Fine Needle Aspiration Cytology of Warthin-like Papillary Thyroid Carcinoma: A Brief Case Report
Article information
The Warthin-like variant of papillary thyroid carcinoma (WL-PTC) was first introduced by Apel et al.1 in 1995 as an extremely rare subtype of papillary thyroid carcinoma (PTC) that is characterized by papillary architecture, lined by Hürthle cells, with classical cytologic features of PTC cells, and a heavy lymphocytic stroma of the papillary core. WL-PTC is now classified in the World Health Organization terminology as a special subtype of an oncocytic variant of PTC.2 Its histopathological features have been relatively well documented in cases that followed the first 13 that were described by Apel et al.1,2 However, the cytologic features of WL-PTC in fine needle aspiration cytology (FNAC) are described rather poorly and by only a few authors.3,4,5,6 Although Kim et al.7 have documented the cytologic features of an oncocytic variant of PTC in a Korean patient, FNAC of WL-PTC has not been reported in Korea.
FNAC is being used widely for initial diagnosis of thyroid lesions for a treatment plan decision. The first cytological picture of WL-PTC highly resembles that of benign lymphocyterich thyroid lesions such as Hashimoto's thyroiditis. Therefore, knowledge about key points in the differential cytological diagnosis is essential for an accurate diagnosis and appropriate treatment. Here, we present WL-PTC with FNAC for the first time in Korea in a teaching case involving liquid-based cytology (LBC) preparation in a 31-year-old woman.
CASE REPORT
A 31-year-old Korean woman was referred to the department of surgery with a hypoechoic solid nodule in the upper pole of her left thyroid that was found during a routine health checkup (Fig. 1A). The nodule measured 0.99×0.75 cm and was accompanied by microcalcifications. The remaining thyroid parenchyma was hypoechoic and heterogeneous, which suggested Hashimoto's thyroiditis. Thyroid function tests, serum calcium, and parathyroid hormone level were within normal ranges. An aspiration of the mass was performed with a 21-gauge needle, and an air-dried smear was stained using the Papanicolaou (Pap) method. Another smear was fixed in 95% alcohol and stained with hematoxylin and eosin (H&E). The remaining aspirates were fixed in SurePath (BD Diagnostics-Tripath BD Biosciences, Oxford, UK) liquid medium and processed according to LBC protocols. After the cytologic diagnosis was made, total thyroidectomy was performed (Fig. 1B).
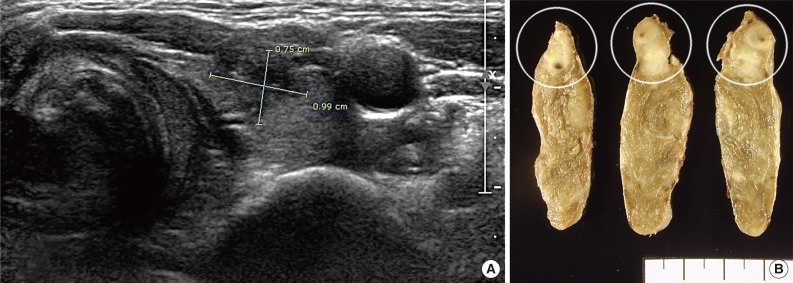
Ultrasonographic and gross findings. (A) A 0.99×0.75-cm-sized irregular hypoechoic nodule with calcification and spiculated margins is noted on the upper pole of the left lobe. (B) Grossly, the lesion is a poorly circumscribed, white, soft mass with fish-flesh appearance (circles). The remaining parenchyma shows diffuse, ill-defined, white, spotty nodules throughout the lobe.
Cytology using conventional smears stained either by Pap or by H&E demonstrated relatively low cellularity with mainly isolated follicular cells and some small irregular clusters on a lymphocyte-rich background (Fig. 2). The follicular cells displayed an abundant polygonal morphology and contained well-defined cytoplasm and centrally or eccentrically located, round to oval nuclei with fine chromatin and inconspicuous micronucleoli. The tumor cells showed many nuclear grooves and occasional intranuclear pseudoinclusions, which were highly suggestive of PTC. These cells were more evident in numbers on LBC than with conventional smears, although the intranuclear pseudoinclusions were less common and the lymphocytic background was absent.
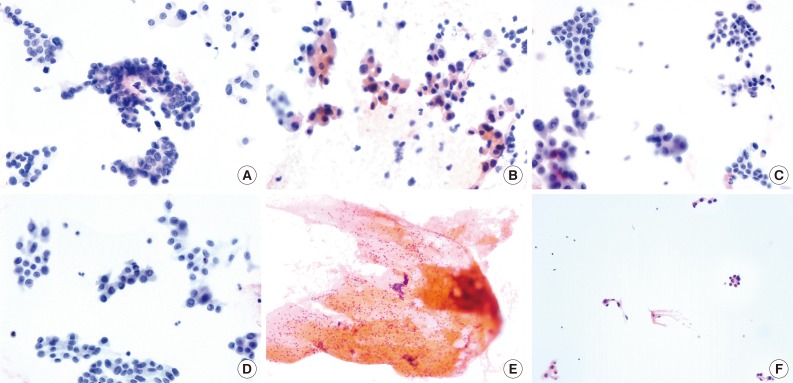
Cytological features according to methods and stains. The conventional smear shows many irregular and papillary clusters with typical cytological features of a classic papillary carcinoma (Pap stain) (A), while some irregular clusters and single follicular cells show an abundant oxyphilic cytoplasm (B). Most of the cells show a moderate nuclear enlargement with irregularity and with occasional grooving and intranuclear pseudoinclusions. (C, D) Liquid-based cytology exhibits a homogeneous cellular smear with monolayered sheets lacking a 3-dimensional papillary appearance (Pap stain, SurePath). The cells that compose the clusters have abundant to scant cytoplasm, and those with irregular nuclei contain occasional pseudoinclusions. (E) The conventional smear with hematoxylin and eosin stain reveals a scanty cellular smear with a bloody background and abundant inflammatory cells, the majority of which are lymphocytes. (F) Only a few small clusters of follicular cells with relatively abundant cytoplasm are observed.
The cytological diagnosis for this patient was built up as PTC with oncocytic changes, and the tumor was removed by total thyroidectomy. On gross examination, an ill-defined, white, soft mass with fish-flesh consistency was noted on the upper pole (Fig. 1B). The remaining parenchyma showed diffuse ill-defined, white spots throughout the lobe, which suggested Hashimoto's thyroiditis. The histologic findings were consistent with an oncocytic variant of PTC with lymphocytic stroma, or WL-PTC (Fig. 3). The tumor focally invaded the thyroid capsule without further extension to the perithyroidal soft tissue. There was neither a vascular nor a lymphatic invasion. No tumor metastasis was found among eight dissected lymph nodes. The surrounding parenchyma showed a picture typical of Hashimoto's thyroiditis. The patient remained stable without any recurrent disease during a 6-month follow-up period.

Microscopic findings. (A-C) The tumor is composed of papillary structures of variable sizes, which are lined by atypical follicular cells with abundant oxyphilic cytoplasm and clear grooved nuclei with occasional pseudoinclusions. The core of the papillae shows abundant lymphoid stroma resembling the histologic features of a Warthin tumor. Clear nuclei with occasional pseudoinclusions are evident with frequent psammoma bodies. (D) The remaining parenchyma shows Hashimoto thyroiditis.
DISCUSSION
WL-PTC is still very rare, although the incidence of thyroid carcinoma is continuously increasing worldwide as well as in Korea. The cytological and histological features of WL-PTC are unique, but remain poorly documented. Although the histologic features of WL-PTC are so unique that it can be hardly misdiagnosed, to provide an accurate diagnosis with only cytological samples may be difficult.4,6 Briefly, there are combined cytological findings of both classic PTC and Hashimoto's thyroiditis that are summarized as papillary clusters and/or monolayered sheets of oncocytic follicular cells with ground glass appearance, nuclear grooves, and occasional intranuclear pseudoinclusions on a lymphocyte-rich background. However, the correct diagnosis can be really difficult for a pathologist if there is no single dominant feature of such findings, as mentioned earlier.3,5
The most important and difficult differential diagnosis is that of Hashimoto's thyroiditis, especially if intranuclear pseudoinclusions are not prominent.6 Such pseudoinclusions are an artifact of formalin fixation during tissue processing. As a further difficulty WL-PTC is accompanying well with Hashimoto's thyroiditis in residual thyroid parenchyma. To avoid a misdiagnosis, it is essential to confirm the absence of follicular cells with pseudoinclusions since other benign conditions can present with moderate cellular atypia, including oncocytic changes, nuclear grooves, and ground-glass appearance.6
WL-PTC also can be easily mistaken as follicular adenoma or carcinoma with oncocytic changes if a ground-glass appearance and papillary features are not evident.3 In addition, LBC medium breaks basically large clusters into small pieces during processing. These limitations should be carefully considered if LBC are used for diagnosis.
A heavy lymphocytic background may be a good clue for the differentiation of lymphocyte-rich lesions in thyroid FNAC.5 It also can be totally absent, though, especially when using LBC. In such cases, the smear may resemble an oncocytic variant of PTC.
Conventional smear also can be limited by low cellularity and inter-examiner technique variation. In the present case, a proper diagnosis was possible through a synthesis of cytologic findings of both conventional smears and LBC slides. The papillary clusters and the lymphocytic background were preserved on conventional smears while the intranuclear pseudoinclusions were easily identified on LBC slides due to their relatively high cellularity.
In conclusion, cytological features of WL-PTC can mimic other lymphocyte-rich thyroid lesions such as Hashimoto's thyroiditis, follicular adenoma or carcinoma with oncocytic change, and an oncocytic variant of PTC. Thus, a detailed cytological evaluation with various staining methods and preparation methods is crucial to avoid any misdiagnosis, especially if one or two key features are poorly presented. For the differentiation between benign and malignant lesions, intranuclear pseudoinclusions may be the most helpful feature.
Notes
No potential conflict of interest relevant to this article was reported.