochemistry
Immunohistochemical staining was performed using the Bond Polymer Refine Detection kit (Leica Biosystems, Newcastle upon Tyne, UK) in the Bond-Max automatic immunostainer (Leica Biosystems). ZBTB7A/Pokemon antibody (1:200, clone, Novus Biologicals, Littleton, CO, USA) was used as the primary antibody. Immunohistochemical slides were independently evaluated by two pathologists (SID and SWC). Discrepant cases were reviewed. Pokemon expression was interpreted as positive if the cell showed positivity in either the nucleus or the cytoplasm. The intensity of expression was defined as negative, weakly positive, or strongly positive (Fig. 1). Immunohistochemical expression (× 200) of Pokemon in thyroid tissues from normal (Fig. 1A–C), benign thyroid disease (Fig. 1D–F), and PTC (Fig. 1G–I) groups. Pokemon expression intensity is interpreted as negative (Fig. 1A, D, G), weakly positive (Fig. 1B, E, H), or strongly positive (Fig. 1C, F, I). It was determined using TMA cores of those with PTCs (n = 89) or benign thyroid diseases (n = 25). Pokemon expression intensity of normal thyroid tissue was determined in adjacent normal follicular cells where present, if the TMA core carried an identifiable portion of normal thyroid tissue (n = 68).
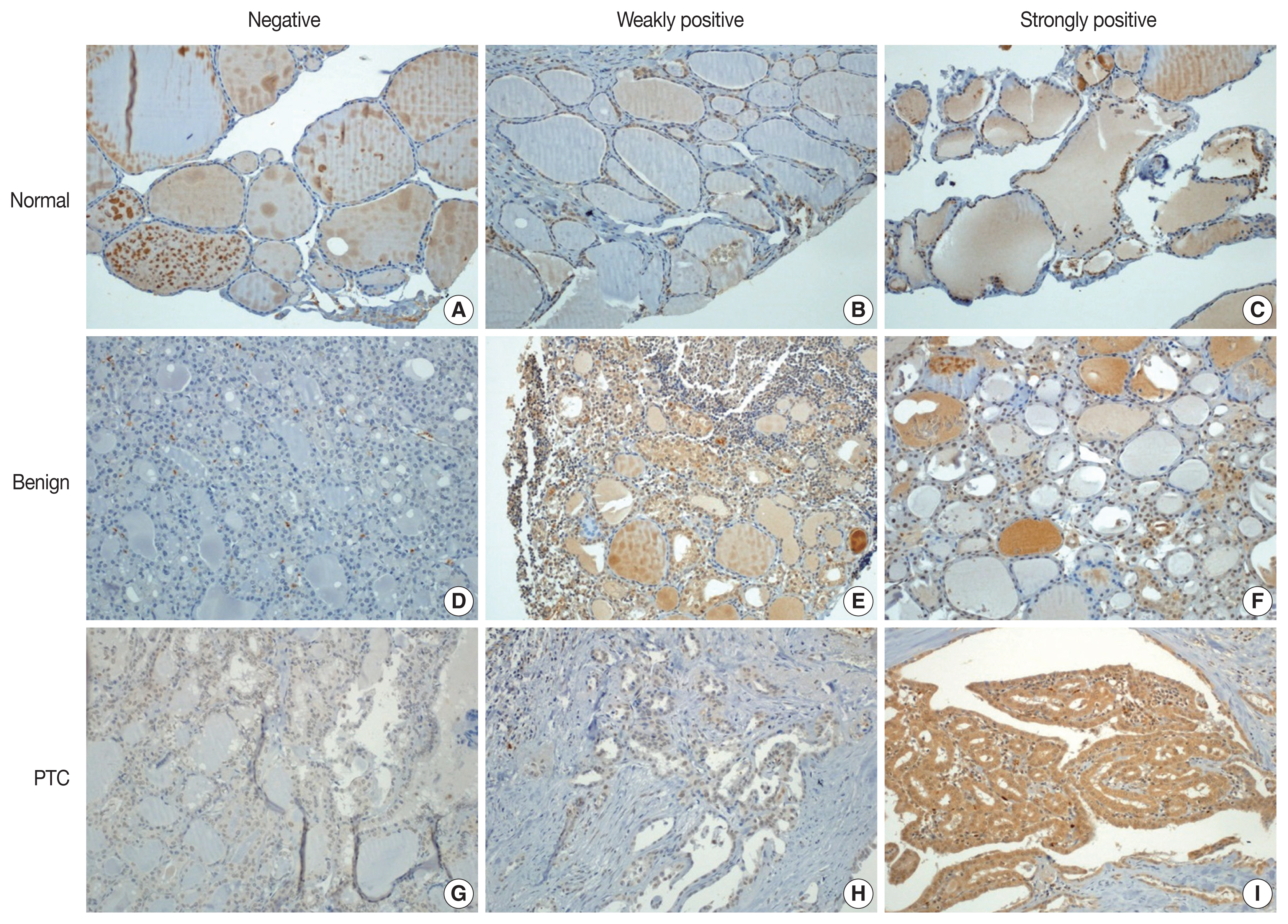
Immunohistochemical expression of Pokemon in thyroid tissues of normal (A–C), benign thyroid disease (D–F), and PTC (G–I) groups. Pokemon expression intensity is interpreted as negative (A, D, G), weakly positive (B, E, H), or strongly positive (C, F, I).
Detection of BRAF mutation
To detect BRAF V600E mutation, nucleic acids were isolated from FFPE tissues using a DNeasy Blood and Tissue Kit (Qiagen, Hilden, Germany). Isolated nucleic acids were mixed with a polymerase chain reaction (PCR) master mix using a Seeplex BRAF V600E ACE Detection Kit (Seegene, Seoul, Republic of Korea). These mixtures were then immediately transferred to a preheated thermal cycler for 15 minutes. PCR was carried out in a GeneAmp PCR System 9700 (Applied Biosystems, Foster City, CA, USA). The cycling amplification program consisted of 35 cycles of denaturation at 94°C for 30 seconds, annealing at 63°C for 30 seconds, and extension at 72°C for 1 minute. Amplified PCR products were loaded onto a 2% agarose gel and visualized with a SafeView Nucleic Acid Stain (Applied Biological Materials, Richmond, BC, Canada). The BRAF V600E mutation was detected using a Gel Documentation System (Bio-Rad Laboratories, Hercules, CA, USA).
Statistical analysis
Pearson’s Chi-square test was performed to compare Pokemon expression intensities in thyroid tissues of PTC, benign thyroid disease, and normal groups. It was also used to analyze associations between Pokemon expression intensity and clinicopathological characteristics. Clinical significance was determined using Kruskal-Wallis test (nonparametric method), linear-by-linear association test, and Pearson’s chi-square test. All statistical analyses were performed using SPSS for windows ver. 24.0 (IBM Corp., Armonk, NY, USA). Statistical significance was considered when p-value was less than .05.
Pathologic TNM staging
Pathologic TNM staging was referred to American Joint Committee on Cancer 8th edition of the Cancer Staging Manual for PTC. Pathologic T categories included the following: T1a, tumor ≤ 1 cm in the greatest dimension limited to the thyroid; T1b, tumor > 1 cm but ≤ 2 cm in the greatest dimension, limited to the thyroid; T2, tumor > 2 cm, but ≤ 4 cm in the greatest dimension, limited to thyroid; T3a, tumor > 4 cm limited to the thyroid; T3b, gross extrathyroidal extension invading only strap muscles (sternohyoid, sternothyroid, thyrohyoid, or omohyoid muscles) from a tumor of any size; and T4, gross extrathyroidal extension beyond strap muscles. Pathologic N categories included the following: N0, no evidence of locoregional lymph node metastasis; N0a, one or more cytologically or histologically confirmed benign lymph nodes; N1, metastasis to regional nodes; N1a, metastasis to level VI or VII (pretracheal, paratracheal, or prelaryngeal/Delphian, or upper mediastinal) lymph nodes; and N1b, metastasis to unilateral, bilateral, or contralateral lateral neck lymph nodes (levels I, II, III, IV, or V) or retropharyngeal lymph nodes.
RESULTS
With collected information shown in Table 1, Pokemon expression intensities in thyroid tissues of normal, benign thyroid disease, and PTC groups were determined (Table 2). Statistically significant (p < .001) differences in Pokemon expression positivity were observed between normal thyroid tissues (22.0%) and thyroid tissues from patients with benign thyroid disease (44.0%) or PTC (92.1%). Results of Pearson’s chi-square test for Pokemon expression intensity in normal, benign, and PTC groups are shown in Supplementary Tables S1–S3. The difference in Pokemon expression intensity between normal and benign thyroid disease groups was statistically significant (p = .035). The difference in Pokemon expression intensity between normal and PTC groups was also statistically significant (p < .001). Similarly, the difference in Pokemon expression intensity between benign thyroid disease and PTC was significant (p < .001).

Pokemon expression intensities in thyroid tissues of normal, benign thyroid disease, and PTC groups
Pokemon expression intensity in PTC showed significant correlations with tumor size and corresponding pathologic T category groups (Table 3). Reduced mean tumor size was significantly associated with stronger Pokemon expression intensity (p = .002). Tumor size and TNM stage were also significantly associated with Pokemon expression intensity. When the tumor size was divided into three groups by a separation point at 0.5 cm and 1 cm, a tumor size less than 0.5 cm was associated with Pokemon expression intensity stronger than 66%. However, increased tumor size was associated with less strong or no Pokemon expression intensity (p = .028). Tumor size categorized by conventional TNM staging, excluding T3b and T4 groups for gross extrathyroidal extension to and beyond strap muscles, showed evident negative concordance with Pokemon expression intensity (p = .010). T1a group was associated with expression greater than 66%, whereas groups T1b, T2, and T3a were collectively associated with no or weak expression (p = .006). Other clinicopathological parameters did not show any significant association with Pokemon expression intensity.
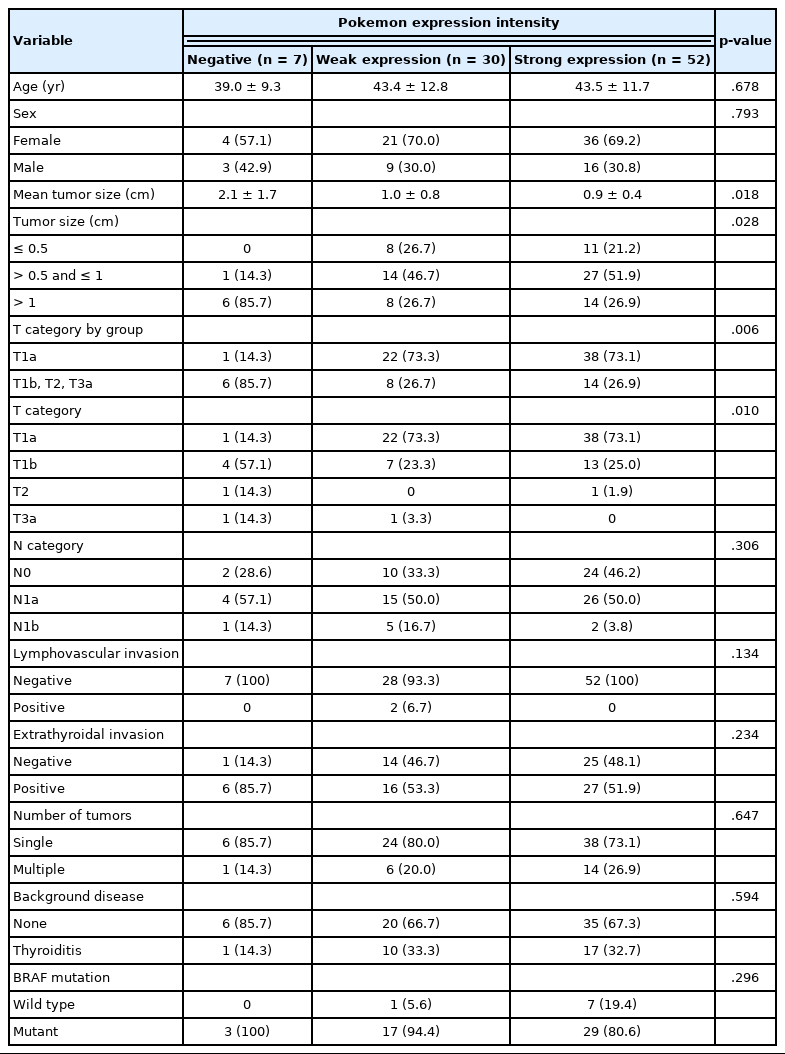
Correlations of Pokemon expression intensity with clinicopathological parameters in PTC
DISCUSSION
Pokemon can act as a genuine proto-oncogene in vivo [6]. It can repress the expression of tumor suppressor protein ARF [6]. ARF is a negative regulator of the E3 ubiquitin-protein ligase MDM2 which participates in the degradation of p53 via ubiquitin-dependent degradation by the proteasome. Reduced ARF levels can stimulate cell proliferation by decreasing the stability and activity of p53 via MDM2 [6]. Pokemon expression in malignancy is generally related to poor cancer outcome in various organs. It promotes tumorigenesis, acting as a pro-oncogene by repressing or enhancing the expression of genes involved in apoptosis, cell proliferation, and differentiation [18]. For example, Pokemon expression can promote breast cancer progression by up-regulating survivin expression [11]. In the nasopharynx, high Pokemon protein expression is closely associated with non-keratinizing nasopharyngeal carcinoma [19]. In the liver, suppression of Pokemon can impair the invasion of hepatocellular carcinoma (HCC) cells [20]. However, to the best of our knowledge, contribution of Pokemon to thyroid malignancy has yet to be reported.
Pokemon expression intensity showed a statistically significant (p = .035) difference between normal and benign thyroid disease groups in the present study. Although Pokemon expression was positive in 44% of patients with benign thyroid disease regardless of its expression intensity, it was more significantly (p < .001) associated with PTC than with benign thyroid disease (Table 2). Pokemon overexpression has also been observed in several malignancies, such as T and B cell lymphomas in transgenic mice model via direct binding of Pokemon and the tumor suppressor gene ARF [6], prostate carcinoma via increased Pokemon expression stimulated by epidermal growth factor [16], ovarian carcinomas of all four major histological types (serous, endometrioid, clear cell, and mucinous) via elevated RNA transcription [21], breast carcinoma by up-regulating survivin, a member of the inhibitor of apoptosis proteins [11]. However, the mechanism which Pokemon overexpression leads to tumorigenesis of PTC remains to be investigated.
When Pokemon expression intensity was compared according to mean PTC tumor size, stronger expression levels were observed in smaller tumors (0.9 ± 0.4 cm), whereas larger tumors (2.1 ± 1.7 cm) showed absent or weak expression. These inverse correlations were evident according to the T category of the tumor when T1a group was compared with the combined group of T1b, T2, and T3a (p = .006) (Table 3). These results were contrary to results of several previous studies of tumors involving various organs, where Pokemon expression was positively correlated with tumor size or T category of breast carcinomas [11], HCC [22], or non-small cell lung cancer [23]. These combined results of particularly strong Pokemon expression in small-sized tumors suggest that Pokemon might play an important role in malignant transformation of thyroid cells and in the early stage of PTC tumor formation, while it might have a diminished role as the tumor grows in size.
Such inverse correlation between Pokemon expression and tumor size has also been observed in oropharyngeal squamous cell carcinoma (OSCC) which shows a higher relative expression in smaller tumors (< 2 cm) and lower to no expression in larger tumors (≥ 4 cm) [18]. Although the distribution of Pokemon expression is lower in OSCC than in normal oral mucosa, Sartini et al. [18] have suggested that the downregulation of Pokemon might be related to tumor progression. Presumably, our results suggest such downregulation.
Aerobic glycolysis (the Warburg effect) is a hallmark of human cancer. It plays a crucial role in tumor growth [24]. Receptor tyrosine kinase/PI3K/AKT signaling and MYC act as pro-growth signaling factors that can upregulate aerobic glycolysis. However, Liu et al. [25] have reported that Pokemon, a proto-oncogene, unexpectedly can act as a tumor suppressor by directly binding to the promoter and repressing the transcription of genes responsible for glycolysis metabolism, such as GLUT3, PFKP, and PKM. As a result, a significant decrease in Pokemon copy number variation was observed in several types of human carcinoma in the late stage (N1, N2, N3, M1, stage IV) than in early stage (N0, M0, stage I), including esophageal carcinoma, bladder urothelial carcinoma, colorectal adenocarcinoma, lung squamous cell carcinoma, cutaneous melanoma, and low-grade glioma [25]. We believe that the mechanism underlying the inverse correlation between Pokemon expression and tumor size of PTC might be related to the unexpected negative regulation of aerobic glycolysis by Pokemon.
Regardless of its contrasting behavior in PTC, Pokemon itself is associated with malignant transformation of tumors in various organs. High levels of Pokemon expression in patients with early stages of PTC may potentially be used for screening and identifying malignancies involving other organs.
Our study was performed at a single institution with PTC cases retrieved from a two-year period, which invariably resulted in limitations involving the follow-up period of patients with PTC and their survival rates. A multi-institutional study with ethnic and racial diversity is needed to further investigate the effect of Pokemon on PTC. Larger patient groups might be needed to elucidate the effect of Pokemon on parameters showing statistical insignificance in the present study. A long-term survival study may provide further insight into the effect of Pokemon on long-term outcomes of PTC, one of the most common malignancies worldwide.
In summary, Pokemon overexpression (when compared to normal thyroid tissues) is associated with formation of PTC and benign thyroid diseases. A smaller PTC tumor shows stronger Pokemon overexpression, which supports the hypothesis that Pokemon overexpression can lead to tumorigenesis of PTC. However, a larger PTC tumor may be associated with Pokemon downregulation, which may be related to tumor progression. Targeting Pokemon in early stages could be effective in suppressing PTC formation and potentially facilitate treatment.
Supplementary Information
Notes
Supplementary Information
The Data Supplement is available with this article at https://doi.org/10.4132/jptm.2021.06.28.
Ethics Statement
All procedures performed in this study were approved by the Institutional Review Board at Kangbuk Samsung Hospital (IRB No. 2016-08-006-001) in accordance with the Helsinki Declaration as revised in 2013. The requirement of informed consent was waived due to its retrospective nature.
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
Code Availability
Not applicable.
Author Contributions
Conceptualization: SID, SWC. Data curation: KC, SID, SWC. Formal analysis: KC, SID, SWC. Investigation: KC, SID, SWC. Methodology: SID, SWC. Project administration: SID, KK, SWC. Resources: SID, SWC. Supervision: SID, KK, SWC, IGD, HJL, DHK, JHS. Validation: SID, SWC. Visualization: KC, SID, KK. Writing—original draft: KC, SID, KK. Writing—review & editing: KC, SID, KK. Approval of final manuscript: all authors.
Conflicts of Interest
The authors declare that they have no potential conflicts of interest.
Funding Statement
No funding to declare.