 E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 57(4); 2023 > Article
-
Original Article
Loss of aquaporin-1 expression is associated with worse clinical outcomes in clear cell renal cell carcinoma: an immunohistochemical study -
Seokhyeon Lee1
 , Bohyun Kim2, Minsun Jung3, Kyung Chul Moon1,4
, Bohyun Kim2, Minsun Jung3, Kyung Chul Moon1,4 -
Journal of Pathology and Translational Medicine 2023;57(4):232-237.
DOI: https://doi.org/10.4132/jptm.2023.06.17
Published online: July 11, 2023
1Department of Pathology, Seoul National University College of Medicine, Seoul, Korea
2Department of Pathology, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea
3Department of Pathology, Yonsei University College of Medicine, Seoul, Korea
4Kidney Research Institute, Medical Research Center, Seoul National University College of Medicine, Seoul, Korea
- Corresponding Author: Kyung Chul Moon, MD, PhD, Department of Pathology, Kidney Research Institute, Medical Research Center, Seoul National University College of Medicine, 103 Daehak-ro, Jongno-gu, Seoul, Korea Tel: +82-2-740-8380, Fax: +82-2-743-5530, E-mail: blue7270@snu.ac.kr
© 2023The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
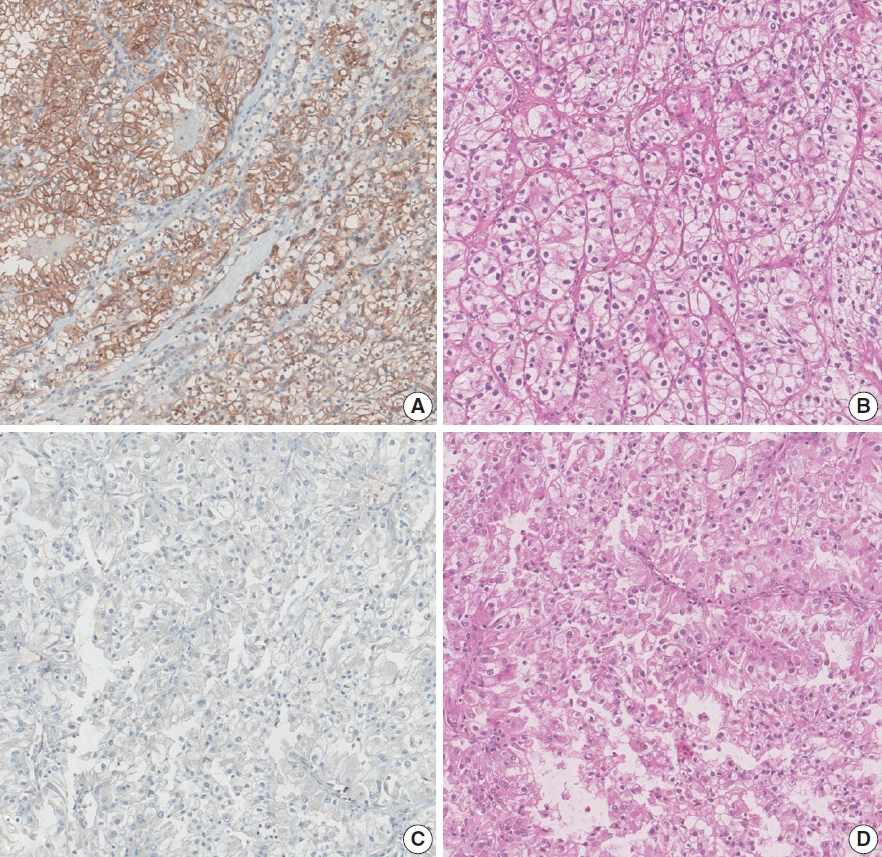

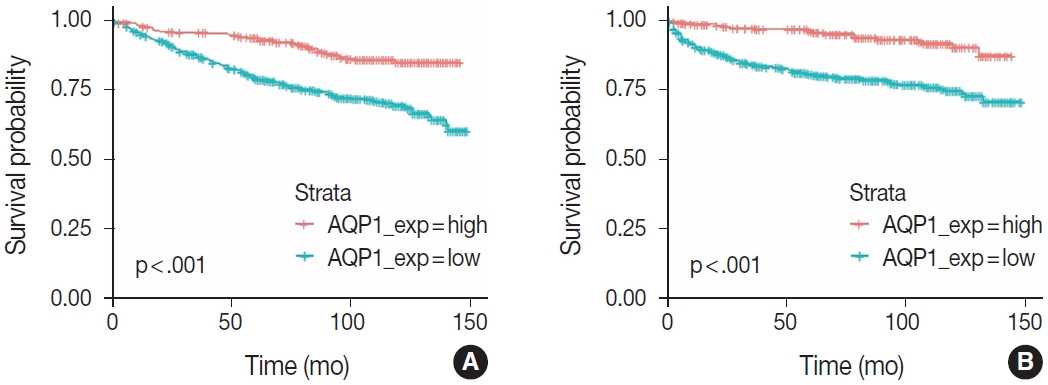
Figure & Data
References
Citations
- Loss of Aquaporin-1 in Tumor Cells Fosters Intrahepatic Cholangiocarcinoma Progression
César I. Gaspari, Carine Beaupere, Seth Richard, Estanislao Peixoto, Bouchra Lekbaby, Mirko Minini, Branko Dubravcic, Javier Vaquero, Marie Vallette, Ander Arbelaiz, Marion Janona, Corentin Louis, Pauline Le Gall, Cédric Coulouarn, Julieta Marrone, Juan E
The American Journal of Pathology.2026; 196(2): 428. CrossRef - Construction and validation of renal cell carcinoma tumor cell differentiation-related prognostic classification (RCC-TCDC): an integrated bioinformatic analysis and clinical study
Yifan Liu, Keqin Dong, Yuntao Yao, Bingnan Lu, Lei Wang, Guo Ji, Haoyu Zhang, Zihui Zhao, Xinyue Yang, Runzhi Huang, Wang Zhou, Xiuwu Pan, Xingang Cui
Annals of Medicine.2025;[Epub] CrossRef - Prognostic Assessment of Aquaporins in Pancreatic Adenocarcinoma: An In Silico Analysis
Vignesh Krishnasamy, Lalhmingliana, Nachimuthu Senthil Kumar
Current Biotechnology.2025; 14(2): 130. CrossRef - Targeting PLOD2 induces epithelioid differentiation and improves therapeutic response in sarcomatoid renal cell carcinoma
Xiangyu Chen, Dongkui Xu, Yu Ji, Xichen Dong, Xiaomei Dong, Zihan Li, Jingyu Tan, Qianqian Sun, Huixian Xin, Ziwei Liu, Qing Deng, Tao Wen, Yanjun Jia, Xuhui Zhu, Jian Liu
Journal of Advanced Research.2025;[Epub] CrossRef - Serum Exosomal MiR-874 as a Potential Biomarker for Nonsmall Cell Lung Cancer Diagnosis and Prognosis
Amal F. Gharib, Saad S. Al-Shehri, Abdulraheem Almalki, Ayman Alhazmi, Mamdouh Allahyani, Ahmed Alghamdi, Amani A. Alrehaili, Maha M. Bakhuraysah, Althobaiti Naif Saad M., Weal H. Elsawy
Indian Journal of Medical and Paediatric Oncology.2024;[Epub] CrossRef
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-

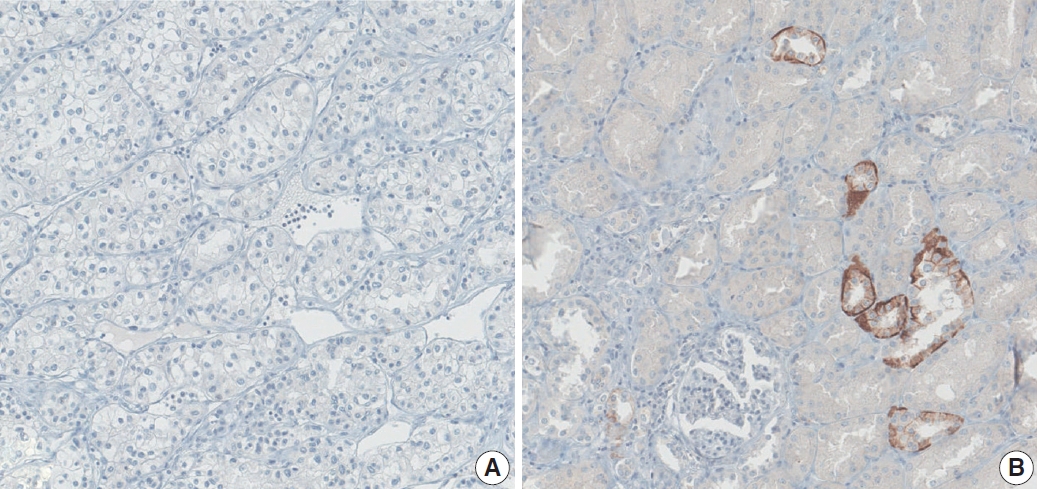
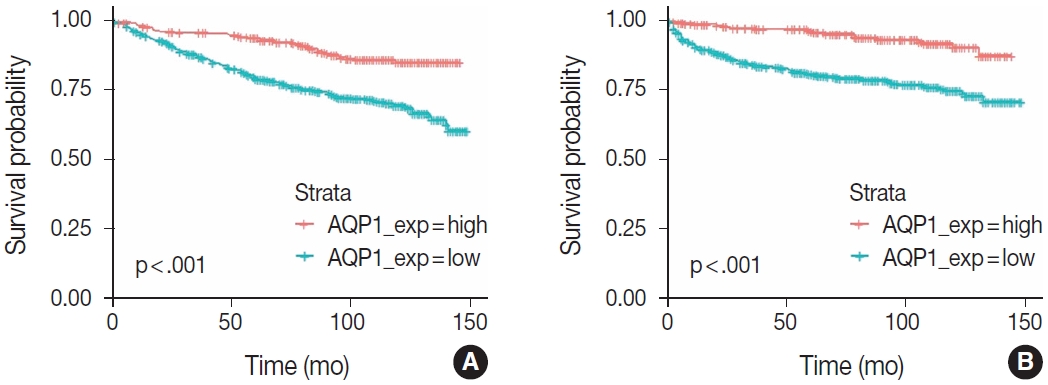
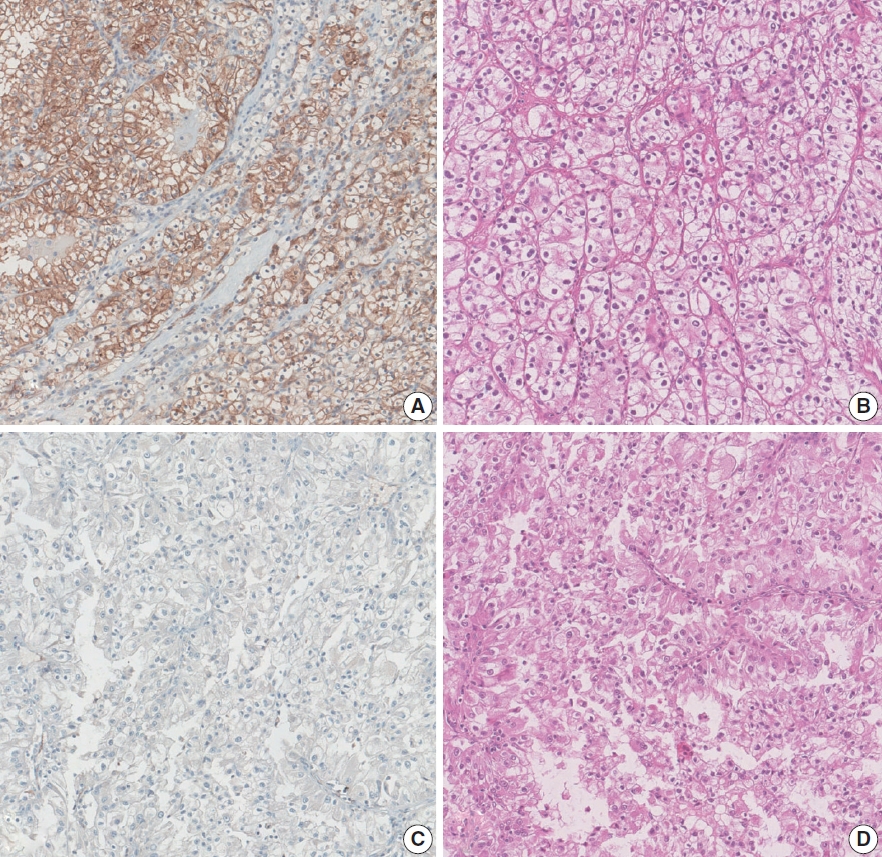
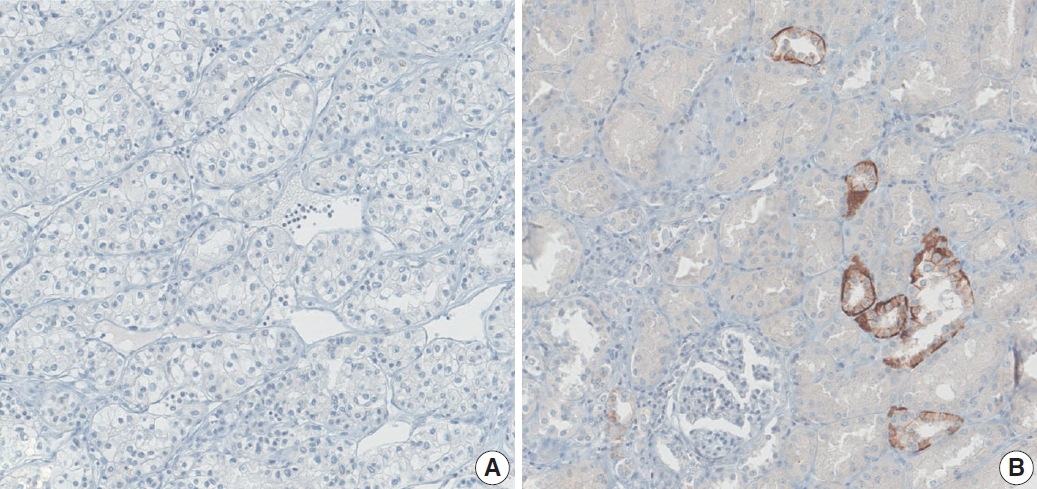

Fig. 1.
Fig. 2.
Fig. 3.
| Characteristic | Value |
|---|---|
| Age (yr) | 56.5 ± 12.3 |
| Sex (%) | |
| Male | 619 (74.9) |
| Female | 207 (25.1) |
| Tumor size (cm) | 4.2 ± 2.7 |
| TNM stage (%) | |
| Stage I | 637 (77.0) |
| Stage II | 34 (4.1) |
| Stage III | 96 (11.6) |
| Stage IV | 60 (7.3) |
| Nuclear grade (%) | |
| Grade 1 | 33 (4.0) |
| Grade 2 | 424 (51.3) |
| Grade 3 | 322 (38.9) |
| Grade 4 | 48 (5.8) |
| Survival (month) | |
| Overall survival | 91.8 ± 40.3 |
| Progression-free survival | 79.5 ± 42.4 |
| AQP1 expression (%) | |
| High | 320 (38.7) |
| Low | 507 (61.3) |
| Characteristics | No. (%) | Low AQP1 expression (%) | p-value |
|---|---|---|---|
| Age (yr) | |||
| ≥ 55 | 471 (57.0) | 67.3 | < .001 |
| < 55 | 356 (43.0) | 53.4 | |
| pTNM stage | |||
| I, II | 671 (81.1) | 55.4 | < .001 |
| III, IV | 156 (18.9) | 86.5 | |
| Nuclear grade | |||
| 1, 2 | 457 (55.3) | 50.5 | < .001 |
| 3, 4 | 370 (44.7) | 74.6 | |
| Distant metastasis | |||
| Present | 58 (7.0) | 86.2 | < .001 |
| Absent | 769 (93.0) | 59.4 | |
| Microvascular invasion | |||
| Present | 43 (5.2) | 0.9 | < .001 |
| Absent | 784 (94.8) | 7.9 |
| Prognostic factor | Overall survival |
Progression-free survival |
||
|---|---|---|---|---|
| Hazard ratio (95% CI) | p-value | Hazard ratio (95% CI) | p-value | |
| pTNM stage | ||||
| III, IV vs. I, II | 5.94 (4.45–7.94) | < .001 | 12.11 (8.45–17.36) | < .001 |
| Nuclear grade | ||||
| 3, 4 vs. 1, 2 | 2.95 (1.96–3.60) | < .001 | 5.02 (3.32–7.58) | < .001 |
| AQP1 expression | ||||
| Low vs. High | 2.58 (1.80–3.67) | < .001 | 3.65 (2.29–5.82) | < .001 |
| Prognostic factor | Overall survival |
Progression-free survival |
||
|---|---|---|---|---|
| Hazard ratio (95% CI) | p-value | Hazard ratio (95% CI) | p-value | |
| pTNM stage | ||||
| III, IV vs. I, II | 7.86 (5.25–11.78) | < .001 | 4.56 (3.27–6.34) | < .001 |
| Nuclear grade | ||||
| 3, 4 vs. 1, 2 | 1.98 (1.24–3.15) | .004 | 1.36 (0.96–1.92) | .086 |
| AQP1 expression | ||||
| Low vs. High | 1.85 (1.24–3.15) | .013 | 1.74 (1.20–2.50) | .003 |
Values are presented as mean ± standard deviation or number (%). AQP, aquaporin.
AQP, aquaporin; pTNM, pathological tumor–node–metastasis.
CI, confidence interval; pTNM, pathological tumor–node–metastasis; AQP, aquaporin.
CI, confidence interval; pTNM, pathological tumor–node–metastasis; AQP, aquaporin.

