 E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 46(6); 2012 > Article
-
Case Report
Adenolipoma of the Skin Arising at Neck Region - Hyun Seung Lee, Yoon Sang Song1
-
Korean Journal of Pathology 2012;46(6):587-589.
DOI: https://doi.org/10.4132/KoreanJPathol.2012.46.6.587
Published online: December 26, 2012
Department of Pathology, Yangji General Hospital, Seoul, Korea.
1Department of Plastic Surgery, Cheju Halla General Hospital, Jeju, Korea.
- Corresponding Author: Hyun Seung Lee, M.D. Department of Pathology, Yangji General Hospital, 1636 Nambusunhwan-ro, Gwanak-gu, Seoul 151-852, Korea. Tel: +82-70-4665-9341, Fax: +82-2-879-1610, laghonda@naver.com
• Received: January 13, 2012 • Revised: February 22, 2012 • Accepted: March 7, 2012
© 2012 The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
- We report here a case of adenolipoma of the skin, an unusual variant of lipoma, arising on the neck. A 56-year-old man visited our hospital due to an anterior neck mass. An excisional biopsy was performed. The mass revealed a tan-yellow soft cut surface. We could not find any difference from other lipoma on gross inspection. Microscopically, the mass showed proliferation of mature adipocytes admixed with several eccrine units. The eccrine units were demonstrated by periodic acid-Schiff-positive granules in the secretory portions and by positivity of smooth muscle actin in the myoepithelial cells surrounding the eccrine glands. The tumor was completely excised, and the patient has been followed up without any evidence of recurrence so far.
- A 56-year-old man was admitted to our hospital because of an anterior neck mass. It had been slowly growing over several years. The patient had no other specific history, including familial history, and had good general status. On the physical examination, an approximately 4.0 cm movable, non-painful, and soft mass on the anterior neck was observed. A neck computerized tomography showed a small fatty mass at the subcutaneous tissue of the anterior neck. An excisional biopsy was performed. On gross examination, the tumor was soft, tan-yellow, and lobulated (Fig. 1). Microscopically, it showed many lobules of mature adipose tissue with fine fibrous septa. A few clusters of eccrine units were entrapped in the adipose tissue (Fig. 2). At times, the eccrine ducts showed partly cystic dilatation. The adipocytes and eccrine glands had no cytologic atypia, necrosis, or mitosis. Periodic acid-Schiff (PAS) stain was positive in the secretory granules and intraluminal secretions of the eccrine glands (Fig. 3A). On immunohistochemistry, the myoepithelial cells surrounding the eccrine glands were positive for smooth muscle actin (Fig. 3B).
- A complete excision was performed. The patient was well and without recurrence, for one year after surgery.
CASE REPORT
- Hitchcock et al.3 first described adenolipoma of the skin. They proposed the name "adenolipoma of the skin" due to the presence of eccrine sweat glands in the benign tumors of adipose tissues.
- Daboin et al.5 reported on 6 patients with adenolipomas of the head and neck region: 3 in the parathyroid, 2 in the thyroid, and 1 in the parotid gland. The microscopic features of adenolipomas arising in the thyroid gland showed neoplasm surrounded by a fibrous capsules and were also composed of fat and thyroid follicles. The adenolipomas of the parathyroid gland were also an intimate admixture of mature adipocytes and small chief cells arranged in nests and acini. It is the author's conclusion that the concept of adenolipoma is an admixture of mature fat tissues, which are the main components of common lipoma, and glandular tissue, which are present at each of the viscera and in the tissues where the tumor occurs. Our case was a variant of superficial lipoma that was characterized by the presence of eccrine sweat glands. Eventually, we were able to diagnose this case as adenolipoma of the skin due to the eccrine glands of the skin adnexa entrapped in the mature adipocytes.
- Adenolipoma of the skin presents as a solitary, slow-growing, and painless tumor.3 The main sites in which the tumor occurs include the thigh, shoulder, thorax, and upper extremities. The tumor size varies from 1.0 cm to 6.0 cm in diameter.4
- Conventionally, adenolipomas of the skin consist of a proliferation of mature adipocytes admixed with several benign-looking eccrine glands and ducts. Our case was also similar to the typical morphology. However, according to the previous report by Kazakov et al.,1 adenolipoma of the skin has a conventional lipomatous component, but the lipomatous component may also correspond to the lipomatous component of spindle cell lipoma. The eccrine gland and duct can be observed in various morphologies; including cystic duct dilatation, epithelial hyperplasia, and clear cell or squamous metaplasia.1
- The differential diagnosis of adenolipoma of the skin includes common lipoma, eccrine angiomatous harmatoma,2,6 and nevus lipomatous superficialis.2,7 Adenolipoma is observed with a similar clinical manifestation to common lipoma, but adenolipoma looks a little smaller and may be more common in older age compared with common lipoma.2 Eccrine angiomatous harmatoma is a developmental disorder and is typically a solitary lesion on lower extremities. Histologically, eccrine angiomatous hamartomas usually occur in the deep dermis and contain an increased number of eccrine structures and numerous capillary channels surrounding or intermingled with the eccrine structures.6 Nevus lipomatous superficialis shows groups of soft and flattened papules or nodules that have smooth or wrinkled surfaces. On histopathologic findings, nevus lipomatous superficialis is characterized by groups and strands of fat cells embedded among the collagen bundles of the dermis.2,7
- Because adenolipoma of the skin is an extremely rare tumor, we need to prove whether the glands and ducts entrapped in the mature adipocytes are true skin adnexal components. Eccrine glands are composed of secretory cells and surrounding myoepithelial cells. The intracytoplasmic granules and intraluminal secretions of secretory cells lining the lumen are PAS-positive. Myoepithelial cells surrounding eccrine glans are positive immunohistochemically for smooth muscle actin, p63 and S-100 protein. Therefore, these special and immunohistochemical stainings are helpful in diagnosis.
- The treatement and prognosis of adenolipomas are the same as that of common lipoma because they are considered to be benign. Surgical excision is the treatment of choice.
DISCUSSION
- 1. Kazakov DV, Spagnolo DV, Kacerovska D, Kempf W, Michal M. Cutaneous adenolipoma: extending the spectrum of changes in the lipomatous and epithelial components. Am J Dermatopathol 2011; 33: 56-59. ArticlePubMed
- 2. Kim TH, Choi YJ, Nam JH, Lee GY, Kim WS, Kim KJ. A case of adenolipoma. Korean J Dermatol 2008; 46: 1548-1550.
- 3. Hitchcock MG, Hurt MA, Santa Cruz DJ. Adenolipoma of the skin: a report of nine cases. J Am Acad Dermatol 1993; 29: 82-85. ArticlePubMed
- 4. Del Agua C, Felipo F. Adenolipoma of the skin. Dermatol Online J 2004; 10: 9.
- 5. Daboin KP, Ochoa-Perez V, Luna MA. Adenolipomas of the head and neck: analysis of 6 cases. Ann Diagn Pathol 2006; 10: 72-76. ArticlePubMed
- 6. Sanmartin O, Botella R, Alegre V, Martinez A, Aliaga A. Congenital eccrine angiomatous hamartoma. Am J Dermatopathol 1992; 14: 161-164. ArticlePubMed
- 7. Dotz W, Prioleau PG. Nevus lipomatosus cutaneus superficialis: a light and electron microscopic study. Arch Dermatol 1984; 120: 376-379. ArticlePubMed
REFERENCES
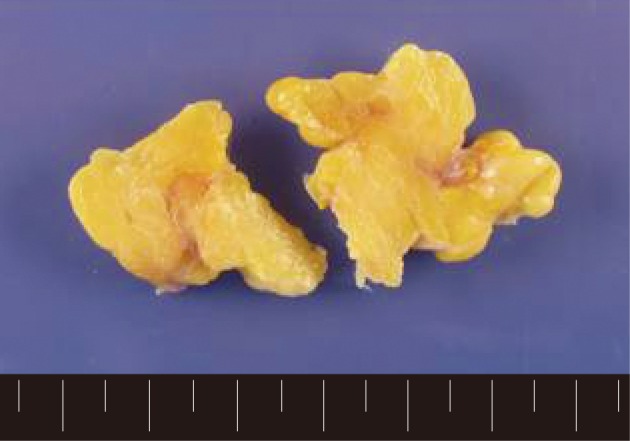
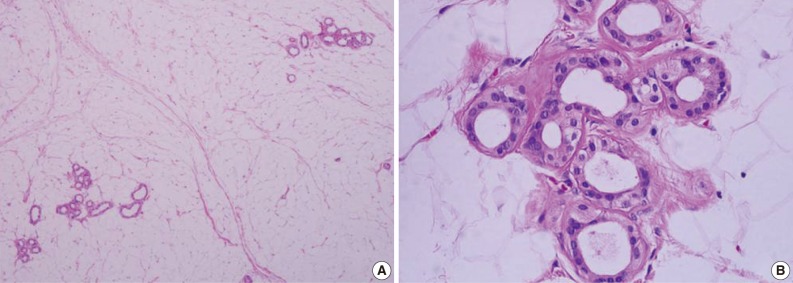
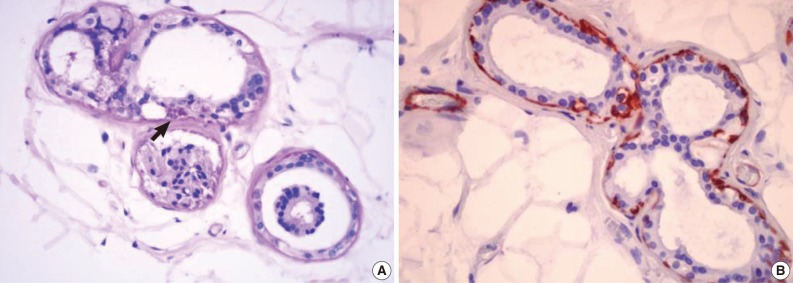
Figure & Data
References
Citations
Citations to this article as recorded by 
- Adenolipoma of the Skin: A Report of 11 Cases
Rawan Amir, Salwa Sheikh
Case Reports in Dermatology.2018; 10(1): 76. CrossRef
 PubReader
PubReader Cite this Article
Cite this Article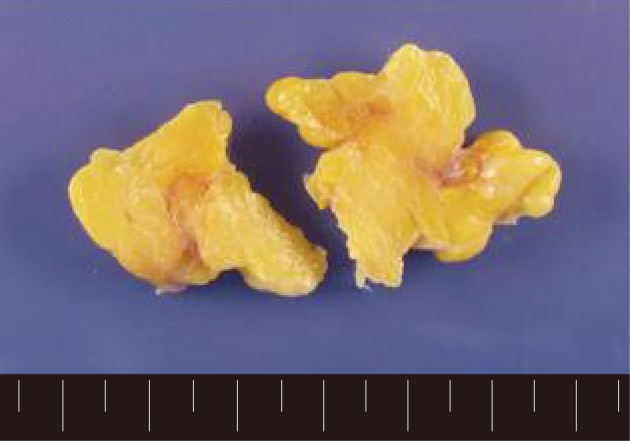
Adenolipoma of the Skin Arising at Neck Region



Fig. 1 The gross specimen of the adenolipoma shows a multinodular tan-yellow soft cut surface.
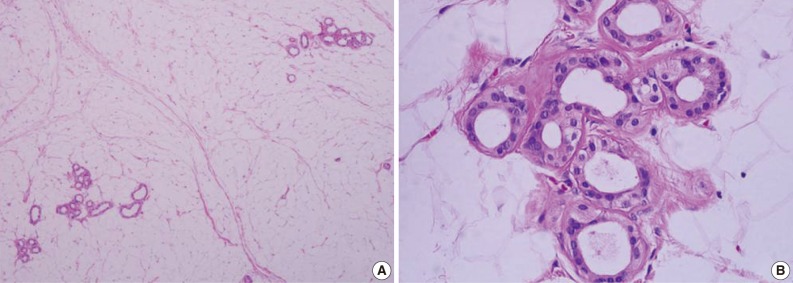
Fig. 2 (A) The tumor is composed of mature fat cells admixed with small clustered eccrine units. (B) The lumens of the secretory portion of the eccrine gland are detected at high magnification.
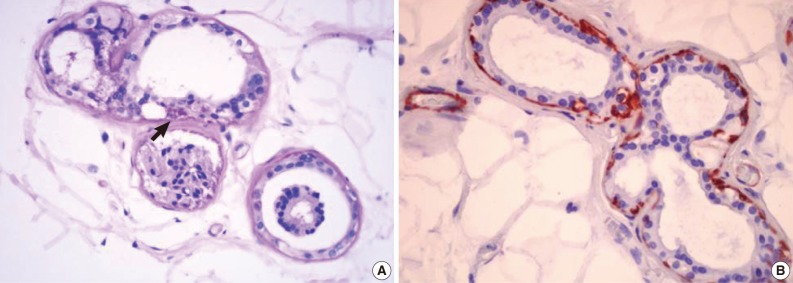
Fig. 3 (A) Periodic acid-Schiff (PAS)-positive intracytoplasmic granules (arrow) and intraluminal secretions are found in the secretory portion of the eccrine gland. (B) The myoepithelial cells are immunoreactive for smooth muscle actin.
Fig. 1
Fig. 2
Fig. 3
Adenolipoma of the Skin Arising at Neck Region

