E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 60(4); 2026 > Article
-
Case Study
Non-keratinizing immature squamous metaplasia in the pancreas mimicking malignancy: a diagnostic pitfall in cytology -
Hiroko Hayashi
 , Tomoaki Kubo, Takuya Hara, Saeko Jinnai, Keisuke Iwasaki
, Tomoaki Kubo, Takuya Hara, Saeko Jinnai, Keisuke Iwasaki -
Journal of Pathology and Translational Medicine 2026;60(4):444-450.
DOI: https://doi.org/10.4132/jptm.2026.02.19
Published online: July 15, 2026
Department of Pathology, Sasebo City General Hospital, Nagasaki, Japan
- Correspondence: Hiroko Hayashi, MD, PhD Department of Pathology, Sasebo City General Hospital, 9-3 Hirase-cho, Sasebo, Nagasaki 857-8511, Japan Tel: +81-956-24-1515, Fax: +81-956-23-6269, E-mail: hayashih@hospital.sasebo.nagasaki.jp
*This case was presented at the 22nd Korea-Japan Joint Meeting for Diagnostic Cytopathology, held in Yeosu, South Korea, on Saturday, September 27, 2025.
© The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 43 Views
- 1 Download
Abstract
- This report describes a challenging case in which atypical immature squamous metaplasia was misinterpreted as malignancy. A 69-year-old man presented with abdominal pain and loss of appetite. Imaging revealed mild pancreatic duct dilation, parenchymal enlargement, and increased fat attenuation in the transverse mesocolon. Endoscopic ultrasound revealed a hypoechoic lesion in the pancreatic body. The serum amylase level was markedly elevated (1,785 U/L), consistent with acute pancreatitis. Repeated pancreatic juice cytology examinations demonstrated atypical epithelial clusters, which raised concerns about possible pancreatic ductal adenocarcinoma. Therefore, distal pancreatectomy with splenectomy and transverse colon resection were performed. However, histopathological examination revealed only atypical immature squamous metaplasia. Retrospective review of the cytological specimens showed overlapping cell clusters with coarse chromatin, prominent nucleoli, nuclear pleomorphism, and peripheral dissociation in a neutrophilic background with focal hemorrhagic necrosis. Although rarely encountered, squamous metaplastic cells can appear in pancreatic cytology and represent a potential pitfall by mimicking adenocarcinoma.
- The reported frequency of squamous metaplasia in the pancreas varies widely in the literature [1,2]. According to the Armed Forces Institute of Pathology, squamous metaplasia is found in up to 45% of pancreata [3]. It typically arises in the intercalated ducts and is characterized by relatively immature squamous epithelial cells occupying the pancreatic ducts [3]. Notably, non-keratinizing squamous metaplasia is observed more frequently and has been referred to as “multilayered metaplasia” [3], “immature squamous metaplasia” [2], or “transitional metaplasia” [4].
- There have been reports of morphologically identifiable keratinizing squamous metaplasia in the field of cytology [1,5,6]. However, to the best of our knowledge, non-keratinizing immature squamous metaplasia in the pancreas has not been discussed, likely because cytology may not identify immature squamous metaplastic cells that are non-keratinized and lack characteristic features. We have encountered a case in which cytology initially led to a diagnosis of malignancy, but subsequent examination of the resected pancreatic specimen revealed only atypical immature squamous metaplasia. This report presents our findings in this extremely rare case in which immature squamous metaplastic cells were identified by cytology.
INTRODUCTION
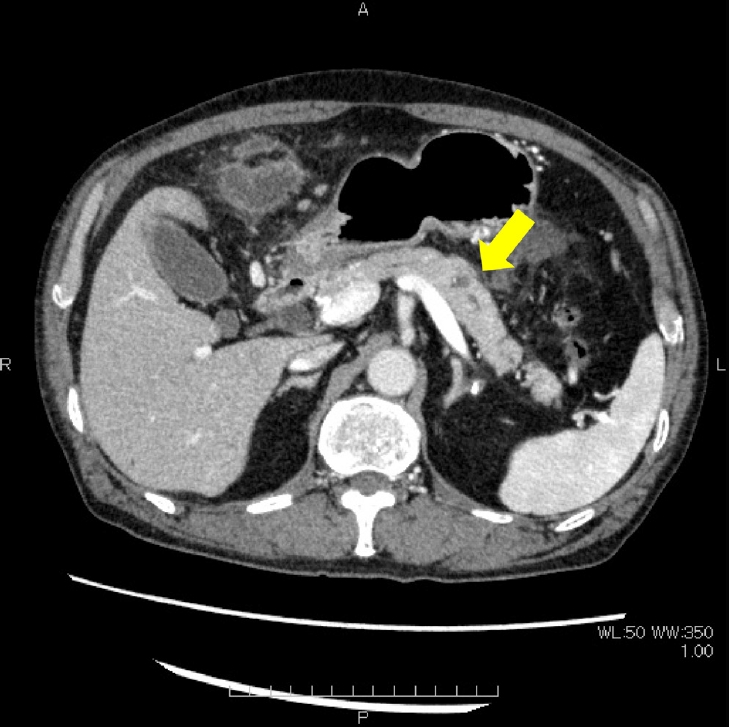
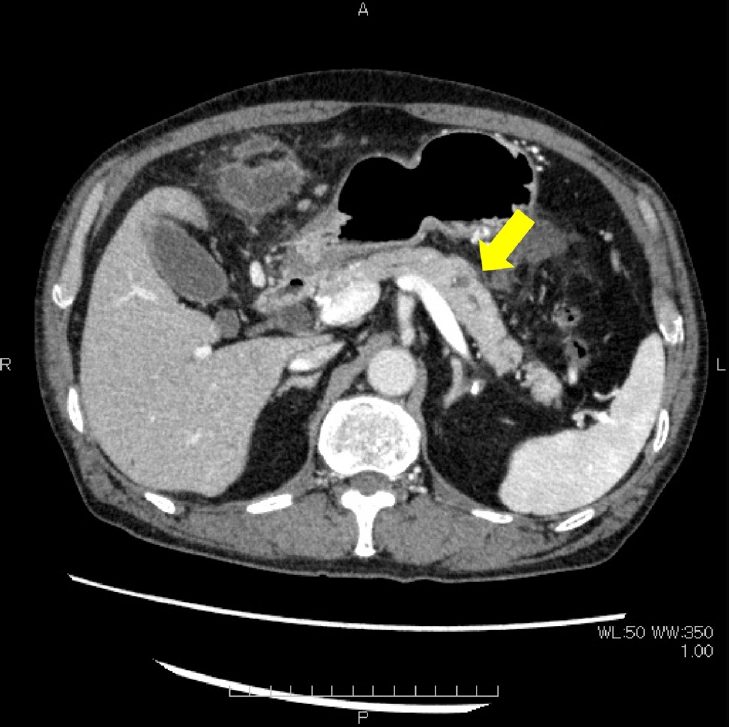
- A 69-year-old man visited our hospital with complaints of abdominal pain and loss of appetite. He had no significant medical history. However, he had a history of consuming 180 mL of Japanese sake per day. Abdominal computed tomography revealed mild dilation of the main pancreatic duct at the pancreatic tail and mild enlargement of the pancreatic parenchyma in the same region (Fig. 1). Furthermore, increased density was observed in the mesenteric adipose tissue in the area of the transverse colon. These findings suggested pancreatitis and fat necrosis of the mesenteric adipose tissue supporting the transverse colon. A 16-mm hypoechoic lesion with irregular margins was observed in the pancreatic body on endoscopic ultrasound; fine-needle aspiration was not performed because of the pancreatitis. Pancreatic enzyme assays showed marked elevations of serum and pancreatic amylase, reaching peak levels of 1,785 U/L, which supported the diagnosis of pancreatitis. Serum tumor markers, including S-pancreas antigen-1 (SPAN-1), Duke pancreatic antigen-2 (DUPAN-2), carbohydrate antigen 19-9 (CA19-9), and carcinoembryonic antigen, were all within normal ranges. Endoscopic pancreatic duct drainage and stenting was performed, followed by repeated pancreatic juice cytology examinations, which were submitted 15 times over an 11-day period. Atypical cells were detected in the final six specimens and were interpreted as atypical cells once, suspicious for malignancy three times, and positive for malignancy once. Although imaging findings were not definitive for malignancy, repeated pancreatic juice cytology demonstrated atypical epithelial clusters with features concerning for adenocarcinoma, leading to surgical intervention. Distal pancreatectomy combined with splenectomy, resection of the transverse colon, and cholecystectomy were performed. The postoperative course was uneventful. Given the possibility of occult microcarcinoma, the patient was followed according to a surveillance protocol similar to that for pancreatic malignancy. Computed tomography and serum tumor marker assessments were performed every 6 months. Although the serum carcinoembryonic antigen level fluctuated between 5 ng/mL and 8 ng/mL, no other clinical, radiological, or laboratory evidence of malignancy was identified during 5 years of follow-up, and surveillance was subsequently discontinued.
- Cytological findings
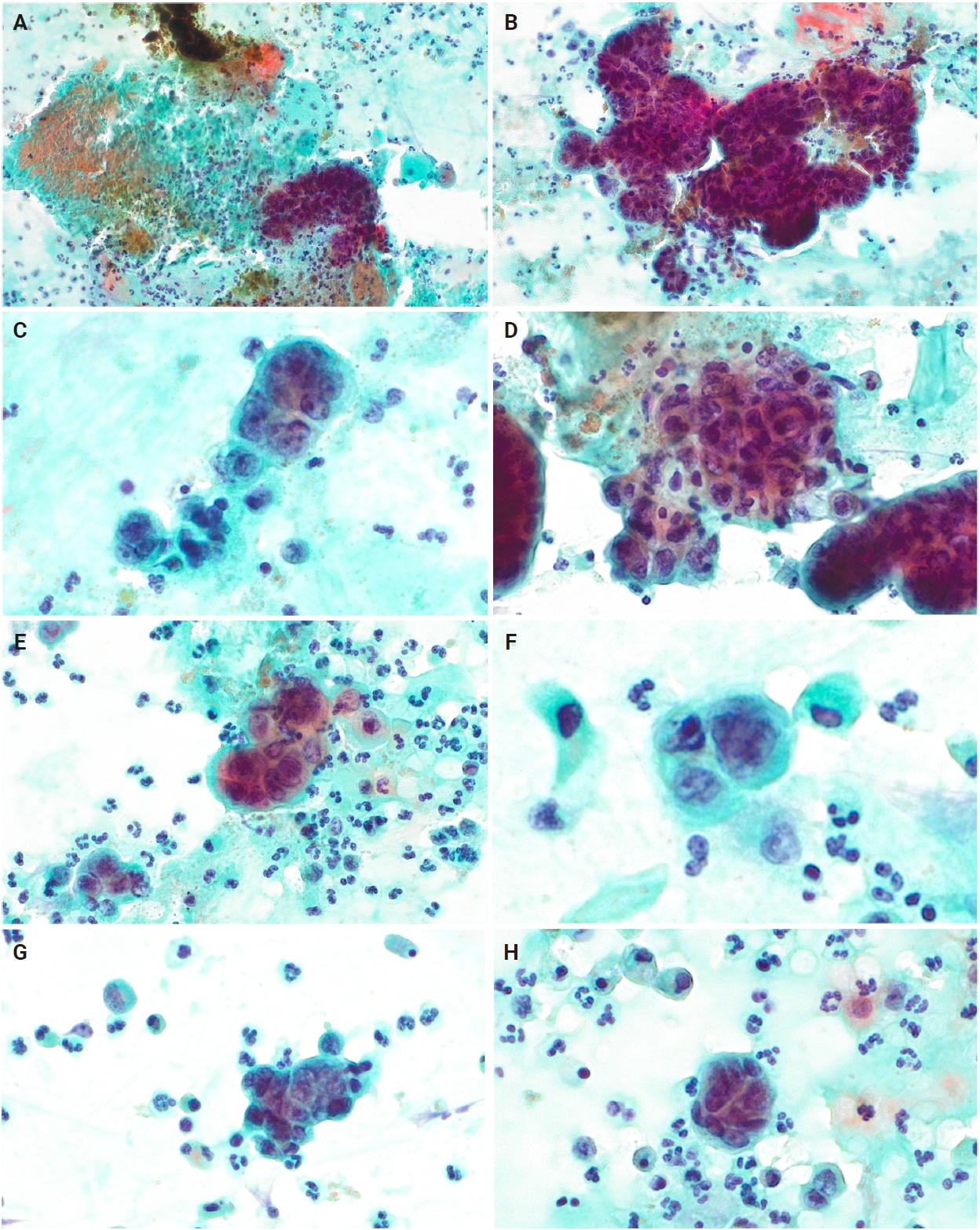
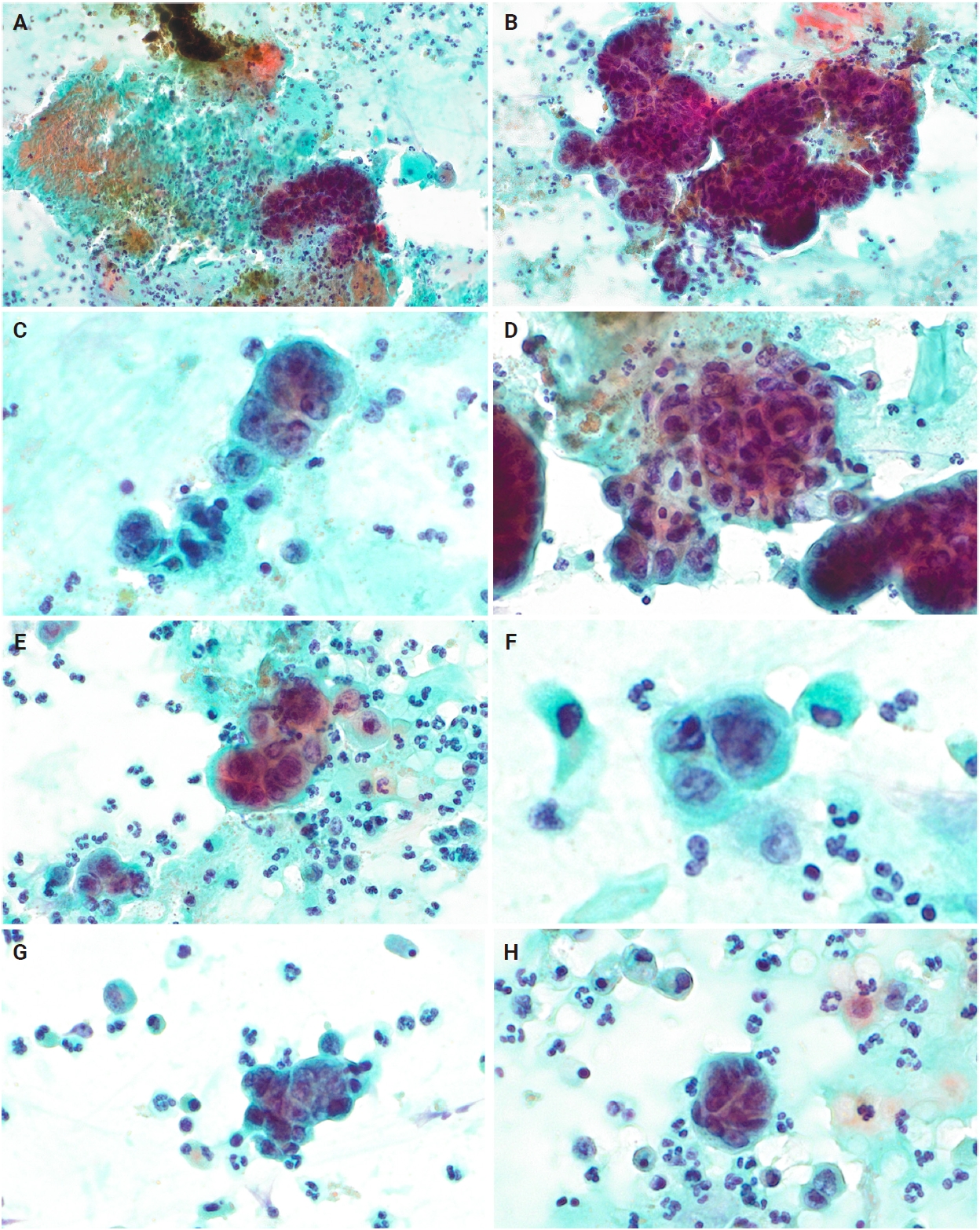
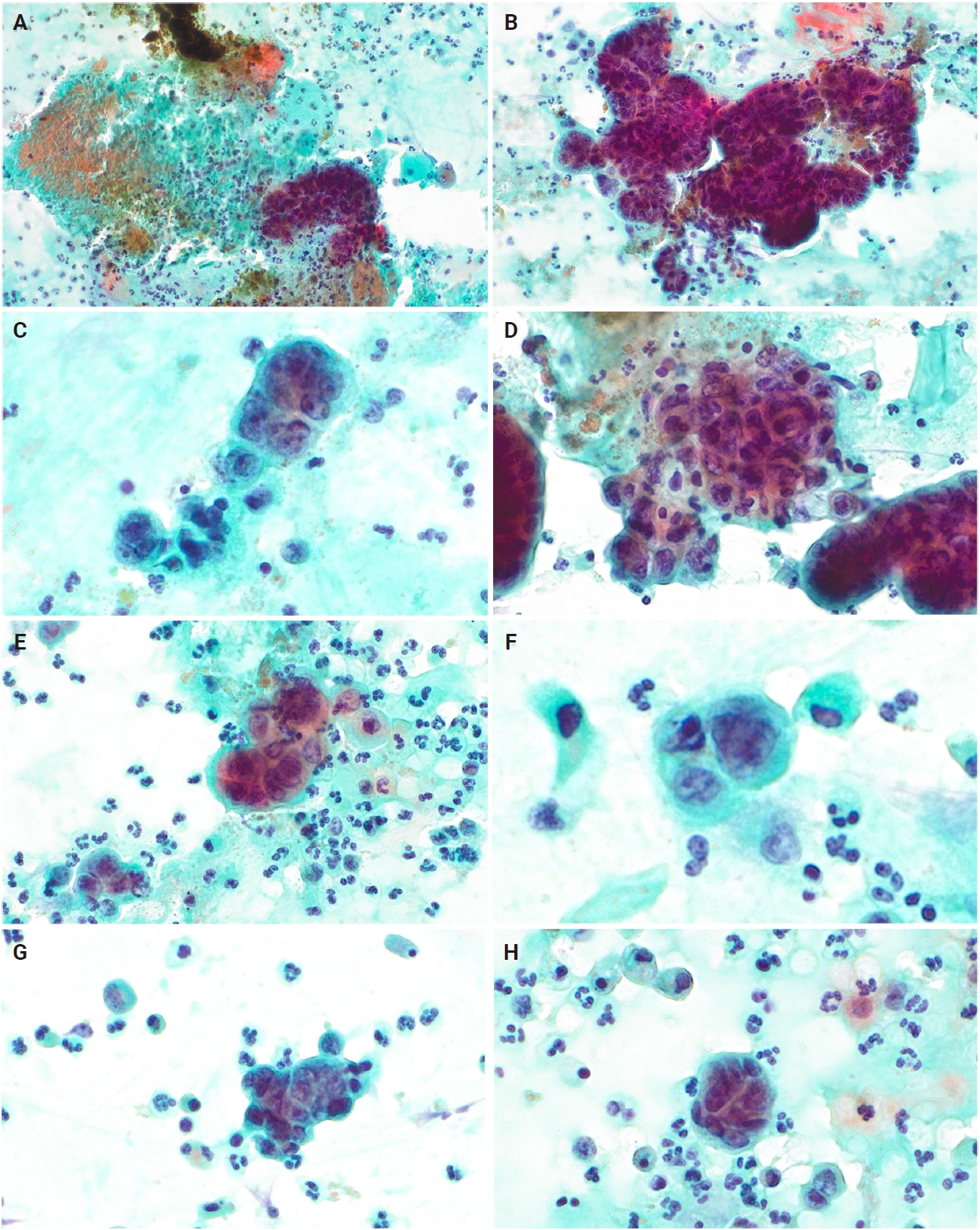
- Alcohol-fixed slides were stained by the Papanicolaou method in the cytology laboratory. Numerous cell clusters with overlapping arrangements were observed against a background of diffuse neutrophilic infiltration (Fig. 2A, B). Focal hemorrhagic necrosis was present (Fig. 2A). The cell clusters contained large cells with coarse nuclear chromatin, and nucleoli were prominent and enlarged (Fig. 2C). Nuclear pleomorphism was evident, with irregular nuclear arrangement and cell dissociation observed at the periphery of the clusters (Fig. 2D–H). Taken together, these cytological features of architectural complexity, nuclear atypia, and a necrotic inflammatory background supported a diagnosis of pancreatic ductal adenocarcinoma.
- Histopathological findings
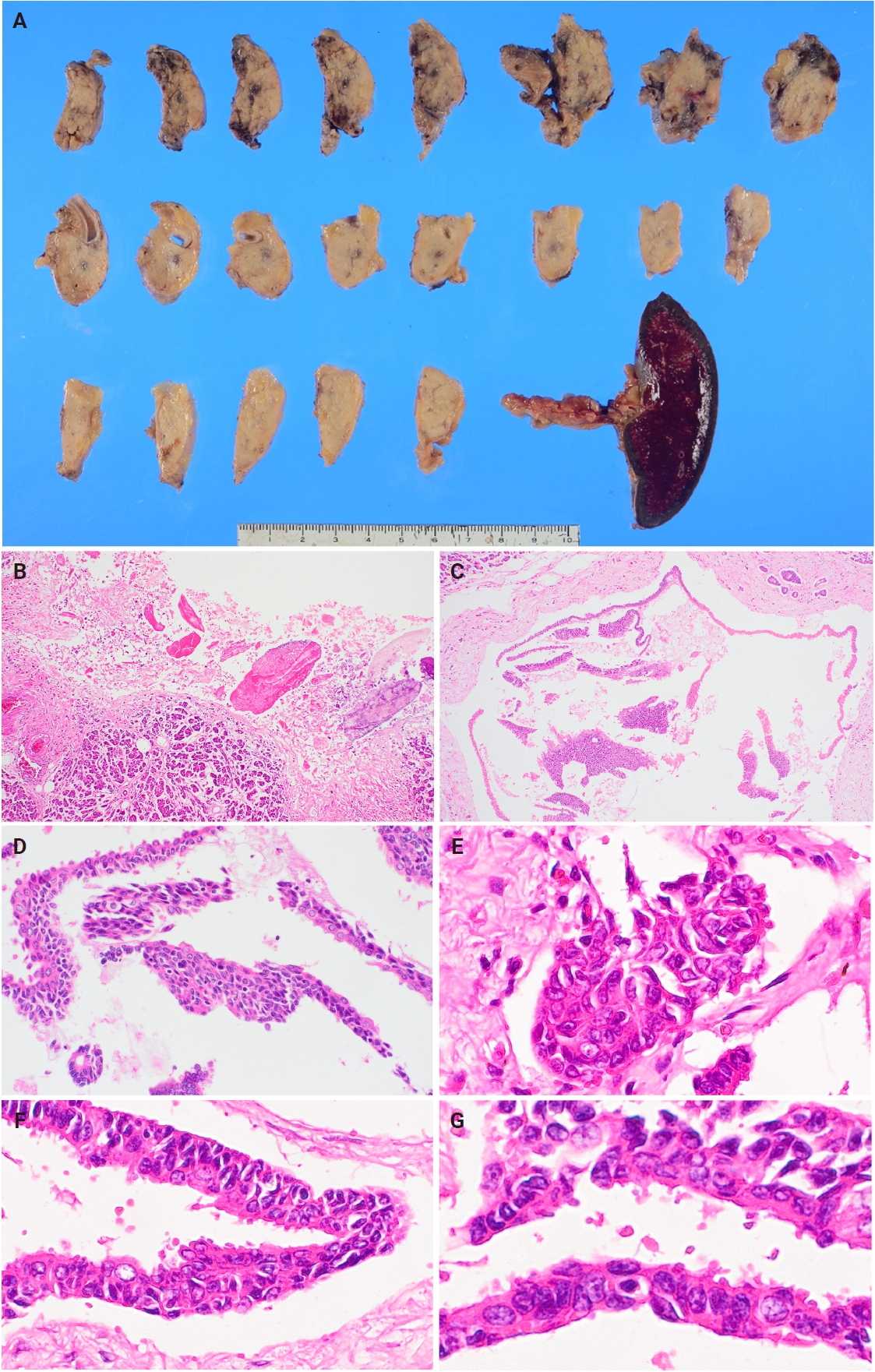
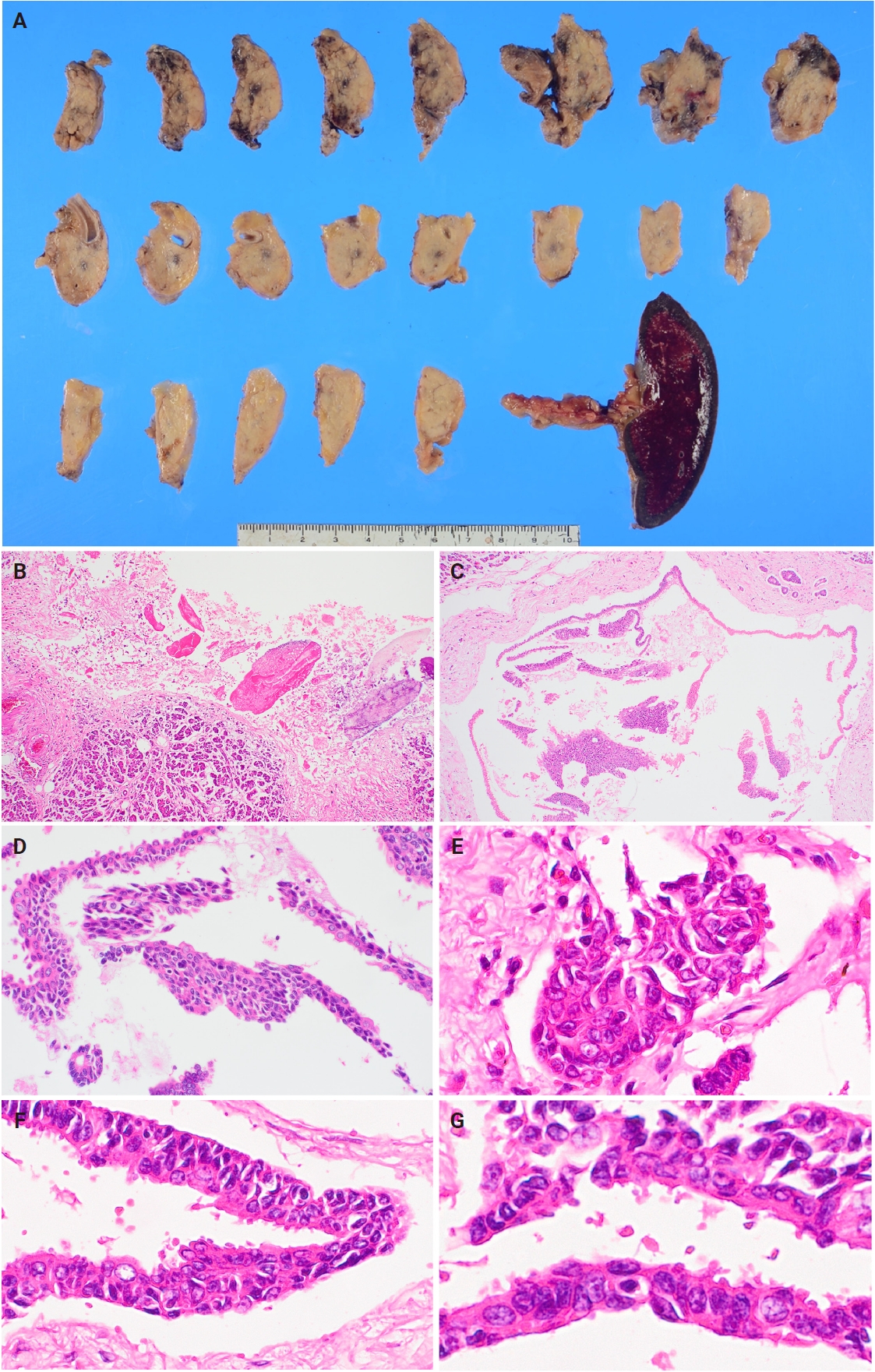
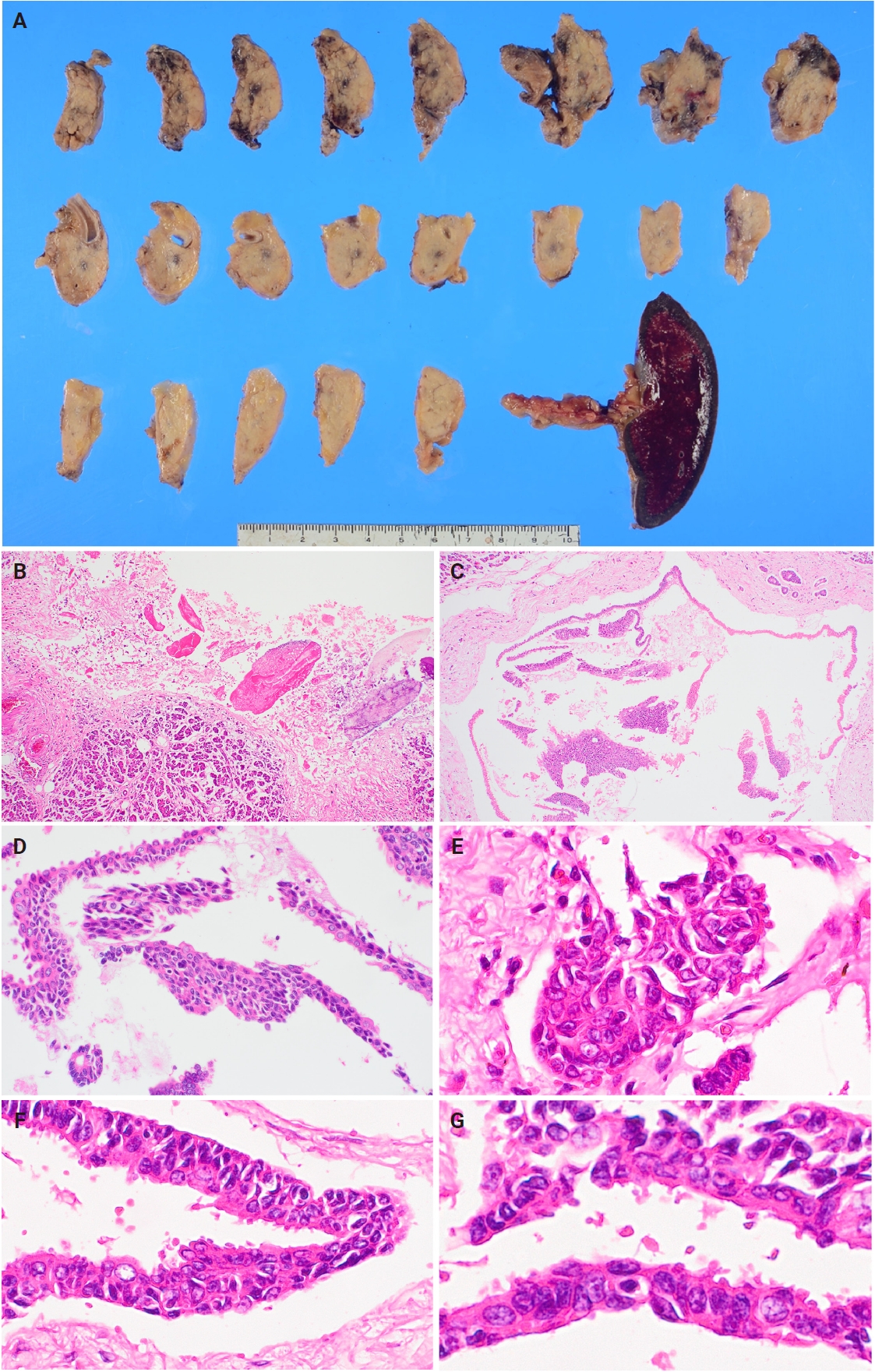
- Macroscopically, a portion of the cut surface of the pancreas showed necrosis as a result of pancreatitis. However, no distinct mass was identified (Fig. 3A). Histologically, mild fibrosis and dilated peripheral pancreatic ducts were observed, consistent with chronic pancreatitis. Focal necrosis of the surrounding adipose tissue and pancreatic parenchyma was also present, indicating superimposed acute pancreatitis (Fig. 3B). Furthermore, the concurrently resected transverse colon showed extensive mesenteric necrosis, consistent with the preoperative computed tomography findings and supportive of marked acute pancreatitis. The epithelium of the main pancreatic duct was extensively denuded, and squamous metaplasia was widely observed in both the main pancreatic duct and its branches (Fig. 3C, D). The squamous metaplastic cells varied in nuclear size, nuclear pleomorphism, and architectural disarray, closely resembling the atypical cells identified on cytological examination (Fig. 3E–G). Apart from the atypical immature squamous metaplasia, only a focal low-grade PanIN (pancreatic intraepithelial neoplasia)-equivalent mucinous epithelial metaplasia was observed in a single branch.
CASE REPORT
- The key diagnostic cytopathological features of pancreatic ductal adenocarcinoma include a necrotic background, loosely cohesive cell clusters, uneven nuclear spacing, loss of polarity (i.e., “drunken honeycomb”), hyperchromatic nuclei, and nuclear irregularity [7,8]. In the present case, the cytological specimens showed a necrotic and hemorrhagic background with clusters of varying sizes composed of large cells showing marked nuclear pleomorphism, irregular nuclear contours, coarse chromatin, and prominent nucleoli. Partial loss of cellular cohesion with cytologic features closely overlapped with those characteristic of pancreatic ductal adenocarcinoma led to an initial interpretation of malignancy. However, the hemorrhagic necrosis observed in the background was likely attributable to acute pancreatitis, based on clinical findings and the marked presence of neutrophils.
- False-positive cytology results in patients with chronic pancreatitis have been reported previously [9-11]. Chronic pancreatitis causes reactive nuclear enlargement and pleomorphism of pancreatic ductal epithelium because of inflammation, which presents cytologically with features that can be mistaken for adenocarcinoma [11,12]. However, false positives caused by squamous metaplasia have not been discussed until now. In the present case, although findings suggestive of chronic pancreatitis were observed, they were limited to mild fibrosis, and the main pathology was acute pancreatitis.
- Bixler et al. [1] described atypical squamous metaplasia as being characterized by mild to moderate nuclear hyperchromasia, nuclear enlargement up to four to five times the size of normal nuclei with pleomorphism, and nuclear irregularity with a relatively preserved nuclear-to-cytoplasmic ratio. Layfield et al. [6] reported that even when atypical squamous metaplastic cells are present, they can be distinguished from adenosquamous carcinoma or squamous cell carcinoma based on the number of atypical cells and the degree of nuclear atypia. Specifically, unlike squamous cell carcinoma or adenosquamous carcinoma, atypical squamous metaplastic cells tend to form cohesive clusters and lack necrotic debris in the background. However, in the present case, the atypical squamous metaplastic cells lacked overt keratinization and had scant cytoplasm with a high nuclear-to-cytoplasmic ratio, closely mimicking atypical glandular cells and leading to misinterpretation as adenocarcinoma.
- Histologically, immature squamous metaplastic cells in the pancreas are readily identifiable in resected specimens, allowing easy differentiation from malignancy, but can sometimes show atypia, necessitating differentiation from high-grade pancreatic intraepithelial neoplasia and other premalignant lesions [2,4]. In our case, atypical squamous metaplasia was identified histologically. The squamous metaplastic epithelial cells showed a tendency to detach from the ductal lining in both the main pancreatic duct and its branches. The morphology of these exfoliated cells closely resembled the atypical epithelial clusters observed in the cytological specimens, allowing retrospective recognition that the cytologically atypical cells corresponded to squamous metaplastic cells. On high-power examination, these cells were relatively large with architectural disarray, irregular nuclear contours, and coarse chromatin. Although these features represented marked cytological atypia at high magnification, low-power examination revealed unequivocal squamous metaplasia, and malignancy was not suspected histologically. These cells were considered to represent reactively enlarged squamous metaplastic cells with cytological atypia; however, when fragmented and exfoliated in pancreatic juice, they can closely mimic adenocarcinoma cells, as in the present case. This represents a significant diagnostic pitfall that has not been previously reported and should be carefully noted.
- A retrospective review of the cytological findings in this case revealed several features that could have helped avoid this diagnostic error. Although it remains uncertain whether atypical squamous metaplasia could be reasonably suspected when a similar case is encountered in routine practice, several observations from this case may nonetheless provide limited but important clues. Although the cell clusters showed some degree of peripheral dissociation, they were generally cohesive. Furthermore, despite the prominent nuclear pleomorphism and atypia, most nuclei were centrally positioned within the cells, and the cytoplasmic margins around them were discernible. Although subtle and easily overlooked, these findings, in retrospect, were more consistent with squamous metaplasia than with true malignancy.
- Pancreatic juice cytology has been performed in cases where the lesion is not clearly visible on imaging or is complicated by acute pancreatitis, with relatively high diagnostic sensitivity [13,14]. Repeated cell sampling via endoscopic pancreatic duct drainage and stenting allows for examination of more cells, improving the diagnostic accuracy. Sagami et al. [13] examined pancreatic juice cytology in 13 cases and reported that those with a greater number of positive results were more likely to represent true positives, whereas there were fewer positive findings in cases with false-positive results. In our case, pancreatic juice cytology was submitted 15 times over a period of 11 days. Three of the samples were diagnosed as suspicious for malignancy and one as positive for malignancy. Squamous metaplastic cells arise in the pancreatic ducts, so are likely to appear in pancreatic juice cytology. Therefore, the presence of atypical squamous metaplastic cells should be regarded as a cytological finding of particular concern in pancreatic juice specimens.
- In conclusion, squamous metaplasia can occur in patients with chronic and/or acute pancreatitis and even in those “without pancreatitis,” occasionally displaying atypia and leading to cytological findings that may mimic adenocarcinoma. Recognition of these cells as squamous metaplastic cells in cytology is extremely challenging because of the lack of keratinization. When cytological features raise suspicion for adenocarcinoma but are not definitive and no mass lesion is detected on imaging, the possibility of benign reactive atypical cells, such as atypical squamous metaplastic cells, should be carefully considered, especially in pancreatic juice cytology.
DISCUSSION
Ethics Statement
This case report is exempt from ethical review, in accordance with the ethical guidelines of the Japanese Society of Pathology and the institutional policy, as it involves a single case and contains no personally identifiable information. According to the ethical policy of the Japanese Society of Pathology and the policy of our institutional ethics committee, informed consent is not required for case reports if the patient’s identity cannot be determined. This report was prepared in compliance with these guidelines, and all identifying information has been removed or anonymized to protect the patient’s privacy.
Availability of Data and Material
All data generated or analyzed during the study are included in this published article (and its supplementary information files).
Code Availability
Not applicable.
Author Contributions
Conceptualization: HH, TK. Writing—original draft: HH. Writing—review & editing: all authors. Approval of final manuscript: all authors.
Conflicts of Interest
The authors declare that they have no potential conflicts of interest.
Funding Statement
No funding to declare.
Acknowledgments
We are grateful to Dr. Takuji Yamao (Department of Gastroenterology, Sasebo City General Hospital) and Dr. Yorihisa Sumida (Department of Gastroenterological Surgery, Sasebo City General Hospital) for their valuable clinical support and collaboration in patient management. We also thank Edanz (https://jp.edanz.com/ac) for editing a draft of this manuscript.
- 1. Bixler HA, Castro MJ, Stewart J 3rd. Cytologic differentiation of squamous elements in the pancreas. Diagn Cytopathol 2011; 39: 536-9. ArticlePubMed
- 2. Mochizuki K, Kondo T, Oishi N, et al. Immature squamous metaplasia (focal atypical epithelial hyperplasia) of the pancreatic duct: immunohistochemical distinction from intraductal carcinoma. Histopathology 2013; 63: 343-50. ArticlePubMed
- 3. Klimstra DS, Hruban RH, Sigel CS, Kloppel G. Atlases of tumor and non-tumor pathology, series 5: tumors of the pancreas. Arlington: American Registry of Pathology, 2023.
- 4. Basturk O, Khanani F, Sarkar F, Levi E, Cheng JD, Adsay NV. DeltaNp63 expression in pancreas and pancreatic neoplasia. Mod Pathol 2005; 18: 1193-8. ArticlePubMedPDF
- 5. VandenBussche CJ, Maleki Z. Fine-needle aspiration of squamous-lined cysts of the pancreas. Diagn Cytopathol 2014; 42: 592-9. ArticlePubMed
- 6. Layfield LJ, Cramer H, Madden J, Gopez EV, Liu K. Atypical squamous epithelium in cytologic specimens from the pancreas: cytological differential diagnosis and clinical implications. Diagn Cytopathol 2001; 25: 38-42. ArticlePubMed
- 7. WHO Classification of Tumours Editorial Board. WHO classification of tumours. 5th ed. Digestive system tumours. Lyon: International Agency for Research on Cancer (IARC), 2019.
- 8. Bergeron JP, Perry KD, Houser PM, Yang J. Endoscopic ultrasound-guided pancreatic fine-needle aspiration: potential pitfalls in one institution's experience of 1212 procedures. Cancer Cytopathol 2015; 123: 98-107. ArticlePubMed
- 9. Siddiqui AA, Kowalski TE, Shahid H, et al. False-positive EUS-guided FNA cytology for solid pancreatic lesions. Gastrointest Endosc 2011; 74: 535-40. ArticlePubMed
- 10. Xie C, Bohy K, Abdallah MA, et al. Finding a needle in a haystack: endoscopic ultrasound-guided fine-needle aspiration for solid pancreatic masses in the setting of chronic pancreatitis. Ann Gastroenterol 2020; 33: 418-25. ArticlePubMedPMC
- 11. Scarpa-Carniello JV, Siddiqui MT. Challenges and pitfalls in pancreatobiliary cytopathology. Acta Cytol 2024; 68: 219-26. ArticlePubMedPMCPDF
- 12. Bellizzi AM, Stelow EB. Pancreatic cytopathology: a practical approach and review. Arch Pathol Lab Med 2009; 133: 388-404. ArticlePubMedPDF
- 13. Sagami R, Mizukami K, Nishikiori H, et al. Pancreatic juice cytology for diagnosing invasive pancreatic carcinoma/high-grade pancreatic intraepithelial neoplasia without visible tumors on endoscopic ultrasound. Pancreatology 2024; 24: 740-6. ArticlePubMed
- 14. Mikata R, Ishihara T, Tada M, et al. Clinical usefulness of repeated pancreatic juice cytology via endoscopic naso-pancreatic drainage tube in patients with pancreatic cancer. J Gastroenterol 2013; 48: 866-73. ArticlePubMedPDF
REFERENCES
Figure & Data
References
Citations
 Cite this Article
Cite this Article