 E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 52(4); 2018 > Article
-
Original Article
Pulmonary Nodular Lymphoid Hyperplasia with Mass-Formation: Clinicopathologic Characteristics of Nine Cases and Review of the Literature -
Jongmin Sim
 , Hyun Hee Koh, Sangjoon Choi, Jinah Chu, Tae Sung Kim1, Hojoong Kim2, Joungho Han
, Hyun Hee Koh, Sangjoon Choi, Jinah Chu, Tae Sung Kim1, Hojoong Kim2, Joungho Han -
Journal of Pathology and Translational Medicine 2018;52(4):211-218.
DOI: https://doi.org/10.4132/jptm.2018.04.27
Published online: June 15, 2018
Department of Pathology and Translational Genomics, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
1Department of Radiology, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
2Division of Pulmonary and Critical Care Medicine, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- Corresponding Author Joungho Han, MD Department of Pathology and Translational Genomics, Samsung Medical Center, Sungkyunkwan University School of Medicine, 81 Irwon-ro, Gangnam-gu, Seoul 06351, Korea Tel: +82-2-3410-2765 Fax: +82-2-3410-0025 E-mail: hanjho@skku.edu
© 2018 The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Background
- Pulmonary nodular lymphoid hyperplasia (PNLH) is a non-neoplastic pulmonary lymphoid disorder that can be mistaken for malignancy on radiography. Herein, we present nine cases of PNLH, emphasizing clinicoradiological findings and histological features.
-
Methods
- We analyzed radiological and clinicopathological features from the electronic medical records of nine patients (eight females and one male) diagnosed with PNLH. IgG and IgG4 immunohistochemical staining was performed in three patients.
-
Results
- Two of the nine patients had experienced tuberculosis 40 and 30 years prior, respectively. Interestingly, none were current smokers, although two were ex-smokers. Three patients complaining of persistent cough underwent computed tomography of the chest. PNLH was incidentally discovered in five patients during examination for other reasons. The remaining patient was diagnosed with the disease following treatment for pneumonia. Imaging studies revealed consolidation or a mass-like lesion in eight patients. First impressions included invasive adenocarcinoma and mucosal-associated lymphoid tissue‒type lymphoma. Aspergillosis was suspected in the remaining patient based on radiological images. Resection was performed in all patients. Microscopically, the lesions consisted of nodular proliferation of reactive germinal centers accompanied by infiltration of neutrophils and macrophages in various degrees and surrounding fibrosis. Ultimately, all nine patients were diagnosed with PNLH and showed no evidence of recurrence on follow-up.
-
Conclusions
- PNLH is an uncommon but distinct entity with a benign nature, and understanding the radiological and clinicopathological characteristics of PNLH is important.
- Case selection and clinical data
- The electronic medical records of Samsung Medical Center were searched for lung specimens of patients diagnosed with PNLH between January 2012 and September 2017. We excluded lymphoid interstitial pneumonia and other lymphoproliferative disorders that were not nodular or reactive. Clinical characteristics of patients were also retrieved from the electronic medical records, including age, sex, chief complaint, past and/or current history, smoking history, and radiological findings. The present study protocol was reviewed and approved by the Institutional Review Board (IRB) of Samsung Medical Center (IRB No. 2017-10-055-011). Formal written informed consent was not required and was waived by the IRB.
- Pathological evaluation
- Two pathologists (J. Han and J. Sim) reviewed the slides of selected cases. Primary malignant lymphomas and other lymphoproliferative lesions were excluded. IHC staining with CD3 (A0452, Dako, Glostrup, Denmark), CD20 (L26, Leica, Wetzlar, Germany), and Ki-67 (MIB-1, Dako) was performed in all cases. BCL2 (124, Dako), BCL6 (LN22, Novocastra, Newcastle upon Tyne, UK), and kappa and lambda light chain (Dako) IHC staining was performed in only one patient who showed a diffuse pattern (case 6). Additionally, the IgG4:IgG ratio was assessed using IgG (Dako) and IgG4 (MRQ-44, Cell Marque, Rocklin, CA, USA) antibodies in only three cases which showed plasma cell infiltration (cases 1, 2, and 6). Special staining was performed to confirm the presence of microorganisms. Molecular tests such as IgH gene rearrangement test were not performed in any case.
MATERIALS AND METHODS
- Clinical and radiological findings
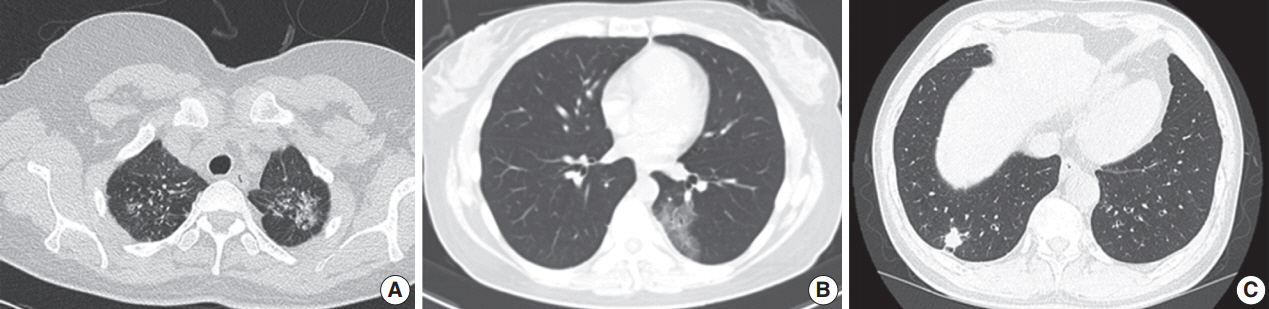
- Table 1 shows the clinicopathological characteristics of the nine patients (eight females and one male). The mean age was 57.3 years (range, 39 to 79 years). Two patients (patients 2 and 3) had a history of tuberculosis 40 and 30 years prior, respectively. Seven patients had never smoked, and the other two patients were ex-smokers who stopped smoking 20 and 2 years prior, respectively; none of the patients were current smokers. Three patients were diagnosed with cough symptoms, and five were accidentally discovered during an examination for other reasons, including angina, emphysema, health examination, and systemic lupus erythematosus. The remaining patient was identified after treatment for pneumonia. Only one patient (patient 6) had several autoimmune antibody tests. Antinuclear antibody titer was 1:40 with a nuclear pattern. Negative results were obtained for several autoimmune antibodies, including anti-Sjogren’s syndrome A, anti-Sjogren’s syndrome B, anti-ribonucleoprotein, anti-Sm, and antineutrophil cytoplasmic antibodies. The lesions were solitary in eight patients and multiple in one patient (patient 2). Most radiological findings were persistent and/or slow-growing consolidation lesions (Fig. 1). In eight patients, the possibility of primary lymphoma or primary lung cancer was suspected based on radiological findings. One patient (patient 4) was suspected of aspergilloma based on radiological images. Recurrence, previous disease, or new lesions were not observed in any patient during the 3–18 months of radiological follow-up.
- Pathological features
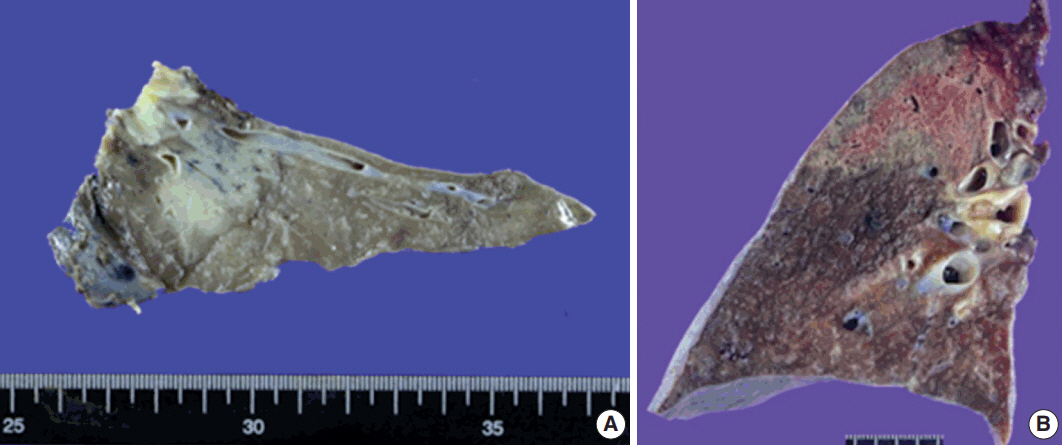
- Although gross images were not available in four patients, softto-firm and well-circumscribed lesions were observed in most cases on gross examination. An infiltrative mass-like lesion mimicking invasive lung cancer was observed on one image (Fig. 2A). The remaining four patients showed a relatively well-defined lesion with soft-to-firm consistency (Fig. 2B).
- Based on microscopy, the lesions were relatively well-defined with a nodular pattern. Although six of nine patients had well-marginated and regular borders (Fig. 3A), three had a relatively well-demarcated, irregular borders (Fig. 3B). Four cases showed a nodular pattern (Fig. 3B), and the other five showed a mixed diffuse and nodular pattern (Fig. 3C, D). Each lesion was composed of polymorphous lymphoid cells, reactive germinal centers, and infiltration of a variety of neutrophils, plasma cells, and macrophages without a carcinoma component. No Dutcher bodies or invasion of the pleura were present in any case. In addition, three cases showed moderate neutrophilic infiltration with a few macrophages. In contrast, moderate to marked infiltration of macrophages with rare neutrophilic infiltration was observed in five cases. The remaining one showed marked infiltration of neutrophils and macrophages. The degree of fibrosis was variable. Three cases showed rare or mild fibrosis (Fig. 3A, B), and the remaining six displayed moderate to marked fibrosis (Fig. 3D). However, the pattern of fibrosis was not storiform in any case. Obliterative arteritis or phlebitis suggesting IgG4-related disease was not detected in any patient. The amount of plasma cell infiltration also varied from scattered to dense. The plasma cell infiltration was in a scattered pattern in three cases and moderate to marked in six cases (Fig. 3E). Two patients had mild lymphoepithelial lesions which were not extensive or destructive (Fig. 3F). Microscopic features are summarized in Table 2.
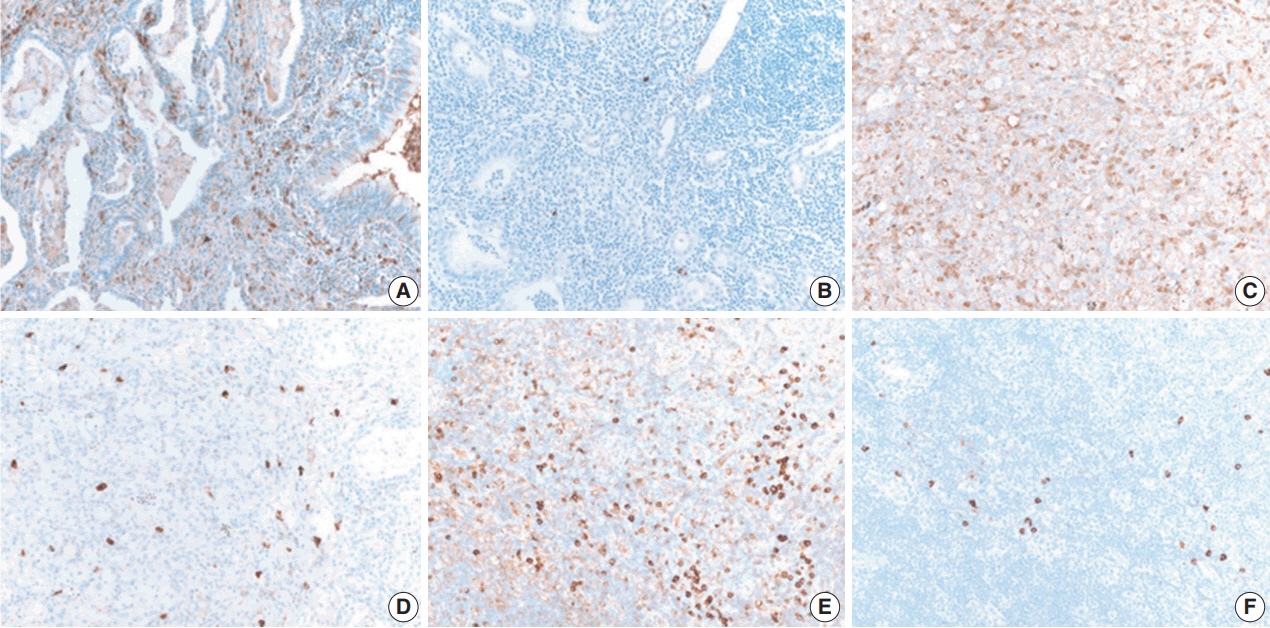
- IHC staining for B cells showed numerous B cells within reactive follicles in all cases (Fig. 4A). IHC staining for CD3 displayed many T cells in interfollicular areas and occasional T cells within reactive follicles (Fig. 4B). A high proliferative activity (Ki-67 index) was observed in reactive follicles (Fig. 4C), dividing dark and light zones. Although two cases showed a diffuse pattern, diffuse B-cell infiltration which is a characteristic of extranodal marginal zone lymphoma of mucosal-associated lymphoid tissue (MALT)-type lymphoma was not identified by CD3 and CD20 IHC staining (Fig. 4D, E). Additionally, BCL2 and BCL6 IHC staining confirmed inter-follicular lymphoid cells and germinal centers (Fig. 4F, G). Moreover, kappa and lambda light chain IHC staining did not reveal any monoclonality (Fig. 4H, I).
- Thus, PNLH was diagnosed as such. In all patients, molecular tests such as IgH gene rearrangement test were not required to differentiate malignant lymphomas. Patient 4 showed an aspergillus species that was confirmed by Grocott’s methenamine silver stain and periodic acid–Schiff stain (not shown). The IgG4:IgG ratio was less than 0.2 in three patients, which was not compatible with IgG4-related disease (Fig. 5).
RESULTS
- We reviewed clinicopathological features of nine PNLH patients. Based on radiological findings, eight patients were suspected to have a malignancy such as adenocarcinoma or MALT-type lymphoma, and one showed a solid mass-forming lesion on gross examination. However, histological findings on H&E staining showed benign reactive lesions. Non-extensive lymphoepithelial lesions were present in two patients. However, extensive lymphoepithelial lesion, Dutcher bodies, or pleural invasion were not observed. Additional IHC staining for CD3, CD20, and Ki-67 showed no evidence of malignancy. Only one case showed a diffuse pattern; additional staining was required to distinguish the lesion from MALT-type lymphoma. IHC staining of kappa and lambda light chain indicated a polyclonal population. Molecular testing such as IgH gene rearrangement test was not performed in any case.
- PNLH is usually asymptomatic and in most cases is found incidentally during examination for other reasons. As mentioned above, PNLH is a benign lesion typically diagnosed histologically using H&E-stained slides [2,3,6,9]. Based on histological analysis, PNLH is composed of reactive germinal centers with a nodular pattern and is mainly located in the subpleural area. Fibrosis and infiltration of other inflammatory cells are variable. Lymphoepithelial lesions with lymphocytes infiltrating the bronchial epithelium can occur [10]; however, no pleural or bronchus invasion is observed [6,10]. Although presence of a single lesion is common, the clinical course of solitary and multiple lesions is similar. Based on radiological findings, PNLH appears as a consolidation or mass-like lesion and cannot be easily distinguished from lung cancer or malignant lymphoma, especially when the size increases during follow-up [7]. Differential diseases include lymphoid interstitial pneumonia, follicular bronchitis, and MALT-type lymphoma [2,8,9,11]. Lymphoid interstitial pneumonia infiltrates the lungs as a whole and does not form a germinal center. MALT-type lymphoma also presents with a diffuse pattern with monotonous lymphoid cells. Dutcher bodies, pleural invasion, and bronchus invasion are common in MALT-type lymphoma. IHC staining and/or IgH gene rearrangement test indicate a monoclonal population. The key features of PNLH and MALT-type lymphoma are summarized in Table 3.
- In 2000, Abbondanzo et al. [6] reported clinicopathological features of 14 patients with PNLH. They demonstrated that PNLH was mainly asymptomatic, incidentally found on radiological imaging or due to complaints of cough, and often observed as a mass on radiological imaging. Although most patients presented with a single mass smaller than 3 cm, others were as large as 5 cm. Histological analysis showed that PNLH has germinal centers with a nodular pattern, sometimes accompanied by fibrosis. Lymphoepithelial lesions, pleural plaques, or bronchial cartilage involvement was not observed. However, Begueret et al. [10] demonstrated that PNLH could also have lymphoepithelial lesions. They further found the lymphoepithelial lesions in MALT-type lymphoma were CD20+/CD43+, in contrast to CD3+/CD43+ or CD20+/CD43– lesions in lymphoid hyperplasia. Moreover, they found no intralymphatic extension in lymphoid hyperplasia.
- In 2013, Guinee et al. [12] reported that the number of IgG4-positive plasma cells was significantly higher in PNLH than in other lesions. Their study included six patients with PNLH, nine patients with MALT-type lymphoma, eight patients with intrapulmonary lymphoma, eight patients with follicular bronchitis, and four patients with lymphoid interstitial pneumonia. They demonstrated that the IgG4/IgG ratio in PNLH was significantly higher than in other lesions. Moreover, two of six PNLH patients had an IgG4/IgG ratio greater than 0.4. However, in 2017, Bois et al. [13] reported that the ratio in 26 PNLH patients was not higher than that in controls. The control group in their study included two patients with diffuse lymphoid hyperplasia without nodularity, five patients with usual interstitial pneumonia and increased lymphoplasmacytic infiltrates, and two patients with thoracic lymphadenopathy. In addition, they found that PNLH had a low IgG4/IgG ratio that did not suggest IgG4-related disease and reported no evidence of Epstein-Barr virus infection. In our study, IgG and IgG4 IHC staining results were available in three patients. Similar to the previous results, there was no evidence of IgG4-related disease in those patients. Whether PNLH is associated with IgG4-related disease requires further evaluation with a greater number of patients.
- Interstitial lung disease (ILD) may be the first presentation of connective tissue diseases (CTDs); up to 15% of patients initially diagnosed with idiopathic nonspecific interstitial pneumonia (NSIP) have an underlying systemic autoimmune rheumatic disease upon further evaluation [14,15]. The most common histological pattern in patients with CTD is NSIP [14]. However, no evidence of ILD except PNLH was found in the systemic lupus erythematosus patient included in this study. Moreover, on radiological analysis, ILD was not evident. PNLH in patients with Sjogren’s syndrome was previously reported [16]. To determine whether PNLH is associated with CTD requires further studies with a larger cohort.
- In addition, we observed that PNLH could have various degrees of fibrosis as well as neutrophil and macrophage. Patients with PNLH could possibly be diagnosed using some of the organizing pneumonia spectrum as a post-obstructive change due to mass formation. Moderate to marked infiltration of neutrophils with rare macrophage infiltration could represent a relatively early phase of organizing pneumonia, while numerous macrophages and surrounding fibrosis with rare neutrophil infiltration are more likely to indicate progression of organizing pneumonia.
- In conclusion, we report a mass-like or consolidative lesion in nine patients with PNLH. Differential diagnosis of PNLH includes MALT-type lymphoma and other benign lymphoproliferative disorders. Although molecular tests were not performed, meticulous pathological examination can aid in diagnosing PNLH with confidence.
DISCUSSION


TB, tuberculosis; S, solitary; M, multiple; Dx, diagnosis; F, female; GGO, ground glass opacity; LUL, left upper lobe; DDx, differential diagnosis; MALT, mucosaassociated lymphoid tissue; R/O, rule out; Segm, segmentectomy; PNLH, pulmonary nodular lymphoid hyperplasia; YA, years ago; RLL, right lower lobe; Lobe, lobectomy; LLL, left lower lobe; Wegde, wedge resection; SLE, systemic lupus erythematosus; EX, ex-smoker; RUL, right upper lobe; PET, positron emission tomography.
- 1. Travis WD, Galvin JR. Non-neoplastic pulmonary lymphoid lesions. Thorax 2001; 56: 964-71. PubMedPMC
- 2. Guinee DG Jr. Update on nonneoplastic pulmonary lymphoproliferative disorders and related entities. Arch Pathol Lab Med 2010; 134: 691-701. ArticlePubMedPDF
- 3. Yi E, Aubry MC. Pulmonary pseudoneoplasms. Arch Pathol Lab Med 2010; 134: 417-26. ArticlePubMedPDF
- 4. Saltzstein SL. Pulmonary malignant lymphomas and pseudolymphomas: classification, therapy, and prognosis. Cancer 1963; 16: 928-55. ArticlePubMed
- 5. Kradin RL, Mark EJ. Benign lymphoid disorders of the lung, with a theory regarding their development. Hum Pathol 1983; 14: 857-67. ArticlePubMed
- 6. Abbondanzo SL, Rush W, Bijwaard KE, Koss MN. Nodular lymphoid hyperplasia of the lung: a clinicopathologic study of 14 cases. Am J Surg Pathol 2000; 24: 587-97. PubMed
- 7. Sirajuddin A, Raparia K, Lewis VA, et al. Primary pulmonary lymphoid lesions: radiologic and pathologic findings. Radiographics 2016; 36: 53-70. ArticlePubMed
- 8. Poletti V, Ravaglia C, Tomassetti S, et al. Lymphoproliferative lung disorders: clinicopathological aspects. Eur Respir Rev 2013; 22: 427-36. ArticlePubMedPMC
- 9. Arcadu A, Moua T, Yi ES, Ryu JH. Lymphoid interstitial pneumonia and other benign lymphoid disorders. Semin Respir Crit Care Med 2016; 37: 406-20. ArticlePubMedPDF
- 10. Begueret H, Vergier B, Parrens M, et al. Primary lung small B-cell lymphoma versus lymphoid hyperplasia: evaluation of diagnostic criteria in 26 cases. Am J Surg Pathol 2002; 26: 76-81. PubMed
- 11. Tashtoush B, Okafor NC, Ramirez JF, Smolley L. Follicular bronchiolitis: a literature review. J Clin Diagn Res 2015; 9: OE01-5. Article
- 12. Guinee DG Jr, Franks TJ, Gerbino AJ, Murakami SS, Acree SC, Koss MN. Pulmonary nodular lymphoid hyperplasia (pulmonary pseudolymphoma): the significance of increased numbers of IgG4-positive plasma cells. Am J Surg Pathol 2013; 37: 699-709. PubMed
- 13. Bois MC, Sekiguchi H, Ryu JH, Yi ES. No definite clinical features of immunoglobulin G4-related disease in patients with pulmonary nodular lymphoid hyperplasia. Hum Pathol 2017; 59: 80-6. ArticlePubMed
- 14. Atzeni F, Gerardi MC, Barilaro G, Masala IF, Benucci M, Sarzi-Puttini P. Interstitial lung disease in systemic autoimmune rheumatic diseases: a comprehensive review. Expert Rev Clin Immunol 2018; 14: 69-82. ArticlePubMed
- 15. Mittoo S, Gelber AC, Christopher-Stine L, Horton MR, Lechtzin N, Danoff SK. Ascertainment of collagen vascular disease in patients presenting with interstitial lung disease. Respir Med 2009; 103: 1152-8. ArticlePubMed
- 16. Song MK, Seol YM, Park YE, et al. Pulmonary nodular lymphoid hyperplasia associated with Sjogren's syndrome. Korean J Intern Med 2007; 22: 192-6. ArticlePubMedPMC
REFERENCES
Figure & Data
References
Citations
- Clinical and MRI features for differentiating reactive lymphoid hyperplasia from hepatocellular carcinoma in non-cirrhotic chronic HBV patients
Qiansen Lin, Gengyun Miao, Lishan Wang, Chen Xu, Pengju Xu
European Journal of Radiology.2026; 200: 112844. CrossRef - Clinical and Imaging Features of Pulmonary Nodular Lymphoid Hyperplasia
Dong-Lei Nie, Yan-Hong Shi, Xin-Min Li, Xiao-Jiang Wang, Bao-Li Han, Guo-Fu Zhang
Journal of Thoracic Imaging.2025;[Epub] CrossRef - Pathologic Findings of Pulmonary Lymphoproliferative Disorders
Yoshiaki Zaizen, Junya Fukuoka
Seminars in Ultrasound, CT and MRI.2025; 46(4): 272. CrossRef - Utilizing Immunoglobulin G4 Immunohistochemistry for Risk Stratification in Patients with Papillary Thyroid Carcinoma Associated with Hashimoto Thyroiditis
Faridul Haq, Gyeongsin Park, Sora Jeon, Mitsuyoshi Hirokawa, Chan Kwon Jung
Endocrinology and Metabolism.2024; 39(3): 468. CrossRef - Pulmonary Nodular Lymphoid Hyperplasia Evaluated with Bronchoalveolar Lavage Fluid Findings: A Case Report and Review of the Literature on Japanese Patients
Sakiko Moriyama, Takashi Kido, Noriho Sakamoto, Mai Fuchigami, Takatomo Tokito, Daisuke Okuno, Takuto Miyamura, Shota Nakashima, Atsuko Hara, Hiroshi Ishimoto, Yoshitaka Imaizumi, Kazuto Tsuruda, Katsunori Yanagihara, Junya Fukuoka, Hiroshi Mukae
Internal Medicine.2023; 62(1): 95. CrossRef - A Case of Pulmonary Nodular Lymphoid Hyperplasia Responding to Corticosteroid Treatment
Jonathan Teow Koon Goh, Issam Al Jajeh, Jessica Han Ying Tan
Cureus.2023;[Epub] CrossRef - Pulmonary nodular lymphoid hyperplasia presenting as cavitating lung mass
Aqeel Alameer, Chary Duraikannu, Avinash Kumar Kanodia, David Dorward
BMJ Case Reports.2023; 16(8): e254121. CrossRef - Clinicopathological Characteristics and Curative Effect of Lymphoma Based on Sampling Theory
Shuxiang Ding, Leipo Liu
Mathematical Problems in Engineering.2022; 2022: 1. CrossRef - Pulmonary nodular lymphoid hyperplasia presenting as multifocal subsolid nodules: A case report and literature review
Yoon Jin Cha, Duk Hwan Moon, Ji Hyun Park, Sungsoo Lee, Ji Ae Choi, Tae Hoon Kim, Chul Hwan Park
Respiratory Medicine Case Reports.2022; 36: 101581. CrossRef - Pulmonary nodular lymphoid hyperplasia in a 53-year-old man with malignant sign: a case report
Zhen Yang, Lianshuang Wei, Xu Li, Xin Liu
Journal of Cardiothoracic Surgery.2021;[Epub] CrossRef - The diagnostic challenge of adenocarcinoma in pulmonary nodular lymphoid hyperplasia
Anita Savić Vuković, Melita Kukuljan, Morana Dinter, Ksenija Jurinović, Nives Jonjić
SAGE Open Medical Case Reports.2021;[Epub] CrossRef
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-
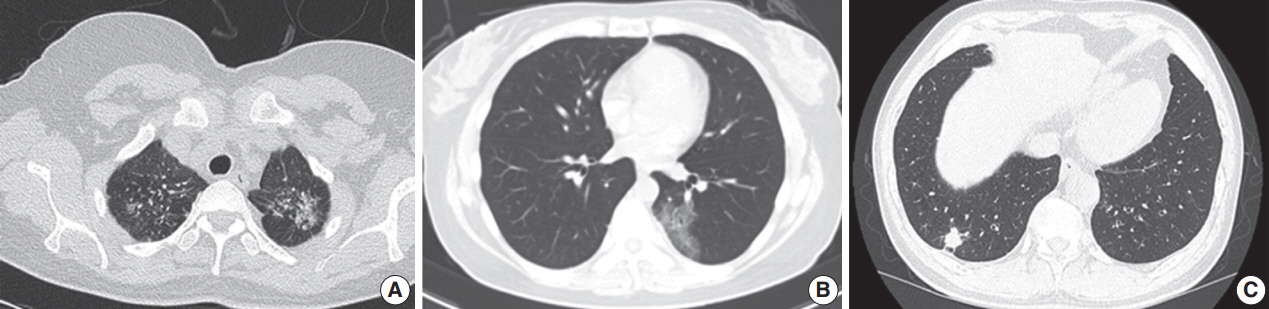
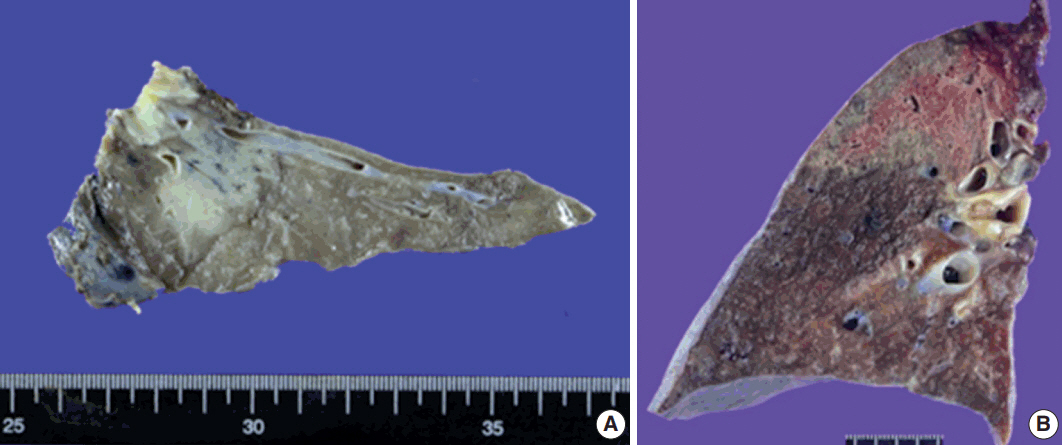
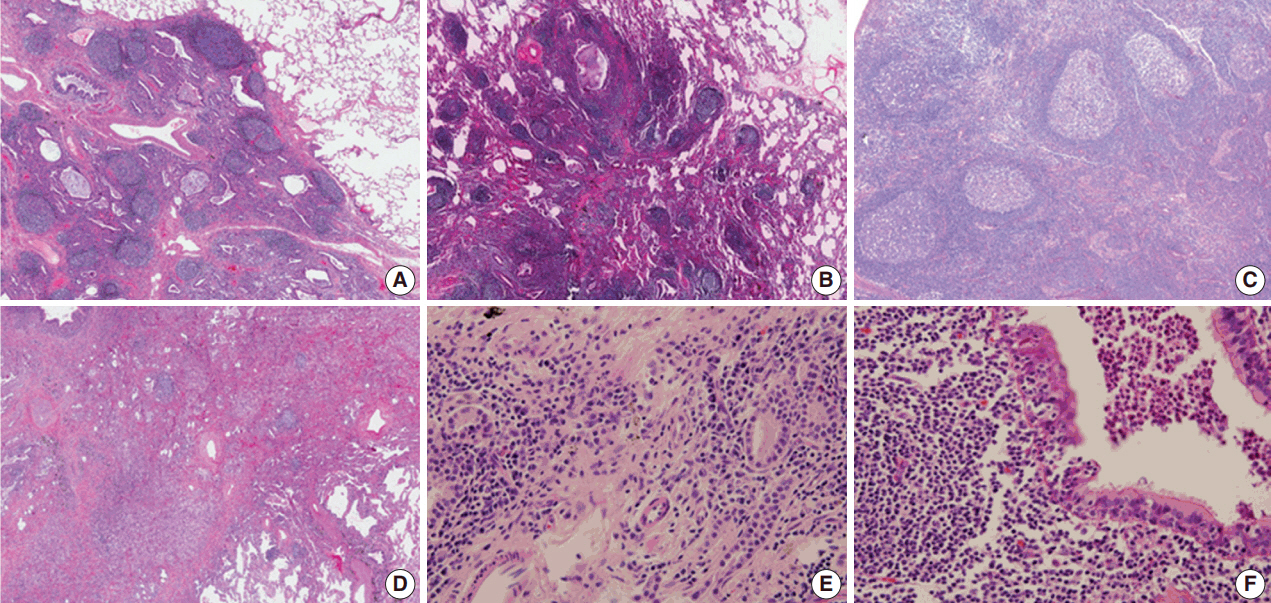
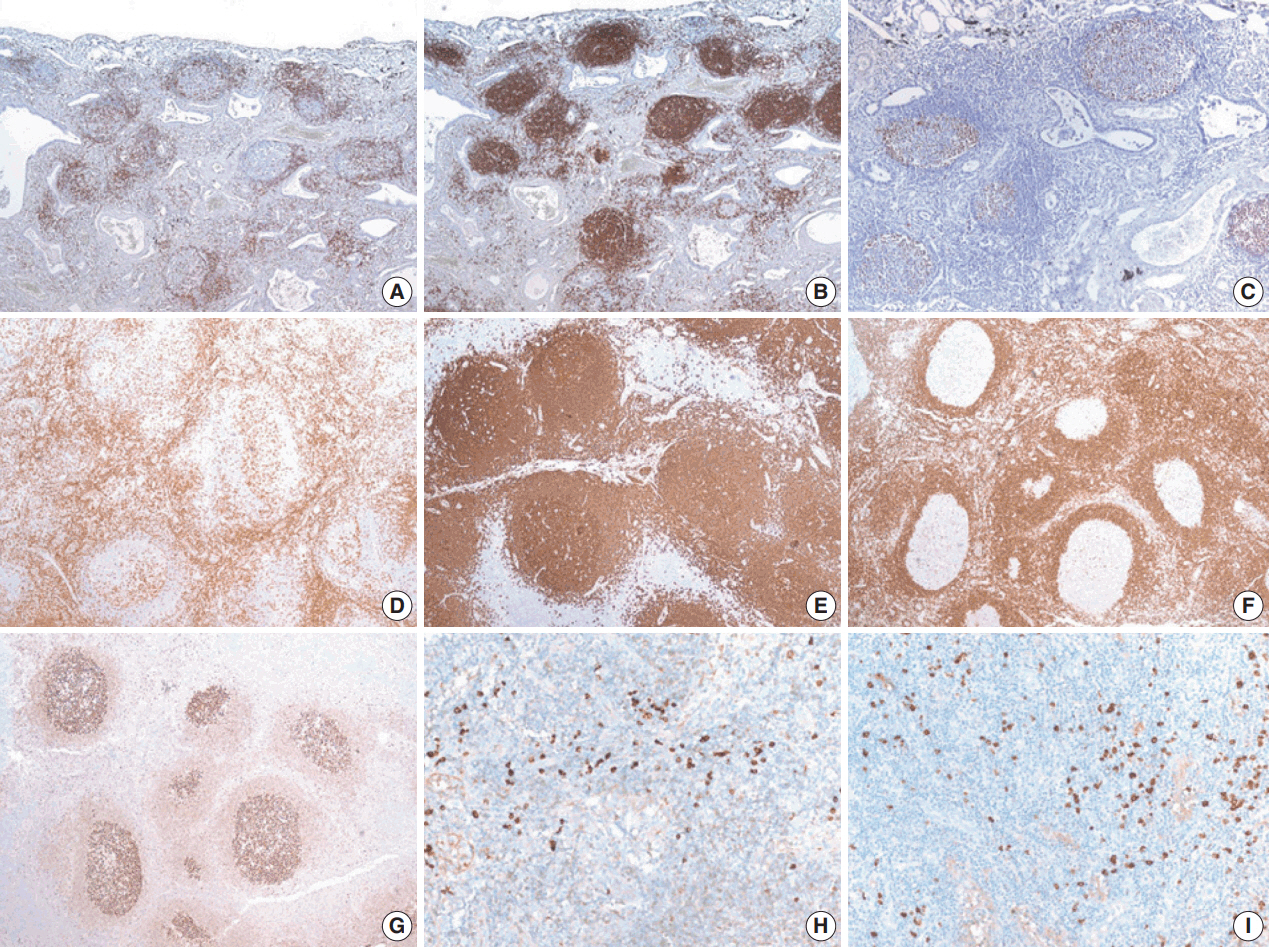
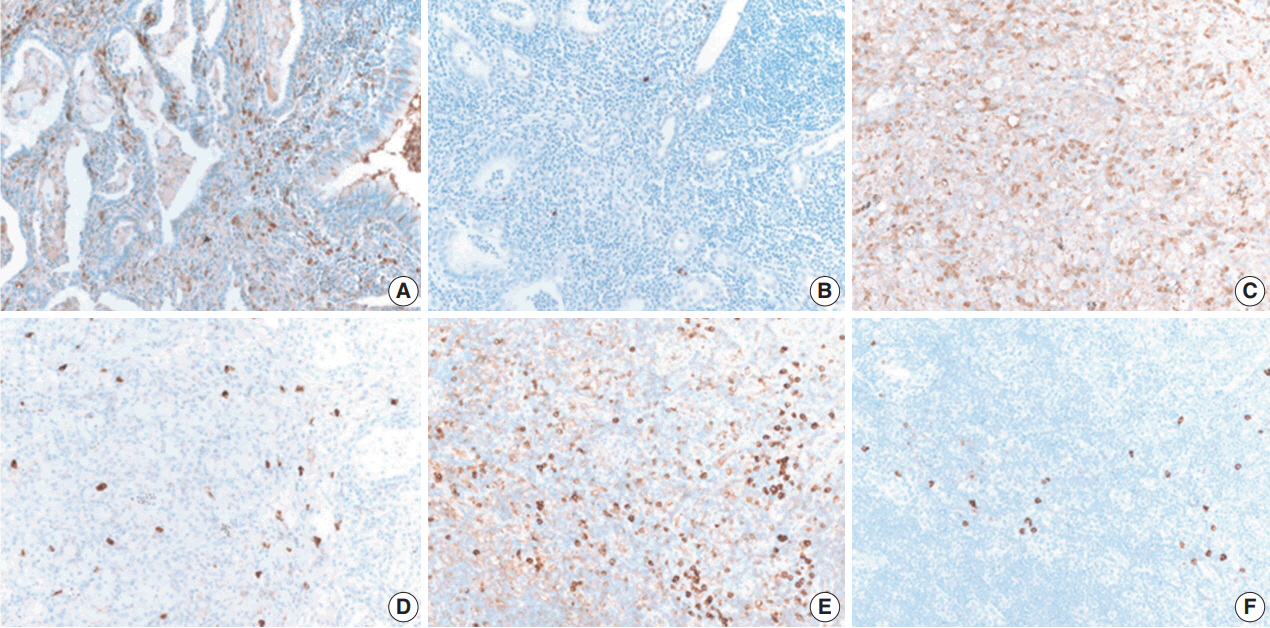





Fig. 1.
Fig. 2.
Fig. 3.
Fig. 4.
Fig. 5.
| No. | Age | Sex | TB | Smoking history | Chief complaint | Site | S/M | Radiology finding | Procedure | Dx | Size (cm) | Follow up (mo) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 42 | F | None | Never | GGO after treatment for pneumonia | LUL | S | Persistent subsegmental consolidation | Segm | PNLH with post-obstructive change | 7 | 10 | |
| DDx | |||||||||||||
| 1) MALT-type lymphoma | |||||||||||||
| 2) R/O Organizing pneumonia | |||||||||||||
| 2 | 62 | F | 40 YA | Never | Cough | RLL | M | Persistent two consolidative lesions | Lobe | PNLH with post-obstructive change | 5.5 | 4 | |
| R/O malignancy such as MALT-type lymphoma or mucinous adenocarcinoma | |||||||||||||
| 3 | 57 | F | 30 YA | Never | Cough | LUL | S | Increase in extent of 58 mm subsolid lesion | Segm | PNLH with post-obstructive change | 4.9 | ||
| DDx | |||||||||||||
| 1) Focal organizing pneumonia | |||||||||||||
| 2) Invasive adenocarcinoma | |||||||||||||
| 3) MALT-type lymphoma | |||||||||||||
| 4 | 59 | F | None | Never | Incidentally found when work-up for angina | LLL | S | Lesion showing air-crescent sign with peribronchail bronchiectasis | Segm | PNLH with post-obstructive change | 1.2 | 15 | |
| R/O Aspergilloma | |||||||||||||
| 5 | 79 | F | None | Never | Cough | LUL | S | A 33-mm-sized ill-defined mass-like lesion | Wedge | PNLH with post-obstructive change | 3.3 | 4 | |
| R/O Lung cancer | |||||||||||||
| 6 | 50 | F | None | Never | Incidentally found on follow up for SLE | LLL | S | A 45-mm growing poorly-defined consolidative mass lesion | Wedge | PNLH with post-obstructive change | 4.5 | 18 | |
| DDx | |||||||||||||
| 1) Mucinous adenocarcinoma | |||||||||||||
| 2) Organizing pneumonia, less likely | |||||||||||||
| 7 | 39 | F | None | Ex 10 YA stop | Incidentally found | LLL | S | Wide ground-glass opacity lesion | Lobe | PNLH with post-obstructive change | 4.5 | 4 | |
| DDx | |||||||||||||
| 1) Invasive adenocarcinoma | |||||||||||||
| 2) Pneumonia | |||||||||||||
| 8 | 69 | F | None | Never | Incidentally found on health-exam | RUL | S | A 14-mm-sized oval nodular lesion | Segm | PNLH with post-obstructive change | 1.4 | 3 | |
| DDx | |||||||||||||
| 1) Benign nodule, more likely | |||||||||||||
| 2) i nvasive adenocarcinoma due to faint uptake on PET | |||||||||||||
| 9 | 59 | M | None | Ex 2 YA | Incidentally found on follow-up for emphysema | RLL | S | A 18-mm irregular nodular lesion with strong enhancement | Wedge | PNLH with post-obstructive change | 2 | 3 | |
| DDx | |||||||||||||
| 1) Focal organizing pneumonia | |||||||||||||
| 2) Hypervascular lung cancer | |||||||||||||
| No. | Border | Location | Pattern | Germinal centers | Lymphoepithelial lesions | Fibrosis | Plasma cell | Neutrophils | Histiocytes | Other findings |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Well-defined | Subpleural | Nodular | Present | Present | + | ++ | ++ | +++ | - |
| 2 | Well-defined | Subpleural | Diffuse | Present | Not definite | + | + | ++ | + | - |
| 3 | Irregular | Subpleural | Nodular | Present | Not definite | - | ++ | + | + | - |
| 4 | Irregular | Subpleural | Nodular | Present | Not definite | - | + | - | ++ | Aspergillosis |
| 5 | Well-defined | Subpleural | Diffuse | Present | Not definite | ++ | +++ | - | +++ | - |
| 6 | Well-defined | Subpleural | Diffuse | Present | Present | - | +++ | - | + | - |
| 7 | Well-defined | Subpleural | Diffuse | Present | Not definite | + | + | + | ++ | - |
| 8 | Well-defined | Subpleural | Nodular | Present | Not definite | ++ | +++ | + | ++ | - |
| 9 | Irregular | Subpleural | Diffuse | Present | Not definite | ++ | ++ | - | ++ | - |
| Pulmonary nodular lymphoma hyperplasia | Extranodal marginal zone lymphoma of MALT | |
|---|---|---|
| Clinical feature | Usually asymptomatic | Often asymptomatic |
| Cough and dyspnea | ||
| Radiographic finding | Single or multiple (rare), mass or mass-like area of consolidation | Single or multiple, mass and/or areas of consolidation |
| Histologic feature | ||
| Growth pattern | Nodular pattern | Diffuse or nodular pattern |
| Component | Mixed cell population, reactive germinal center, and fibrosis | Small lymphocytes which indistinguishable from mature lymphocytes |
| Often monocytoid B-cells | ||
| May be follicular colonization | ||
| Lymphoepithelial lesion | Rare, often | Common |
| Ducther body | Absent | Common with plasmacytoid differentiation |
| Pleural or bronchus invasion | Absent | Frequent |
| Ancillary test | ||
| Immunohistochemistry | Reactive pattern, having well preserved germinal center | Diffuse pattern in B-cell marker |
| High proliferative activity in germinal center | Low proliferative activity | |
| IgH gene rearrangement test | Polyclonal | Monoclonal |
TB, tuberculosis; S, solitary; M, multiple; Dx, diagnosis; F, female; GGO, ground glass opacity; LUL, left upper lobe; DDx, differential diagnosis; MALT, mucosaassociated lymphoid tissue; R/O, rule out; Segm, segmentectomy; PNLH, pulmonary nodular lymphoid hyperplasia; YA, years ago; RLL, right lower lobe; Lobe, lobectomy; LLL, left lower lobe; Wegde, wedge resection; SLE, systemic lupus erythematosus; EX, ex-smoker; RUL, right upper lobe; PET, positron emission tomography.

