E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 53(4); 2019 > Article
-
Brief Case Report
Endocervical Adenocarcinoma In Situ Phenotype with Ovarian Metastasis -
Hyun-Soo Kim
 , Yeon Seung Chung, Moon Sik Kim, Hyang Joo Ryu, Ji Hee Lee
, Yeon Seung Chung, Moon Sik Kim, Hyang Joo Ryu, Ji Hee Lee -
Journal of Pathology and Translational Medicine 2019;53(4):270-272.
DOI: https://doi.org/10.4132/jptm.2018.12.17
Published online: December 28, 2018
Department of Pathology, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea
- Corresponding Author Hyun-Soo Kim, MD, PhD Department of Pathology, Severance Hospital, Yonsei University College of Medicine, 50-1 Yonsei-ro, Seodaemun-gu, Seoul 03722, Korea Tel: +82-2-2228-1794, Fax: +82-2-362-0860, E-mail: hyunsookim@yuhs.ac
© 2019 The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
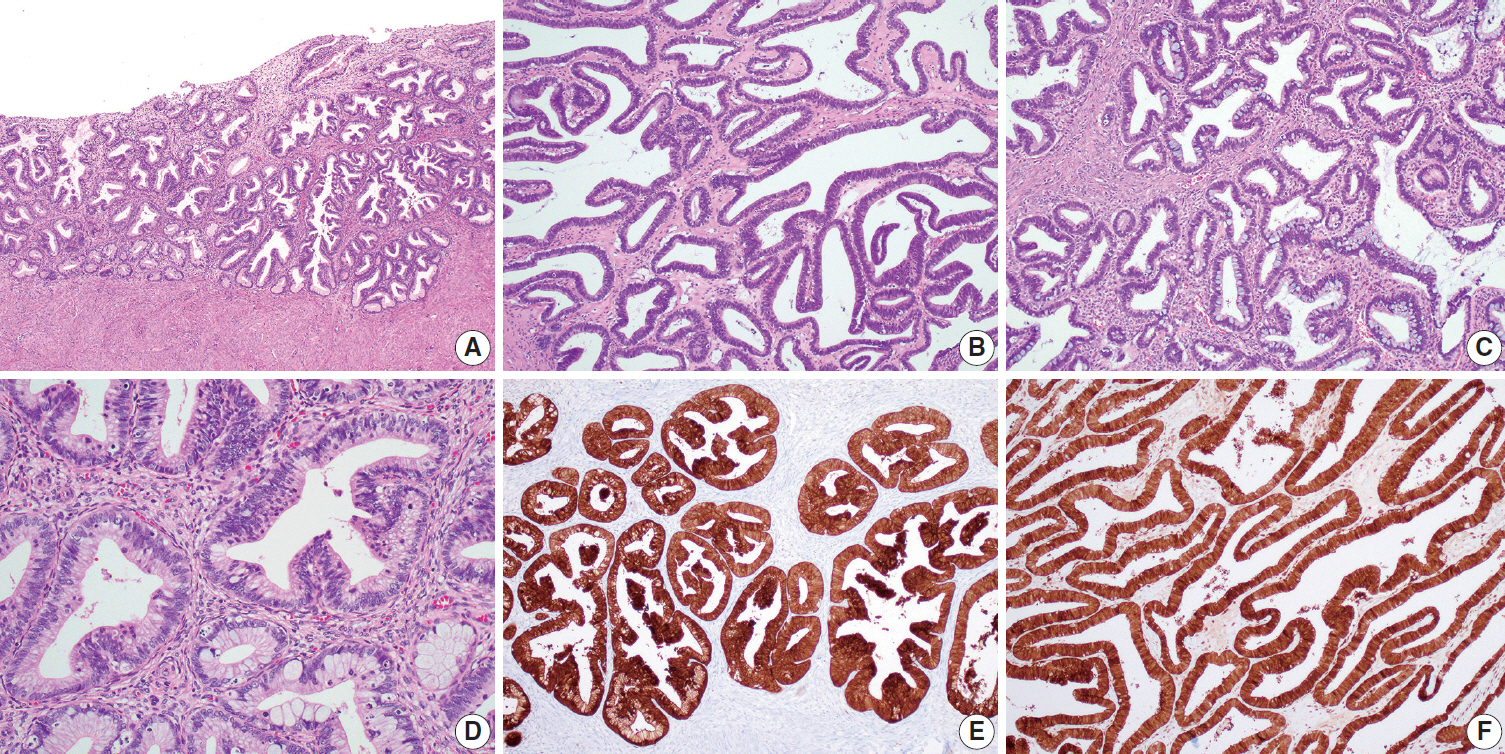
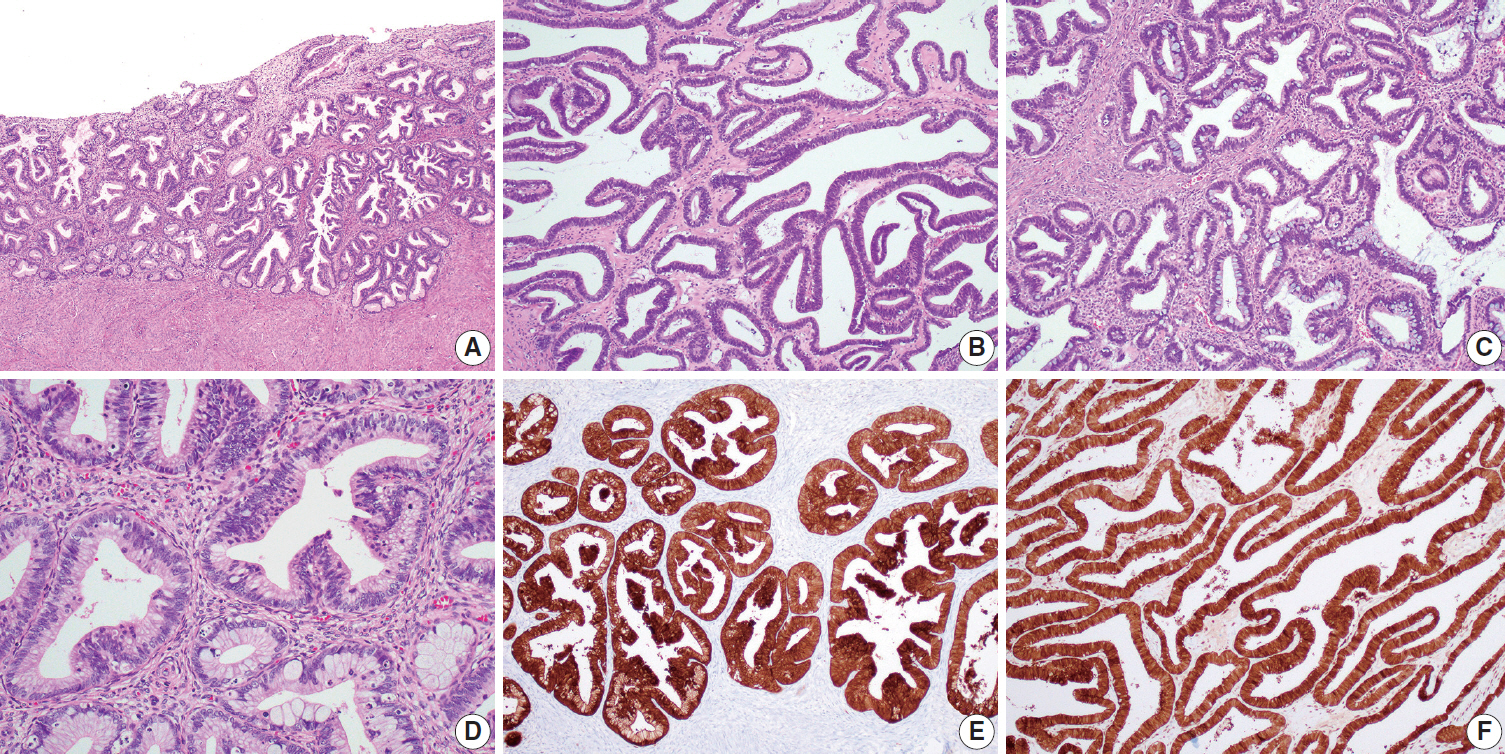
- A 45-year-old woman presented with a left ovarian mass 65 months following diagnosis of endocervical AIS (Fig. 1A) from a punch biopsy and treated with an extended abdominal hysterectomy. She underwent left salpingo-oophorectomy and the left ovarian mass measured 7.0 cm in diameter, had a smooth surface, and was solid and cystic. The inner surface of the cystic lesion varied from smooth to rough with several nodules. Histologically, the tumor displayed confluent glandular architectures with primarily endometrioid-like (Fig. 1B) and focally mucinous (Fig. 1C) differentiation. Nuclei were enlarged and hyperchromatic with occasional mitotic figures and apoptotic bodies (Fig. 1D). There was no stromal invasion. The ovarian tumor was thought to represent an independent borderline endometrioid tumor. We reviewed slides obtained from the hysterectomy specimen, and concerns were raised for metastasis due to the histological similarity between the endocervical and ovarian lesions. Immunostaining for p16 and HPV genotyping were performed. Both endocervical (Fig. 1E) and ovarian (Fig. 1F) lesions exhibited strong and diffuse p16 expression and had identical HPV type 45. Based on these findings, the left ovarian tumor was diagnosed as metastatic endocervical adenocarcinoma. This study was approved by the Institutional Review Board of Severance Hospital with a waiver of informed consent (4-2018-0724).
CASE REPORT
- When histologically similar malignant tumors occur at two locations, it is difficult to determine whether each is an independent primary tumor, or whether one represents a metastasis from the other [5]. The concurrence of endocervical adenocarcinoma and ovarian tumor is quite uncommon, and the diagnostic difficulties encountered have received little attention. The majority of cases with ovarian involvement occur in advanced-stage endocervical adenocarcinoma or in a primary lesion with extrauterine extension [6]. However, there have been cases of early-stage disease, and even cases of noninvasive carcinoma, that involved the ovary [1,2,5,7]. Most ovarian lesions show well-differentiated villoglandular and confluent glandular patterns, resembling those of primary ovarian borderline mucinous or endometrioid tumor [2]. In a previous study, all cases examined were initially thought to represent independent primary ovarian epithelial tumors, including borderline tumors or grade 1 carcinomas of mucinous or endometrioid type [8]. In cases with no stromal invasion in an endocervical adenocarcinoma, a borderline-appearing ovarian tumor could reasonably be interpreted as an independent primary ovarian tumor by the pathologist [7]. In this situation, the presence of the identical HPV type in both the endocervical and ovarian tumors supports that the ovarian lesion is a metastatic endocervical adenocarcinoma rather than an independent primary ovarian tumor. Studies associating HPV and ovarian tumors have yielded almost universally negative results, suggesting that primary ovarian tumors are etiologically unrelated to HPV infection [7]. In addition, p16 immunostaining may prove useful for distinguishing metastases from primary ovarian tumors. p16 immunoreactivity is a surrogate marker of high-risk HPV infection [9]. Although p16 expression is absent or sporadically positive in ovarian mucinous and endometrioid carcinomas, HPV-related endocervical tumors typically display strong and diffuse nuclear p16 immunoreactivity. In conjunction with clinicopathological features, p16 expression in ovarian lesions is associated with high-risk HPV and supports the diagnosis of metastatic endocervical adenocarcinoma.
- In summary, we present a case of endocervical AIS involving the ovary. Notably, minimal to no stromal invasion in endocervical adenocarcinoma does not exclude the possibility of metastasis to the ovary. Cases of concurrent endocervical AIS and ovarian tumor, although rare, prompt thorough sampling of the endocervix to exclude stromal invasion. Careful morphological evaluation and use of ancillary tests promote an accurate diagnosis. p16 immunostaining and HPV testing of ovarian lesions may be confirmatory if positive.
DISCUSSION
Author Contributions
Conceptualization: HSK.
Data curation: YSC.
Formal analysis: YSC, MSK, HJR, JHL.
Funding acquisition: HSK.
Investigation: HSK, YSC.
Methodology: MSK, HJR, JHL.
Project administration: HSK.
Resources: HSK, YSC.
Software: HSK.
Supervision: HSK.
Validation: MSK, HJR, JHL.
Visualization: HSK.
Writing—original draft: HSK, YSC.
Writing—review & editing: HSK, YSC, MSK, HJR, JHL.
Conflicts of Interest
The authors declare that they have no potential conflicts of interest.
Acknowledgments
- 1. Chang MC, Nevadunsky NS, Viswanathan AN, Crum CP, Feltmate CM. Endocervical adenocarcinoma in situ with ovarian metastases: a unique variant with potential for long-term survival. Int J Gynecol Pathol 2010; 29: 88-92. ArticlePubMed
- 2. Turashvili G, Farmer P, Colgan T, Childs T. Human papillomavirus-related ovarian metastasis with endocervical adenocarcinoma: report of 2 cases and review of literature. J Low Genit Tract Dis 2015; 19: e60-3. PubMed
- 3. Yada-Hashimoto N, Yamamoto T, Kamiura S, et al. Metastatic ovarian tumors: a review of 64 cases. Gynecol Oncol 2003; 89: 314-7. ArticlePubMed
- 4. McCluggage WG, Wilkinson N. Metastatic neoplasms involving the ovary: a review with an emphasis on morphological and immunohistochemical features. Histopathology 2005; 47: 231-47. ArticlePubMed
- 5. Khor TS, Brennan BA, Leung YC, Sengupta S, Stewart CJ. Cervical adenocarcinoma metastatic to the ovary mimicking primary ovarian carcinoma. Pathology 2009; 41: 397-400. ArticlePubMed
- 6. Reyes C, Murali R, Park KJ. Secondary involvement of the adnexa and uterine corpus by carcinomas of the uterine cervix: a detailed morphologic description. Int J Gynecol Pathol 2015; 34: 551-63. PubMedPMC
- 7. Ronnett BM, Yemelyanova AV, Vang R, et al. Endocervical adenocarcinomas with ovarian metastases: analysis of 29 cases with emphasis on minimally invasive cervical tumors and the ability of the metastases to simulate primary ovarian neoplasms. Am J Surg Pathol 2008; 32: 1835-53. PubMed
- 8. Elishaev E, Gilks CB, Miller D, Srodon M, Kurman RJ, Ronnett BM. Synchronous and metachronous endocervical and ovarian neoplasms: evidence supporting interpretation of the ovarian neoplasms as metastatic endocervical adenocarcinomas simulating primary ovarian surface epithelial neoplasms. Am J Surg Pathol 2005; 29: 281-94. PubMed
- 9. Vang R, Gown AM, Farinola M, et al. p16 expression in primary ovarian mucinous and endometrioid tumors and metastatic adenocarcinomas in the ovary: utility for identification of metastatic HPV-related endocervical adenocarcinomas. Am J Surg Pathol 2007; 31: 653-63. PubMed
REFERENCES
Figure & Data
References
Citations
- Endocervical adenocarcinoma in situ with ovarian metastases
Kate Glennon, Ann Treacy, Tony Geoghegan, Paul Downey, Donal Brennan
International Journal of Gynecological Cancer.2022; 32(4): 566. CrossRef - Concurrent metastatic ovarian adenocarcinoma of endocervical adenocarcinoma in situ: A case report emphasizing pathologic diagnostic key points and clinical progress
In Ok Lee, Yee Jung Kim, Hanna Moon, Jae Eun Chung
Gynecologic Oncology Reports.2021; 36: 100766. CrossRef - Peritoneal HPV‐DNA test in cervical cancer (PIONEER study): A proof of concept
Nicolò Bizzarri, Luigi Pedone Anchora, Paola Cattani, Rosa De Vincenzo, Simona Marchetti, Carmine Conte, Vito Chiantera, Valerio Gallotta, Salvatore Gueli Alletti, Giuseppe Vizzielli, Barbara Costantini, Anna Fagotti, Francesco Fanfani, Giovanni Scambia,
International Journal of Cancer.2021; 148(5): 1197. CrossRef - Cervical stromal involvement by endometrial ‘hyperplasia’: a previously unreported phenomenon with recommendations to report as stage II endometrial carcinoma
Jennifer Taylor, W. Glenn McCluggage
Pathology.2021; 53(5): 568. CrossRef - Pelvic and Ovarian Recurrence of Small HPV-associated Cervical Adenocarcinoma With Transformation to Neuroendocrine Carcinoma
Duaa Abu-Sinn, Jackie Jamison, Matthew Evans, W. Glenn McCluggage
International Journal of Gynecological Pathology.2021; 40(6): 541. CrossRef - Superficially Spreading Endocervical Adenocarcinoma in situ with Multifocal Microscopic Involvement of the Endometrial Surface: A Case Report with Emphasis on the Potential for Misdiagnosis Based on Endometrial Curettage Specimens
Inwoo Hwang, Jiyeon Lee, Kyue-Hee Choi, Jiheun Han, Hyun-Soo Kim
Case Reports in Oncology.2020; 13(3): 1530. CrossRef
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-