 E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 57(4); 2023 > Article
-
Case Study
Intrathyroidal metastasis of tonsillar squamous cell carcinoma masquerading as a primary thyroid tumor -
Jai-Hyang Go

-
Journal of Pathology and Translational Medicine 2023;57(4):242-245.
DOI: https://doi.org/10.4132/jptm.2023.06.16
Published online: July 11, 2023
Department of Pathology, Dankook University College of Medicine, Cheonan, Korea
- Corresponding Author: Jai-Hyang Go, MD, Department of Pathology, Dankook University College of Medicine, 119 Dandae-ro, Dongnam-gu, Cheonan 31116, Korea Tel: +82-41-550-6974, Fax: +82-41-550-6034, E-mail: cyjy555@daum.net
© 2023The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
- Intrathyroidal metastasis of tonsillar squamous cell carcinoma is rare. To date, only six cases have been reported in the literature. This case was unusual and presented with thyromegaly before the diagnosis of the primary tumor. A 55-year-old male patient was suspected to have a primary thyroid tumor with nodal metastasis. The thyroid gland was diffusely enlarged, with no discernible mass. Histologically, the thyroid parenchyma revealed extensive endolymphatic tumor emboli, which were positive for p40 and p16 in a background of chronic lymphocytic thyroiditis. Positron emission tomography–computed tomography revealed hypermetabolic activity in the right tonsillar region. Tonsillar biopsy revealed human papillomavirus–positive squamous cell carcinoma. The present case is the first reported case of intrathyroidal metastasis of tonsillar squamous cell carcinoma with an initial clinical presentation of thyroid enlargement before the primary tumor of tonsillar cancer was diagnosed.
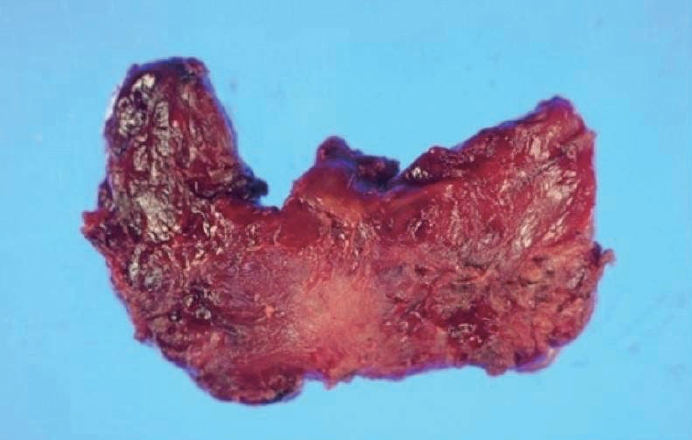
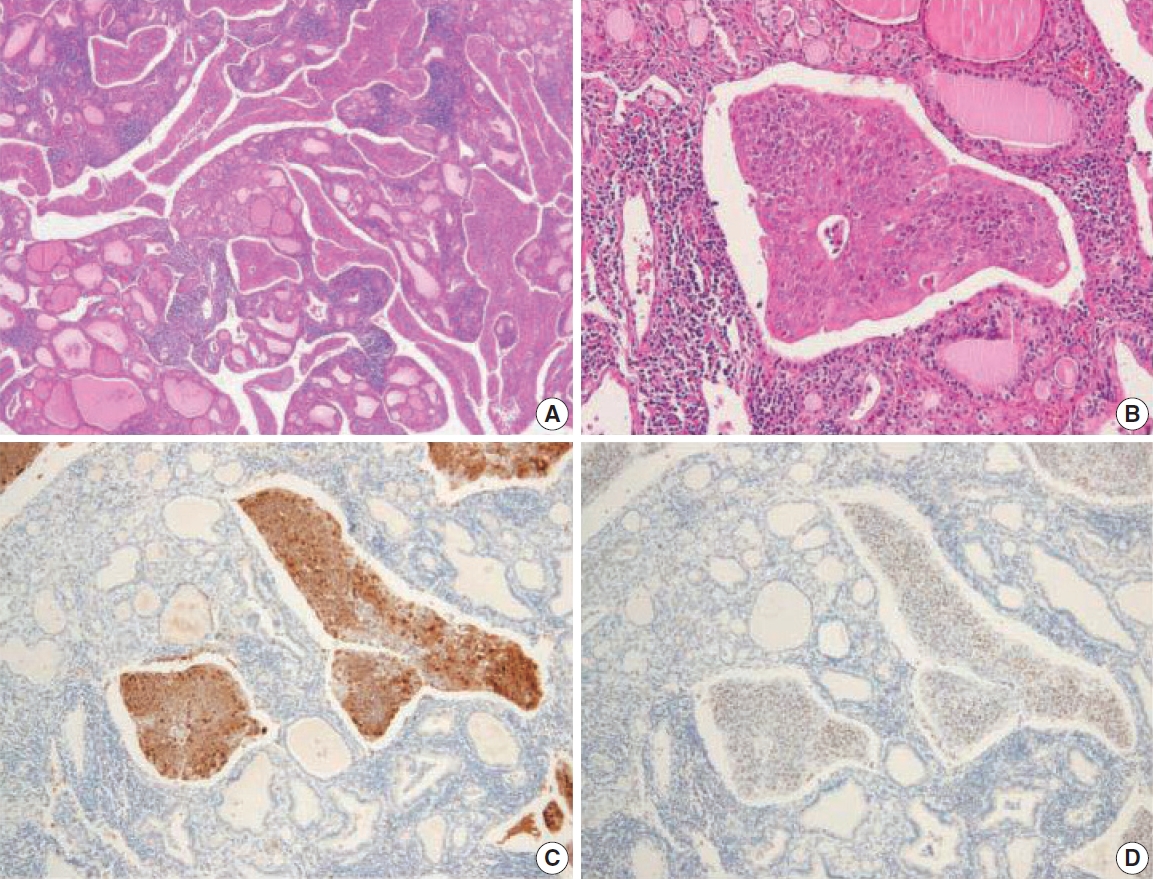
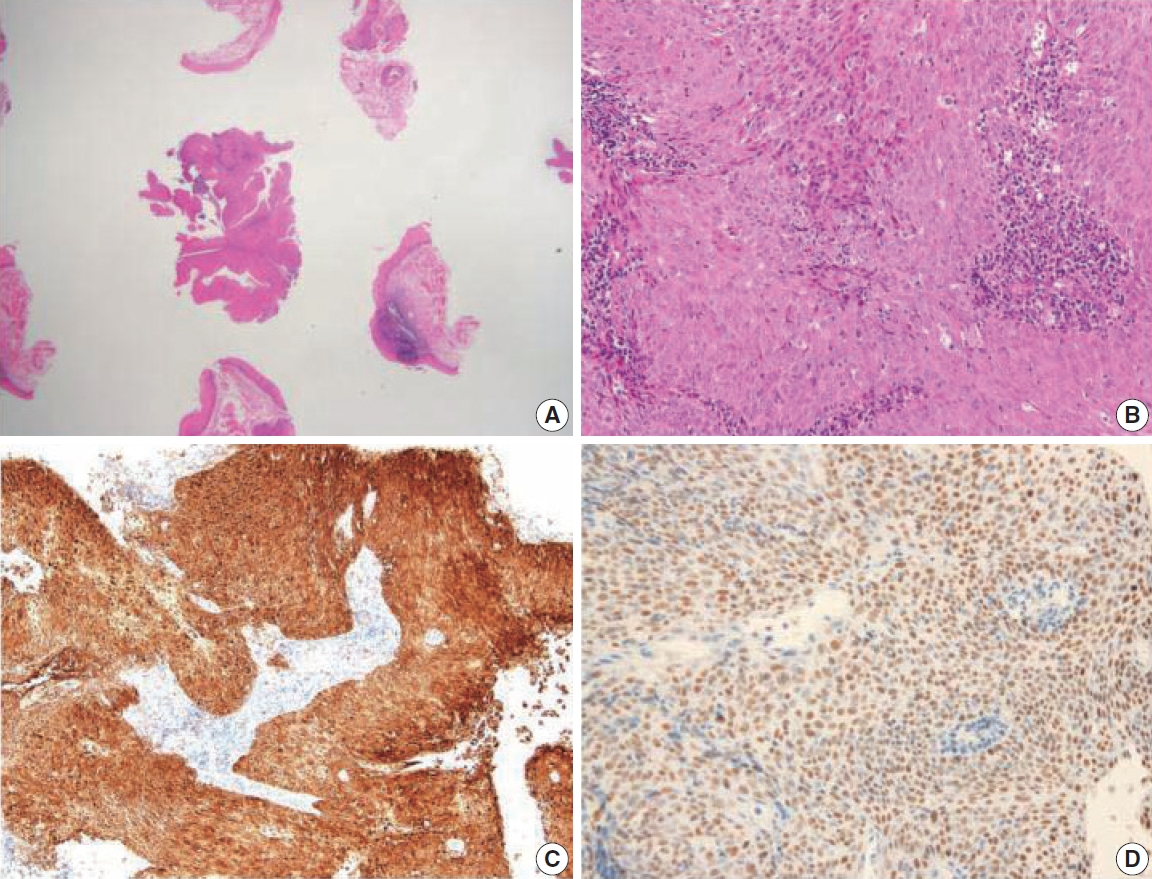
- A 55-year-old male patient was admitted for right neck swelling for 1 month. Neck computed tomography (CT) showed diffuse heterogeneous parenchymal density without focal nodular lesions in either thyroid gland and multiple lymph node enlargements in the right neck at levels II–V, the supraclavicular area, and the posterior neck, which suggested a primary thyroid tumor with nodal metastasis. Thyroid function test results were normal. Total thyroidectomy with radical neck node dissection was performed. Grossly, the thyroid gland was diffusely enlarged and had a white-gray solid appearance with no discernible mass (Fig. 1). Histologically, the thyroid parenchyma revealed extensive endolymphatic tumor emboli in a background of chronic lymphocytic thyroiditis (Fig. 2A). The tumor was composed of solid nests of atypical cells (Fig. 2B). The tumor cells were block-positive for p16 (Fig. 2C), positive for p40 (Fig. 2D) and p63 but negative for thyroglobulin and thyroid transcription factors, confirming SCC. Positron emission tomography–CT (PET-CT) revealed symmetrical hypermetabolic activity in and around the right tonsillar region. Tonsillar biopsy revealed HPV-positive SCC (Fig. 3A, B), with tumor cells showing the same immunohistochemical results as those of the thyroid tumor (Fig. 3C, D). Postoperative followup PET-CT revealed no residual mass. Because of the advanced stage (stage IVC), nine cycles of palliative chemotherapy with docetaxel plus cisplatin were postoperatively administered. However, PET-CT showed new metastatic lymph nodes in the right cervical, left supraclavicular, and right upper paratracheal areas 1 year after operation. A second round of chemotherapy with nivolumab was administered. The patient remained alive but with disease at the latest follow-up (15 months).
CASE REPORT
- The overall rate of distant metastasis of head and neck tumors is approximately 12% [6]. Head and neck SCC commonly metastasizes primarily to the lung and also bone and liver [5]. Distant metastases of head and neck tumors generally present within 2 years of definitive treatment, usually in the context of poor locoregional control of the primary lesion [6].
- Tonsillar cancer may spread locally to the surrounding tissues of the oropharynx, including the base of the tongue, soft palate, and posterior wall of the throat [5,7]. Alternatively, they can access the lymphatic system, which usually involves cervical lymph nodes, because tonsils have a rich vascular supply, providing an easy path for metastases to reach the regional lymph nodes [4,5,7]. However, distant metastases are extremely uncommon [7]. The incidence of distant metastases varies extensively in the literature, ranging from 3%–30% [6,7]. The most common sites include the liver, lungs, bones, mediastinal sites, skin, and, rarely, bone marrow [7]. Tumor stage determines the likelihood of metastasis, with advanced stages associated with approximately 15%–20% chance of metastasis in tonsillar cancer. Early-stage cancers rarely have distant metastases; however, advanced-stage cancers can metastasize beyond the cervical lymph nodes and spread through the lymphatic or vascular channels [5].
- Intrathyroidal metastases are rare, ranging from 0.6%–2.2% [1]. The primary sites most commonly identified in autopsy series are the breast and lung. However, in clinical series, renal cell carcinoma is the most frequent source of metastasis, often presenting many years after the original diagnosis [1,3]. Patients with metastatic thyroid cancer usually present with symptoms similar to those of primary thyroid cancer, particularly palpable neck masses. Dysphagia or dysphonia may develop if the metastatic cancer is advanced [1,4]. The time interval between the original primary cancer diagnosis and metastasis to the thyroid gland varies from a few months to years [4]. Thyroid function is usually normal [1,4].
- Metastasis of head and neck SCC to the thyroid gland is rare. Intrathyroidal metastasis of tonsillar SCC is even more unusual [1]. To date, only six cases of intrathyroidal metastasis of tonsillar SCC have been documented [1-5]. All published cases involved a history of tonsillar SCC. Metastatic tumors were identified during the staging workup for tonsillar cancer in two patients [3]. In two patients, a whole-body PET scan performed as part of the screening process showed an enlarging nodule in the thyroid gland 18 months and 4 years after the diagnosis of tonsillar cancer, respectively [4,5]. One patient presented with a neck mass 3 years after diagnosis of the primary tumor [1], and another patient complained of dysphonia and dysphagia 6 months after initial diagnosis [2]. HPV status was described in only one case and was positive. Clinical characteristics are summarized in Table 1. In this case, the patient first presented with thyromegaly, which was clinically suggestive of a primary thyroid tumor. HPV-positive tonsillar SCC was unexpectedly identified during systemic workup.
- The oropharynx, especially the tonsils and base of the tongue, represents the most common anatomical site of SCC of unknown primary origin of the head and neck, with an incidence ranging from 74%–89% [8]. HPV-positive oropharyngeal SCCs may distantly metastasize in unexpected sites [9] and frequently metastasize early in the course of disease when the primary tumor is small [10]. It is not uncommon for a patient to present with a neck metastasis and a small occult primary tumor that is HPVrelated and located deep in the oropharyngeal tonsillar crypts [10]. Therefore, a thorough oropharyngeal examination is necessary if metastatic SCC of the thyroid gland is suspected, although this is a rare event.
DISCUSSION
Ethics Statement
The Institutional Review Board of Dankook University Hospital (2023-01-015) approved this case report and informed consent was waived.
Availability of Data and Material
All data generated or analyzed during this study are included in this published article and available from the corresponding author.
Code Availability
Not applicable.
Conflicts of Interest
The author declares that I have no potential conflicts of interest.
Funding Statement
No funding to declare.
| Case No. | Tonsillar cancer | Time interval | Clinical symptom | Thyroid gland | HPV | Treatment | Reference |
|---|---|---|---|---|---|---|---|
| 1 | T2N2b | 3 yr | Neck mass | Nodules | N/A | Chemotherapy | [1] |
| 2 | N/A | 6 mo | Dysphonia | Mass | N/A | Thyroidectomy | [2] |
| 3 | T1N2cM0 | N/A | Staging | N/A | N/A | N/A | [3] |
| 4 | T2N2bM0 | N/A | Staging | N/A | N/A | N/A | [3] |
| 5 | T3N0 | 18 mo | Screening | Nodule | N/A | N/A | [4] |
| 6 | T2N2M0 | 4 yr | Screening | Mass | Positive | N/A | [5] |
| Present case | T1N2cM1 | 0 mo | Neck mass | Thyromegaly | Positive | Chemotherapy |
- 1. Jankowska P, Teoh EM, Fisher C, Rhys Evans P, Nutting CM, Harrington KJ. Case report: isolated intrathyroid metastasis from undifferentiated and squamous carcinoma of the head and neck: the case for surgery and re-irradiation. Br J Radiol 2008; 81: e154-61. PubMed
- 2. Scanelli G, Aimoni C, Marchetti E, Geminiani M, Pastore A. Thyroid’s metastasis of tonsillar squamous cell carcinoma. Recenti Prog Med 2005; 96: 428-30. PubMed
- 3. Millare GG, Kwon M, Edeiken-Monroe BS, Debnam JM. (18)FPET/CT imaging of metastasis to the thyroid gland: Imaging findings and effect on patient management. J Solid Tumors 2017; 7: 7-13. ArticlePubMedPMCPDF
- 4. Gumaa D, Christakis I, Mihai R. Metastasis to the thyroid gland from a tonsil squamous cell carcinoma. AME Case Rep 2018; 2: 7.ArticlePubMedPMC
- 5. Aparici CM, Win AZ. Two cases of thyroid metastasis from head and neck squamous cell carcinoma detected by FDG-PET/CT. J Clin Imaging Sci 2014; 4: 62.PubMedPMC
- 6. LeRose CC, Ramirez CA. Atypical metastasis of p16-positive tonsillar squamous cell carcinoma to the pleura: a case report. J Oral Maxillofac Surg 2018; 76: 2577-81. ArticlePubMed
- 7. Khan S, Anichini G, Mian A, Kareem H, Syed N, O’Neill K. Tonsillar carcinoma spreading metastases to central nervous system: case report and literature review. J Neurol Surg Rep 2021; 82: e11-6. ArticlePubMedPMC
- 8. Di Maio P, Iocca O, De Virgilio A, et al. Role of palatine tonsillectomy in the diagnostic workup of head and neck squamous cell carcinoma of unknown primary origin: a systematic review and meta-analysis. Head Neck 2019; 41: 1112-21. ArticlePubMedPDF
- 9. Sacks R, Law JY, Zhu H, et al. Unique patterns of distant metastases in HPV-positive head and neck cancer. Oncology 2020; 98: 179-85. ArticlePubMedPDF
- 10. Chernock RD, Lewis JS. Approach to metastatic carcinoma of unknown primary in the head and neck: squamous cell carcinoma and beyond. Head Neck Pathol 2015; 9: 6-15. ArticlePubMedPMCPDF
REFERENCES
Figure & Data
References
Citations
- Metastasis to Thyroid from Recurrent Head and Neck Squamous Cell Carcinoma: A Case Series and Review of Literature
Avneet Kaur, Rohit Nayyar, Harit Kumar Chaturvedi, Akshat Malik
Indian Journal of Surgical Oncology.2025; 16(1): 122. CrossRef - Metastatic oropharyngeal squamous cell carcinoma to the thyroid: A case report and review of literature
Hannah Walker, Jed Speers, Milena Fabry, Sameep Kadakia
American Journal of Otolaryngology.2024; 45(4): 104306. CrossRef
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-
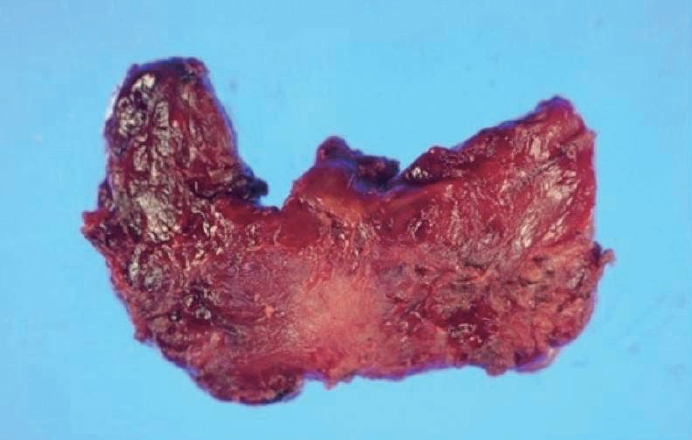
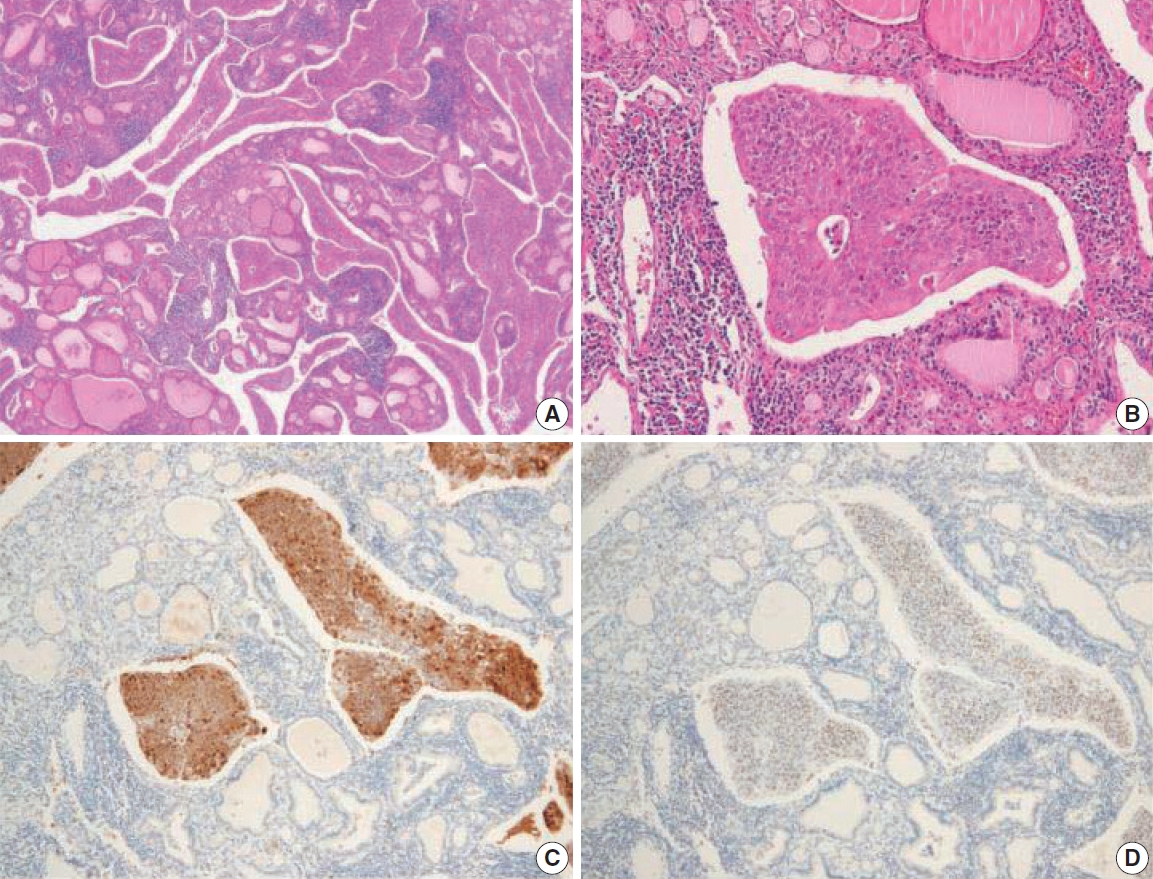
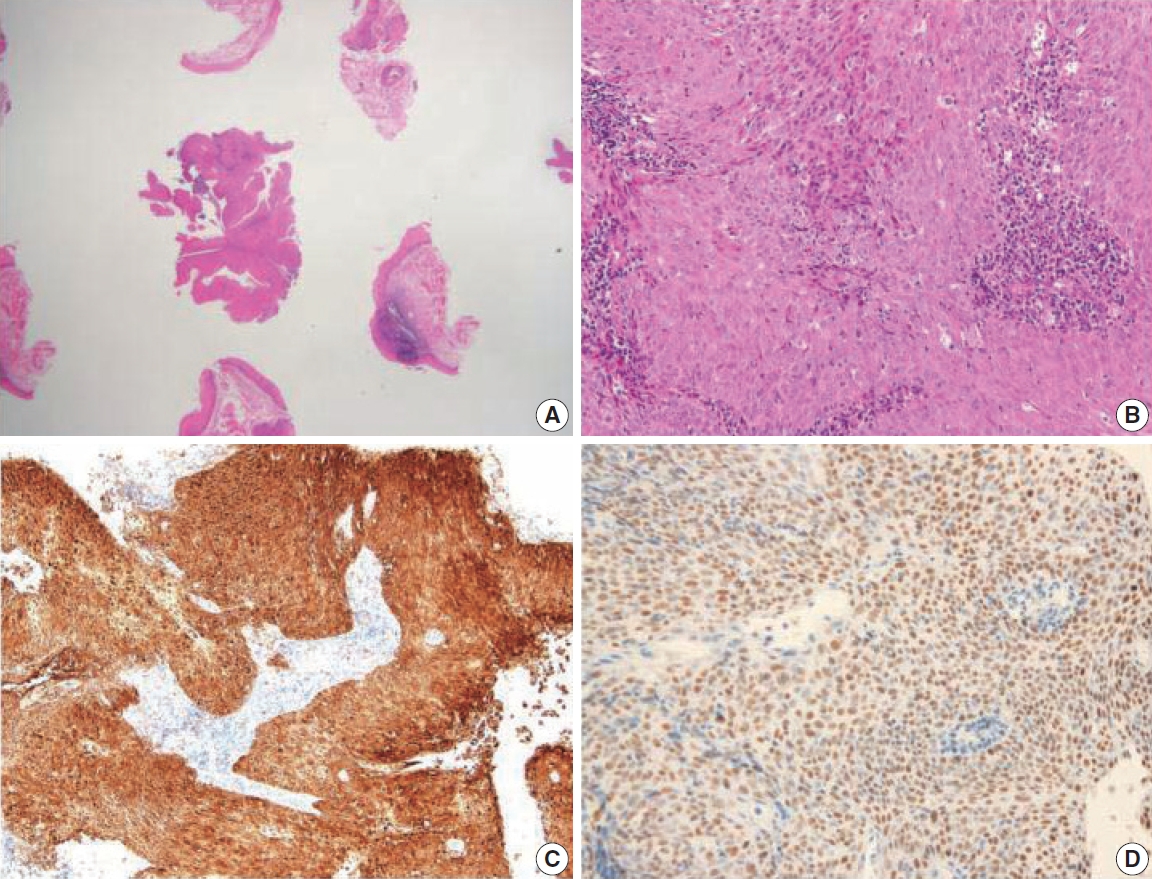



Fig. 1.
Fig. 2.
Fig. 3.
| Case No. | Tonsillar cancer | Time interval | Clinical symptom | Thyroid gland | HPV | Treatment | Reference |
|---|---|---|---|---|---|---|---|
| 1 | T2N2b | 3 yr | Neck mass | Nodules | N/A | Chemotherapy | [1] |
| 2 | N/A | 6 mo | Dysphonia | Mass | N/A | Thyroidectomy | [2] |
| 3 | T1N2cM0 | N/A | Staging | N/A | N/A | N/A | [3] |
| 4 | T2N2bM0 | N/A | Staging | N/A | N/A | N/A | [3] |
| 5 | T3N0 | 18 mo | Screening | Nodule | N/A | N/A | [4] |
| 6 | T2N2M0 | 4 yr | Screening | Mass | Positive | N/A | [5] |
| Present case | T1N2cM1 | 0 mo | Neck mass | Thyromegaly | Positive | Chemotherapy |
HPV, human papilloma virus; N/A, not available.

