Provisional Guideline Recommendation for EGFR Gene Mutation Testing in Liquid Samples of Lung Cancer Patients: A Proposal by the Korean Cardiopulmonary Pathology Study Group
Article information
 , Hyo Sup Shim1, Tae Jung Kim2, Heae Surng Park3, Yun La Choi4, Wan Seop Kim5, Lucia Kim6, Sun Hee Chang7, Joon Seon Song8, Hyo jin Kim9, Jung Ho Han4, Chang Hun Lee, Geon Kook Lee10, Se Jin Jang,8, Korean Cardiopulmonary Pathology Study Group
, Hyo Sup Shim1, Tae Jung Kim2, Heae Surng Park3, Yun La Choi4, Wan Seop Kim5, Lucia Kim6, Sun Hee Chang7, Joon Seon Song8, Hyo jin Kim9, Jung Ho Han4, Chang Hun Lee, Geon Kook Lee10, Se Jin Jang,8, Korean Cardiopulmonary Pathology Study GroupAbstract
Liquid biopsy for detection of mutation from circulating tumor DNA is a new technology which is attractive in that it is non-invasive. Epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors (TKI) is an effective first line drug for advanced non-small cell lung cancer patients who harbor activating EGFR mutation. During the course of treatment, resistance against TKI arises which can be contributed to EGFR T790M mutation in about 50–60% of patients. Third generation TKI may overcome the resistance. In patients who cannot undergo tissue biopsy due to variable reasons, liquid biopsy is an excellent alternative for the detection of EGFR T790M mutation. However, this relatively novel method requires standardization and vigorous quality insurance. Thus, a standard set of guideline recommendations for liquid biopsy for EGFR mutation testing suitable for the Korean medical community is necessary. In this article, we propose a set of provisional guideline recommendations that was discussed and approved by the Cardiopulmonary Pathology Study Group of the Korean Society of Pathologists.
After the discovery of activating epidermal growth factor receptor (EGFR) gene mutation, EGFR tyrosine kinase inhibitors (TKI) became the first line of treatment in advanced non-small cell lung cancer (NSCLC) with mutated EGFR [1-3]. These EGFR TKIs such as gefitinib, erlotinib, and afatinib show consistently better response rate and prolonged progression-free survival in EGFR mutant NSCLC patients [1-3]. However, most patients receiving EGFR TKI treatment may develop acquired resistance [4-6]. Although various mechanisms are involved in this resistance, secondary T790M mutation of EGFR gene illustrates 50%–60% of the resistance [7,8]. A recently developed third generation TKIs can effectively target T790M, and so it is very critical to detect this mutation in patients who has developed acquired resistance against first- or second-line EGFR TKIs [9-11].
Liquid biopsy is an emerging tool that detects genetic changes in circulating tumor DNA (ctDNA) shed from the tumor cells [12-14]. Recently, Cobas EGFR mutation test V2 (Roche, Indianapolis, IN, USA) has been approved by Food and Drug Administration (FDA) for the detection of EGFR mutations from the blood of NSCLC patients [15]. Although this non-invasive technique is fascinating and promising, it is still a developing method which needs further improvements. Hence, it is necessary to have guidelines for its usage. Korean cardiopulmonary study group has prepared the first guideline of EGFR mutation detection in blood for clinicians and pathologists who actively take part in the diagnosis and treatment of lung cancer.
PATIENT ELIGIBILITY
Liquid biopsy for the detection of EGFR mutation can play many roles in cancer diagnostics [12-14,16,17]. Patients diagnosed with lung adenocarcinoma harboring EGFR mutation will be the first candidates when they develop resistance against first-line TKIs. Especially, when the tumor is too small or located in a challenging region to be sampled, liquid biopsy can be a good alternative [14-18]. Patients with poor performance status can also benefit from this technique.
SAMPLE COLLECTION
Sample collection and processing is a critical step in liquid biopsy. Since ctDNA is rapidly degraded by the nuclease in blood and contaminated by genomic DNA from blood cells, it is essential to separate plasma from the sample [13,14]. The routine venipuncture technique will be sufficient to collect blood from the patients. The sample collection tube should be chosen considering each institution’s setting. Conventional ethyldiaminetetraaceticacid (EDTA) tube can be used if the samples are processed without delay [19,20]. Recently, specialized tubes for delaying degradation of ctDNA are commercially available [19,20]. The tube from Streck (Omaha, NE, USA) has been the most widely used collection tube. Roche diagnostics and Qiagen have also marketed specialized tubes. According to a study [19], conventional EDTA tube and Streck tube do not show much difference in their performance when samples are processed within 6 hours. When incubated longer in EDTA tube, cell-free DNA may be released from the blood cells, and EDTA will hinder the polymerase chain reaction (PCR) [20]. Tubes from Roche and Qiagen showed similar performance, and they are slightly better than Streck tube [20]. Specialized tubes can sustain sample quality for several days at room temperature before processing further (Table 1).

Comparison of specialized tubes for collection of ctDNA
CIRCULATING TUMOR DNA ISOLATION
Before ctDNA extraction, blood should be processed into plasma through double centrifugation. Plasma samples are better than serum samples, which can be contaminated by DNA released from immune cells [13]. Since a small amount of ctDNA is present in plasma, isolation is a critical step in the process for saving tumor DNA. Several commercial kits for isolation are available in the market (Table 2) [21,22]. These are manual, semiautomatic, and fully automatic. Manual protocol uses column-based method while semi-automatic instrument works with magnetic beads. Previous studies showed variable results depending on the extraction kits, though they all had similar performances [21,22]. The technician’s skill and protocol optimization may be one of the critical factors for yielding better ctDNA. Table 1 summarizes commercial ctDNA extraction kits.

Commercially available ctDNA extraction kits
MUTATION DETECTION METHODS
High sensitivity detection methods are required to detect EGFR mutations from liquid samples. Kits for detecting mutations have been developed and are commercially available [23-25]. Each kit requires different quality and amount of DNA (Table 3). They depend on real time PCR technology with their own variations. Roche Cobas uses real time PCR with Taqman like probe and Qiagen has released ARMS based kits, Therascreen EGFR RGQ. Another PCR based technique uses peptide nucleic acid clamping and Panamutyper (Panagene, Daejeon, Korea). The Roche and Qiagen systems use their own PCR machine from Roche and Qiagen while Panamutyper can run on any qualified PCR machines. The number of mutations these kits can detect are different; however, together they include exon 19 deletion, T790M and L858R. Currently, only Roche kit has acquired FDA approval. The most important element of these kits is how sensitively and specifically they can detect mutations in liquid samples. There are certain studies to evaluate their performance and report sensitivities ranging from 62% to 67.5% and specificities ranging from 88% to 97% [26-29]. In the ASSESS study, these three kits showed high specificity, however, sensitivity was equal to or less than 75% [25]. For T790M, sensitivity was 41% and 29% for Cobas and Therascreen, respectively, and specificity was 100% for both kits from the patients enrolled in AURA trial [10]. Therefore, deciding the best kit will depend on the laboratory’s choice with consideration of their requirements. Features of these products are summarized in Table 3. Other platforms using digital PCR and next generation sequencing are still far from widespread use in clinical setting [24].

EGFR mutation detection kits in plasma
REPORTING FORMAT
Once liquid biopsy for detecting T790M mutation is done, the reports should contain the following information: pathologic number, age, sex, hospital unit number, sample source, requesting physician, requesting department, adequacy for testing (amount of DNA extracted), receipt day, report day, storage tube, methodology used, exons tested and associated range of detectable mutations, mutation status, comments, testing technician, and corresponding pathologist. Since the patients already have sensitizing EGFR mutation, it is recommended to include the type of original EGFR alteration and previous histologic diagnosis.
PROPOSAL FOR AN EXTERNAL QUALITY ASSESSMENT PROGRAM
Since liquid biopsy technique has not been validated yet, vigorous quality assurance is necessary. Although there is no recommended program for external quality assessment (EQA), one pilot trial for EGFR testing in blood is ongoing in Germany [30]. Another program for BRAF and KRAS is also being conducted [31]. Since patient derived standard sample is difficult to store and distribute, artificial sample mimicking the real one can be used instead [30,31]. We are in the process of developing Korean EQA program.
ROLE OF PATHOLOGISTS
Performance and interpretation of liquid biopsy require broad knowledge in lung cancer pathology. Pathologists have an important role in the diagnosis and management of cancer and thus can interpret liquid biopsy results in conjunction with the histologic diagnosis, previous status of EGFR-activating mutation, and clinical situation. The liquid biopsy in lung cancer is usually performed in patients whose previous EGFR mutation status has been known. The sole purpose of this technique is to detect a T790M mutation responsible for TKI resistance. Unlike tissue specimens, in which the pathologists can determine the percentage of tumor cells, it is extremely difficult to estimate whether the blood sample contains a sufficient amount of tumor DNA. If the sample is adequate, the test generally finds the original EGFR-activating mutation, which may act as an internal control for the presence of ctDNA [13]. When it has not detected any EGFR-activating mutation including previously existing one or reported mutations other than the preexisting ones or T790M, pathologists should be able to interpret the result. In the former, test should be repeated because the samples might have been degraded and contain insufficient ctDNA. In the latter, the newly emerged mutation, in the presence of newly developed lesion, may indicate a metachronous primary tumor. The communication between pathologists, clinicians, and radiologists is important for further diagnosis and management of cancer. Moreover, lung adenocarcinoma undergoes frequent transformation into small cell carcinoma when it is treated with TKI, while maintaining the original EGFR mutation [7,8,32]. Recommended interpretation is suggested in Table 4.

Recommended interpretation of EGFR mutation test from blood
PERSPECTIVES AND ADDITIONAL RECOMMENDATIONS
EGFR mutation testing performed with blood or other liquid sample is a non-invasive method, which can be more widely adopted. Laboratories must get familiar with liquid samples and develop their own protocols to handle these specimens. They can choose appropriate sample tubes, extraction kits, detection methods, and other instruments. They should select the most suitable combination in accordance with their requirements, unless the detection kits indicate specific methods and instruments [31]. Although sensitivity of tissue biopsy is higher than liquid biopsy, both are far from perfection and T790M mutation can be detected only in one of the two methods. Reportedly, allele fraction of T790M mutation tends to correlate with treatment efficacy of osimertinib [33]. Therefore, absence of T790M in tumor tissue while it is detected in plasma might reflect low allele frequency and lead to poor response. Therefore, the two methods are complementary to each other and should be selected according to each patient’s condition (Fig. 1).
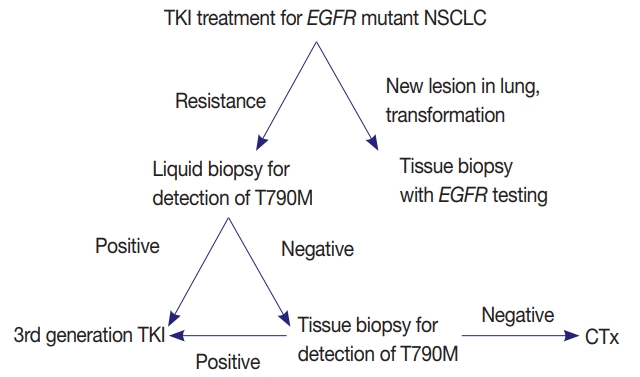
Proposed diagnostic algorithm for the detection of epidermal growth factor receptor (EGFR) T790M mutation. NSCLC, nonsmall cell lung cancer; TKI, tyrosine kinase inhibitor; CTx, chemotherapy.
CONCLUSIONS
Liquid biopsy is a promising method, which is safe and convenient. Before more experiences and data are accumulated, liquid biopsy should be performed with great caution. There are a few steps in liquid biopsy, which can produce false negative or false positive results. Interpretation requires profound knowledge of lung cancer including diagnosis, treatment, and prognosis. However, in debatable cases, discussion between pathologists, physicians, and radiologists is critical. This method will soon play a major role in early diagnosis, monitoring of treatment, and detection of minimal residual disease. Currently, it cannot replace the conventional pretreatment tissue diagnosis [14]. It is important to validate and improve the performance of this technique before it is widely used in clinical practice. Liquid biopsy performed in EGFR has provided a platform for determining gene mutations in KRAS, ALK, PI3CA, and BRAF as well.
Notes
Author contributions
Conceptualization: DHS, HSS, TJK, HSP, YLC, WSK, LK, SHC, JSS, HJK, JHH, CHL, GKL, SJJ.
Data curation: DHS.
Formal analysis: DHS, HSS, TJK.
Investigation: DHS, HSP, YLC, WSK, LK.
Methodology: DHS, SHC, JSS, HJK, JHH.
Project administration: JHH, CHL, GKL, SJJ.
Writing—original draft: DHS.
Writing—review & editing: DHS, HSS, TJK, HSP, YLC, WSK, LK, SHC, JSS, HJK, JHH, CHL, GKL, SJJ.
Conflicts of Interest
The authors declare that they have no potential conflicts of interest.