E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 56(2); 2022 > Article
-
Letter to the Editor
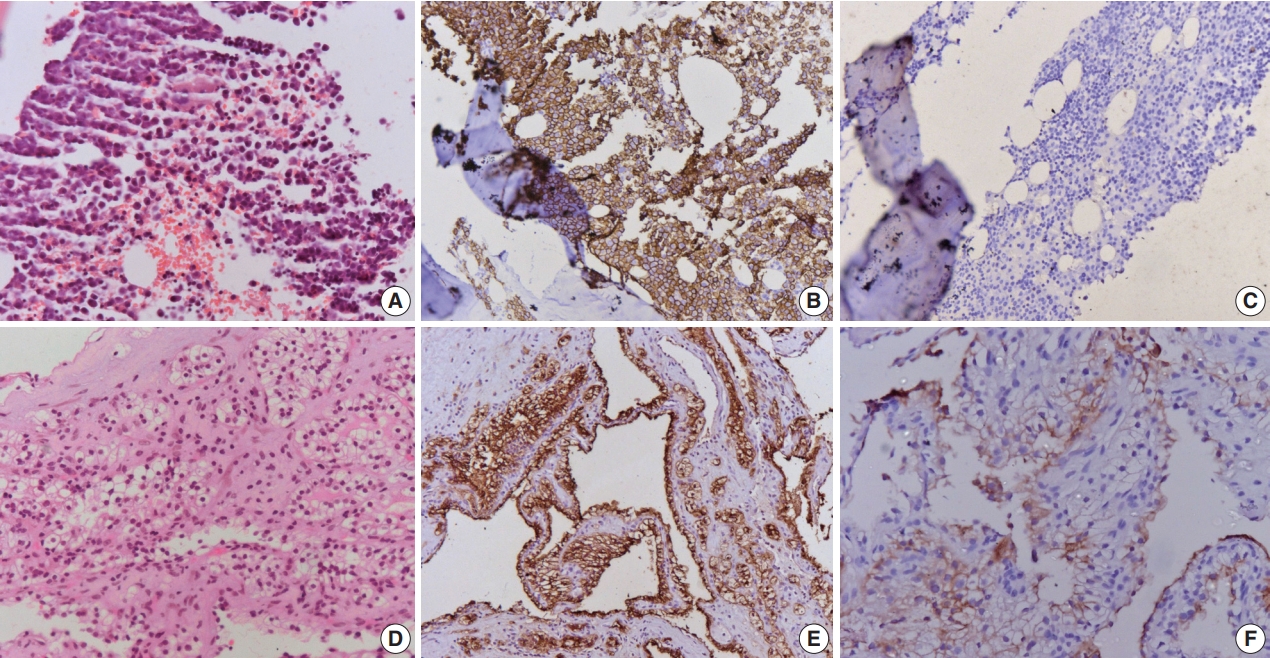
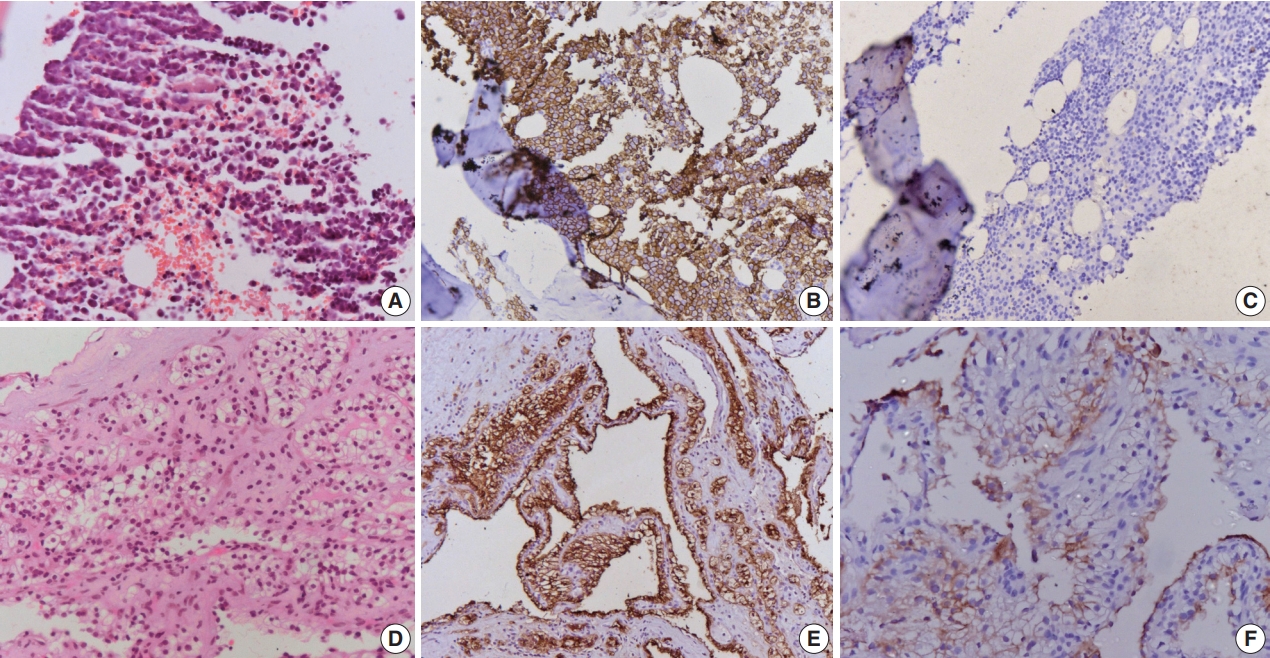
Renal cell carcinoma concomitant with multiple myeloma -
Anubhav Narwal1
 , Prashant Ramteke1, Lalit Kumar2, Saumyaranjan Mallick,1
, Prashant Ramteke1, Lalit Kumar2, Saumyaranjan Mallick,1 -
Journal of Pathology and Translational Medicine 2022;56(2):111-112.
DOI: https://doi.org/10.4132/jptm.2022.01.21
Published online: March 11, 2022
1Department of Pathology, All India Institute of Medical Sciences, New Delhi, India
2Department of Medical Oncology, All India Institute of Medical Sciences, New Delhi, India
- Corresponding Author: Saumyaranjan Mallik, MD Department of Pathology, All India Institutes of Medical Sciences (AIIMS), New Delhi 110029, India Tel: +91-9013957818, Fax: +91-11-26588663, E-mail: drsmallick.aiims@gmail.com
© 2022 The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Ethics Statement
Not applicable.
Availability of Data and Material
Availability of Data and Material: Data sharing not applicable to this article as no datasets were generated or analyzed during the study.
Code Availability
Not applicable.
Author contributions
Conceptualization: SM. Data curation: AN. Formal analysis: AN. Investigation: LK. Methodology: PR. Writing—original draft: AN, PR. Writing—review & editing: SM. Approval of final manuscript: all authors.
Conflicts of Interest
The authors declare that they have no potential conflicts of interest.
Funding Statement
No funding to declare.
- 1. Ojha RP, Evans EL, Felini MJ, et al. The association between renal cell carcinoma and multiple myeloma: insights from population-based data. BJU Int 2011; 108: 825-30. ArticlePubMed
- 2. Shields LB, Kalebasty AR. Concurrent renal cell carcinoma and hematologic malignancies: Nine case reports. World J Clin Oncol 2020; 11: 644-54. ArticlePubMedPMC
- 3. Li N, Liu X, Song Y, et al. The synchronous presence of multiple myelomas and other primary malignant tumors: case series with literature review. Cancer Manag Res 2020; 12: 2829-38. PubMedPMC
- 4. Sakai A, Kawano M, Kuramoto A. Interleukin-6 produced by renalcell carcinoma cells and progression of multiple myeloma. N Engl J Med 1991; 324: 1893-4. ArticlePubMed
- 5. Choueiri TK, Baz RC, McFadden CM, et al. An association between renal cell carcinoma and multiple myeloma: a case series and clinical implications. BJU Int 2008; 101: 712-5. ArticlePubMed
- 6. Padhi S, Sahoo PK, Banerjee D, et al. Renal cell carcinoma and plasma cell myeloma: unique association and clinical implications. Urol Ann 2014; 6: 252-6. ArticlePubMedPMC
REFERENCES
Figure & Data
References
Citations
- Autologous stem cell transplant for multiple myeloma: Impact of melphalan dose on the transplant outcome
Lalit Kumar, Ranjit Kumar Sahoo, Sudhir Kumar, Annie K. Baa, Ghazal Tansir, Neha Pathak, Prabhat S. Malik, Om Dutt Sharma, Anisha Mathew, Ankit Jha, Ritu Gupta, Atul Sharma, Ahitagni Biswas, Rakesh Kumar, Sanjay Thulkar, Soumyaranjan Malik, Ashish Dutt
Leukemia & Lymphoma.2023; 64(2): 378. CrossRef
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-