 E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 60(4); 2026 > Article
-
Original Article
Hyalinizing trabecular tumors with areas resembling noninvasive follicular thyroid neoplasm with papillary‑like nuclear features: an immunohistochemical and molecular analysis -
Risa Kanematsu1
 , Mitsuyoshi Hirokawa1, Ayana Suzuki1, Miyoko Higuchi1, Satomi Usuki2, Hiroshi Kamma2, Takashi Akamizu3
, Mitsuyoshi Hirokawa1, Ayana Suzuki1, Miyoko Higuchi1, Satomi Usuki2, Hiroshi Kamma2, Takashi Akamizu3 -
Journal of Pathology and Translational Medicine 2026;60(4):436-443.
DOI: https://doi.org/10.4132/jptm.2026.06.07
Published online: July 15, 2026
1Department of Diagnostic Pathology and Cytology, Kuma Hospital, Kobe, Japan
2Nasu Institute of Medical Sciences, Kamma Memorial Hospital, Nasushiobara, Japan
3Department of Internal Medicine, Kuma Hospital, Kobe, Japan
- Corresponding Author: Risa Kanematsu Department of Diagnostic Pathology and Cytology, Kuma Hospital, 8-2-35 Shimoyamate-dori, Chuo-Ku, Kobe, Hyogo 650-0011, Japan Tel: +81-78-371-3721, Fax: +81-78-371-3645, E-mail: kanematsu@kuma-h.or.jp
© The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 42 Views
- 1 Download
Abstract
-
Background
- The coexistence of hyalinizing trabecular tumor (HTT) and areas with a morphology of noninvasive follicular thyroid neoplasm with papillary‑like nuclear features (NIFTP) within a single thyroid nodule has not been previously reported. We aimed to determine whether such tumors represent two independent neoplasms or a single tumor exhibiting divergent morphology.
-
Methods
- Ten tumors containing both HTT and NIFTP-like areas were examined. The term “NIFTP-like” was used strictly as a descriptive morphological designation for areas that fulfill the histologic criteria of NIFTP. Immunohistochemical analyses of Ki‑67 (MIB‑1) and type IV collagen and targeted molecular testing were performed. Ten NIFTPs, 10 follicular adenomas, and three HTTs were used as controls.
-
Results
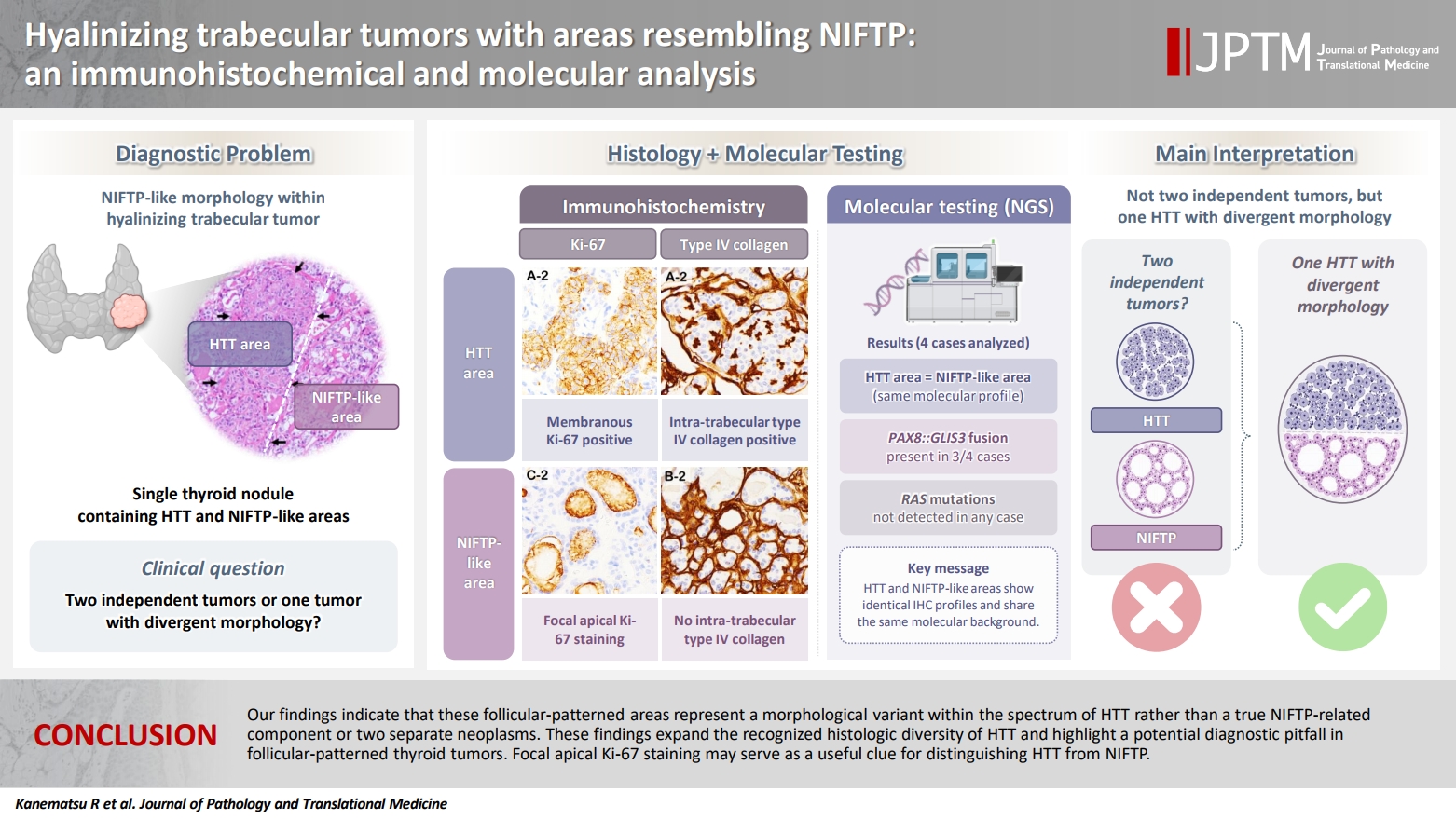
- HTT components consistently showed characteristic membranous Ki‑67 staining and intra‑trabecular type IV collagen deposition, whereas NIFTP‑like areas lacked these features, except for focal apical Ki‑67 staining. Intranuclear cytoplasmic inclusions in HTT were positive for type IV collagen. NIFTPs showed neither membranous Ki‑67 nor intra-trabecular type IV collagen. Molecular analysis demonstrated identical profiles between HTT components and NIFTP-like areas: three tumors harbored PAX8::GLIS3 fusions, and none showed RAS mutations. Pure HTT controls exhibited the same pattern.
-
Conclusions
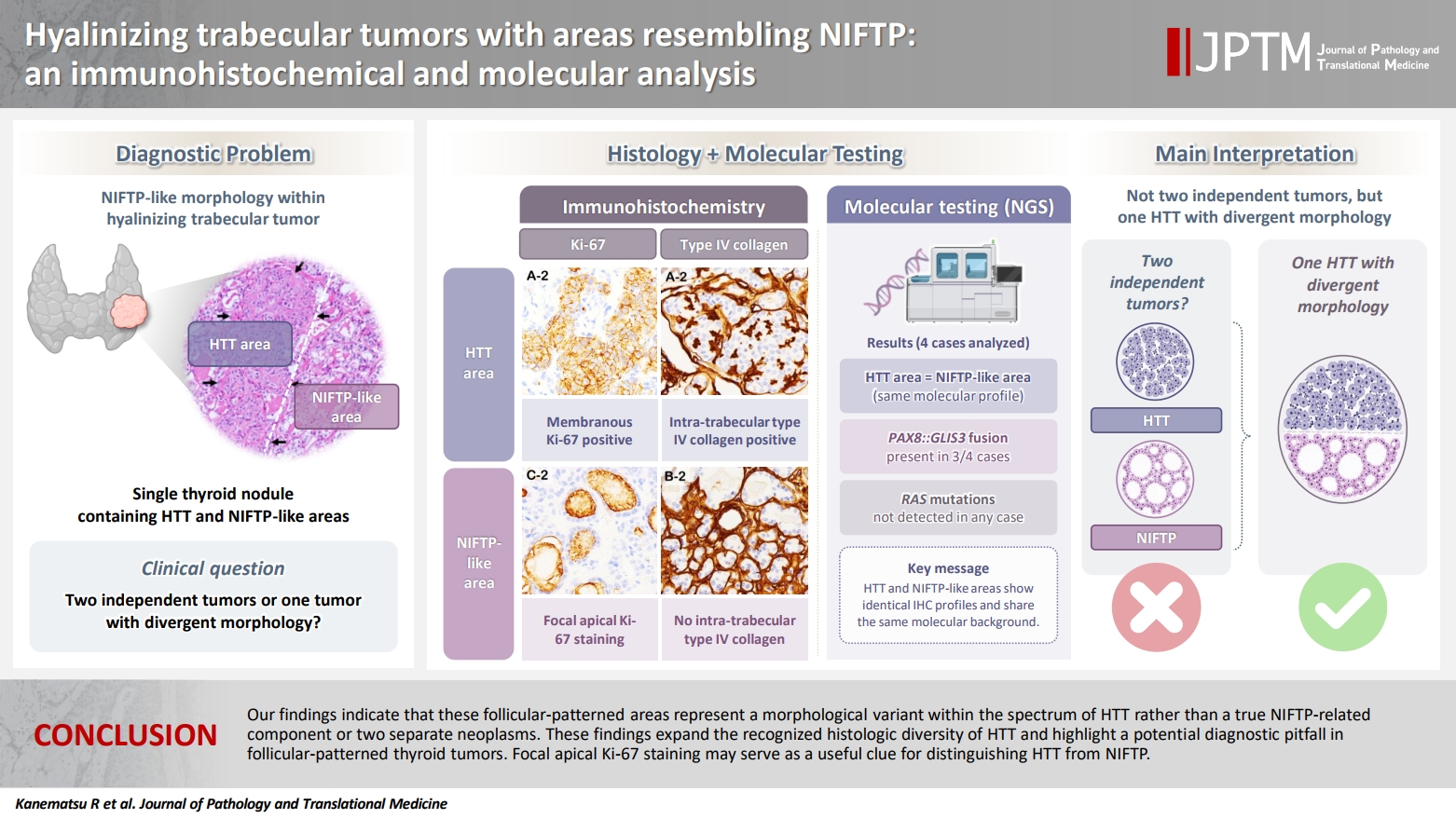
- Our findings indicate that these follicular-patterned areas represent a morphological variant within the spectrum of HTT rather than a true NIFTP-related component or two separate neoplasms. These findings expand the recognized histologic diversity of HTT and highlight a potential diagnostic pitfall in follicular‑patterned thyroid tumors. Focal apical Ki‑67 staining may serve as a useful clue for distinguishing HTT from NIFTP.
- Hyalinizing trabecular tumors (HTT) are uncommon thyroid neoplasms characterized by a trabecular growth pattern, prominent inter- and intra-trabecular hyaline material, and distinctive membranous immunoreactivity for MIB-1 (a Ki-67 clone) [1,2]. While inter‑trabecular hyaline material is usually evident on routine hematoxylin and eosin staining, intra‑trabecular hyalinization can be subtle in some cases. Type IV collagen immunostaining is useful in such situations as it highlights basement‑membrane–derived hyaline material and facilitates the recognition of HTT components [3]. HTT is currently classified as a low-risk thyroid tumor [1]. Cytologically, HTT tumor cells exhibit nuclear grooves, intranuclear cytoplasmic inclusions, and nuclear clearing, features that overlap with papillary thyroid carcinoma (PTC), making accurate diagnosis challenging. The recent identification of the PAX8::GLIS3 fusion as a highly specific molecular hallmark has substantially improved the distinction of HTT from other follicle-derived thyroid tumors [3-6]. Noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) is also categorized as a low-risk tumor and is defined by a follicular growth pattern and PTC-like nuclear features [1]. Previously classified as a noninvasive encapsulated follicular variant of PTC [7], NIFTP is typically associated with RAS-like mutations, which are not specific and may also be observed in other benign or low-grade neoplasms [8,9]. Thus, although HTT and NIFTP share overlapping nuclear morphology and similarly indolent biological behavior, their growth patterns and molecular pathogenesis are fundamentally different.
- During routine diagnostic practice, we identified a series of thyroid tumors demonstrating the coexistence of HTT and areas with NIFTP morphology within a single nodule. To our knowledge, such tumors have not been previously described. These lesions raise important questions regarding their histogenesis: they may represent a hybrid tumor composed of distinct HTT and NIFTP, or a single neoplasm exhibiting divergent differentiation. Therefore, the objective of this study was to determine whether the coexistence of HTT and areas with NIFTP morphology within a single nodule represents two independent neoplasms or a single tumor with divergent morphology. To address this question, we integrated detailed histological assessment with immunohistochemical and molecular analyses, with particular emphasis on detecting PAX8::GLIS3 fusion. Our goal was to clarify the histogenesis of these unusual tumors and to identify diagnostic features that may help to avoid misclassification in routine practice.
INTRODUCTION
- Case selection
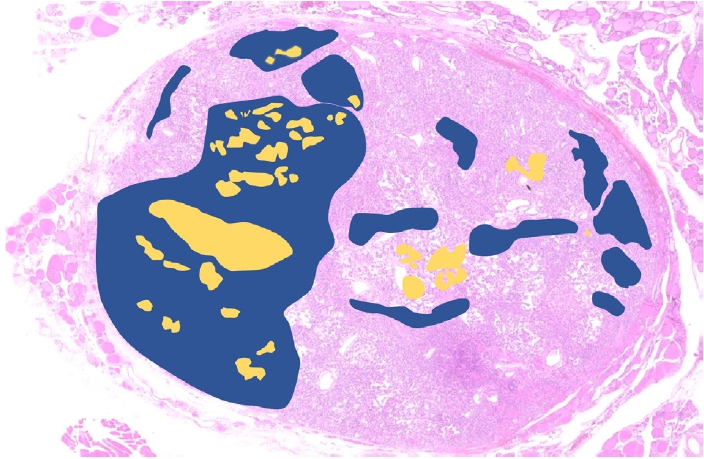
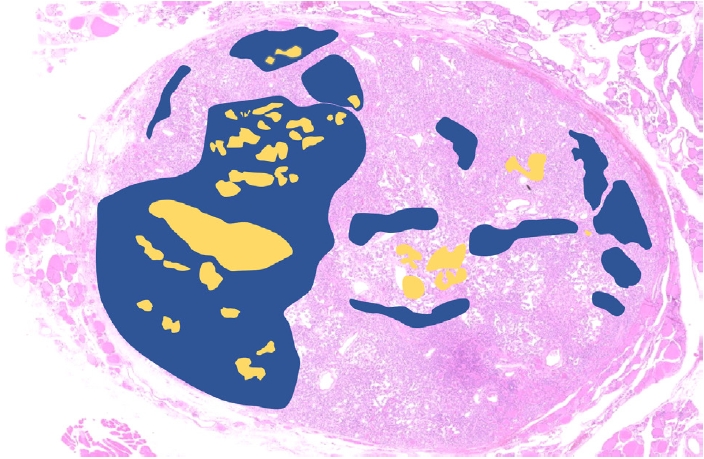
- We retrospectively reviewed data from 70 HTTs that were resected at our institution between 1983 and 2024. Among these, we identified 10 tumors demonstrating the coexistence of HTT components and NIFTP-like areas, defined as the presence of both components within the same nodule, with the NIFTP-like areas comprising at least 1% of the total tumor area (Fig. 1). The HTT components were defined as comprising intra-trabecular hyalinized material and having a trabecular growth pattern and PTC-type nuclear features, including nuclear grooves, pseudoinclusions, and membrane irregularities. The NIFTP-like area was defined as having a follicular growth pattern without intratrabecular hyalinized material, and showing the existence of PTC-like nuclear features (nuclear score of 2 or 3), an absence of tumor necrosis, and a low mitotic count (<3 mitosis/2 mm2). The term “NIFTP-like” was used strictly as a descriptive morphological designation for areas that fulfill the histologic criteria of NIFTP on hematoxylin and eosin (H&E) sections. This terminology does not imply true NIFTP; rather, it was applied because the follicular‑patterned morphology is not inconsistent with the histologic features of NIFTP. All histopathological evaluations and case selections were independently reviewed and confirmed by two board‑certified pathologists specializing in thyroid pathology (Mitsuyoshi Hirokawa and Hiroshi Kamma). Both pathologists examined the slides in a single‑blind manner with respect to the molecular results, and discrepancies were resolved by joint review and consensus. For immunohistochemical and molecular analyses, we selected as controls 10 classic and pure NIFTP, 10 follicular adenoma, and three HTT cases from among the most recent cases within the study period. Formalin-fixed paraffin-embedded (FFPE) tissue blocks from all selected cases were retrieved for histological, immunohistochemical, and molecular analyses.
- Immunohistochemistry
- Immunohistochemical staining was performed using antibodies against Ki‑67 (MIB‑1, 1:200, Dako Cytomation, Carpinteria, CA, USA) and type IV collagen (PHM-12, 1:100, Merck KGaA, Darmstadt, Germany). To evaluate characteristic membranous reactivity, Ki‑67 immunostaining was specifically selected for assessing the HTT component. Type IV collagen immunostaining was included to facilitate the identification of intra‑trabecular hyalinization, which can be difficult to recognize on routine hematoxylin and eosin staining. Staining was carried out on an automated Leica Bond‑Max system using the Bond Refine detection kit (Leica Microsystems, Bannockburn, IL, USA). For Ki-67 immunohistochemistry, antigen retrieval was performed manually using heat treatment (electric kettle 98°C, 40 minutes) [10].
- Molecular analysis
- As the study cohort spanned more than 40 years, many archival specimens were older than 5 years, which is considered unsuitable for reliable next-generation sequencing (NGS) analysis. In addition, separate macrodissection of the HTT components and NIFTP-like areas required each area to contain at least a 5‑mm square of viable tissue. Only four tumors met both criteria. These correspond to cases 7, 8, 9, and 10 in Table 1, and the same case numbers are used in Table 2 to indicate the tumors that underwent molecular testing. FFPE tissue fragments were separately microdissected from HTT components and NIFTP-like areas. DNA and RNA were extracted using the AllPrep DNA/RNA FFPE Kit (#80234, Qiagen, Hilden, Germany). Molecular analysis was performed using a targeted Japanese NGS panel (ThyroGene v3, Nasu Medical Institute of Medical Sciences, Tochigi, Japan), which detects the most common genetic alterations in thyroid tumors, including PAX8::GLIS1/3 fusions, BRAFV600E mutations, and RAS (KRAS, HRAS, and NRAS) mutations.
MATERIALS AND METHODS
- A total of 10 tumors containing both HTT components and NIFTP‑like areas were identified among 70 resected HTTs (14.3%). The clinical and pathological characteristics of these tumors are summarized in Table 1. Patients ranged from 28 to 75 years of age, and eight were women. Tumor sizes varied from 6 to 54 mm. All cases had been originally diagnosed as HTT. Encapsulation was absent or partial in all tumors. HTT components predominated in seven cases, whereas NIFTP‑like areas predominated in three cases. Nuclear scores were uniformly high (score 3 in both HTT components and NIFTP‑like areas).
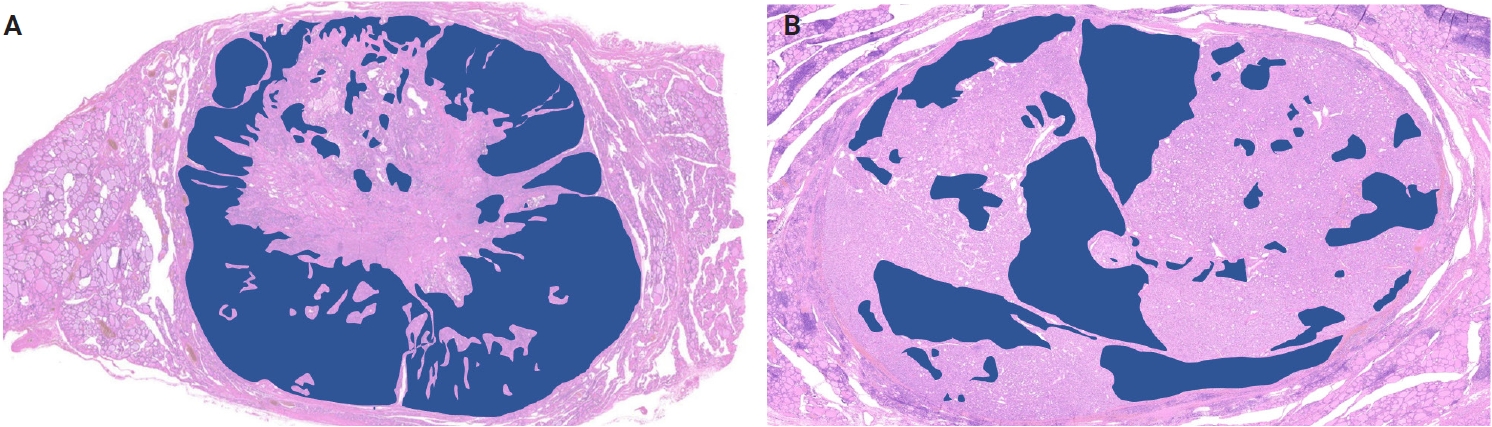
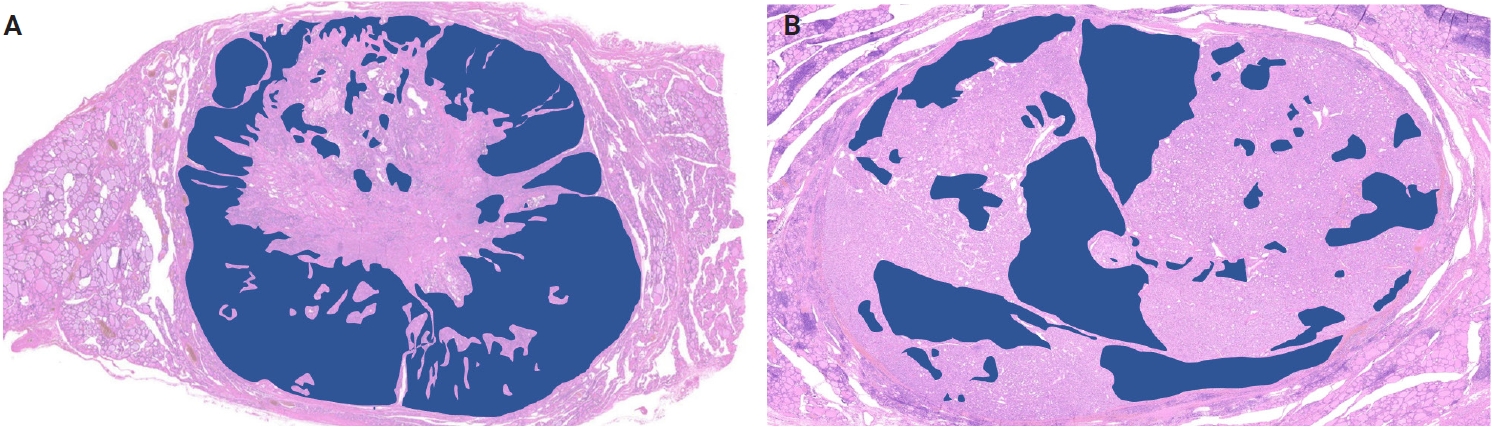
- HTT components were distributed in a geographic or island-like pattern in all cases, and their proportions varied considerably across tumors. In seven of the 10 cases, HTT components accounted for >50% of the tumor area (Fig. 2A), whereas in the remaining three cases, NIFTP-like areas predominated (>50%) (Fig. 2B). The two components were intimately intermingled, and their boundaries could not be clearly delineated.
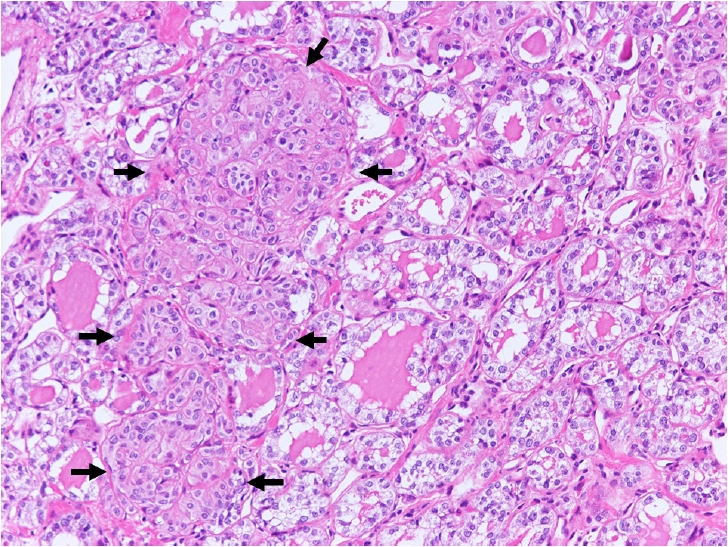
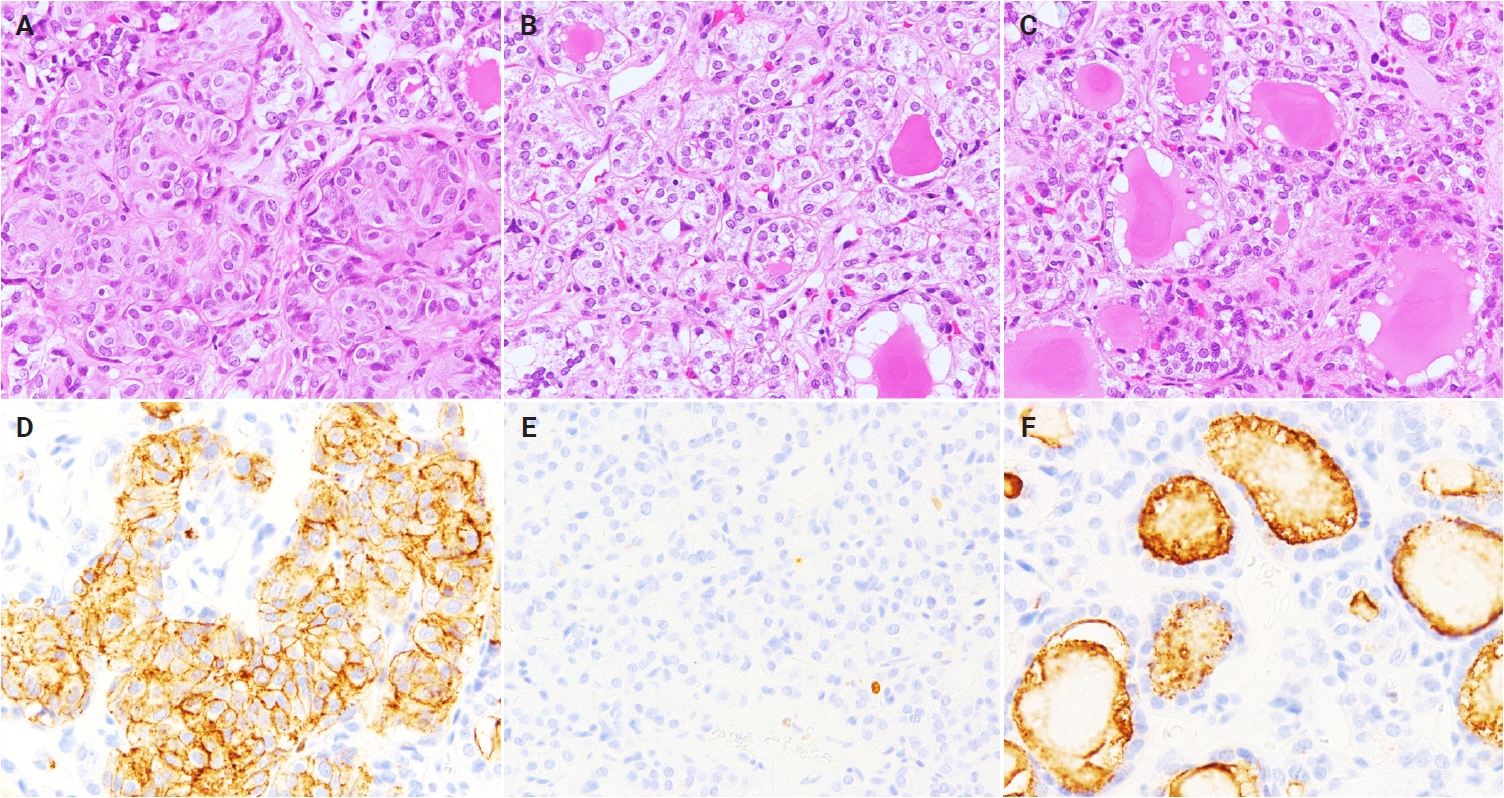
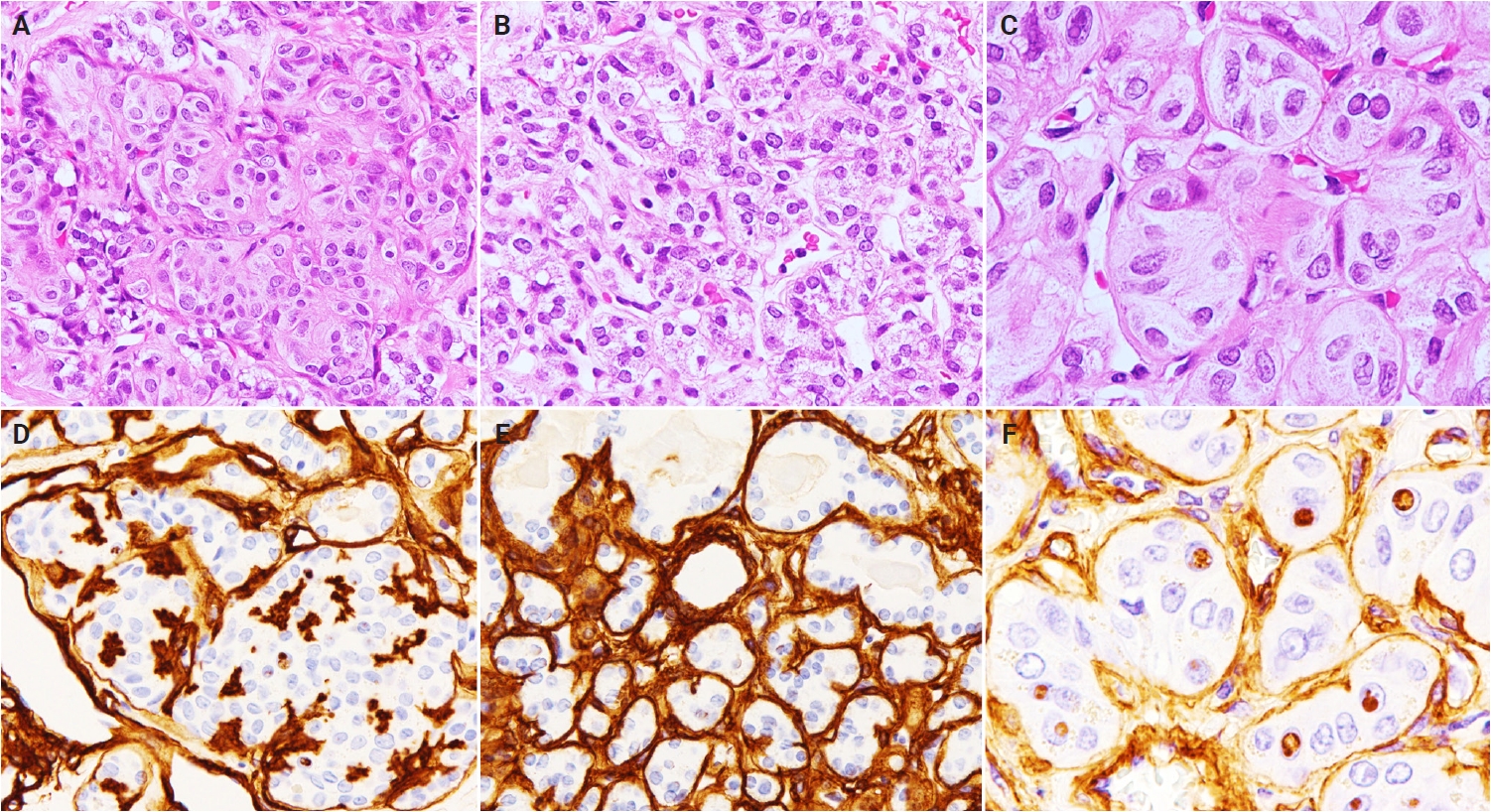
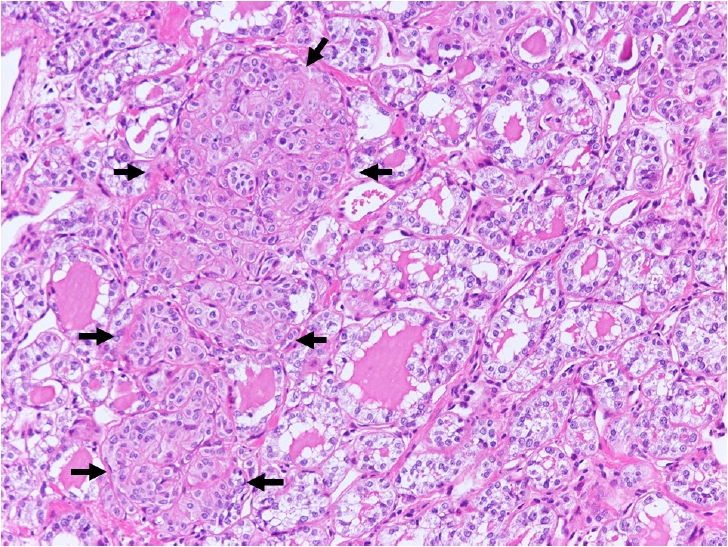
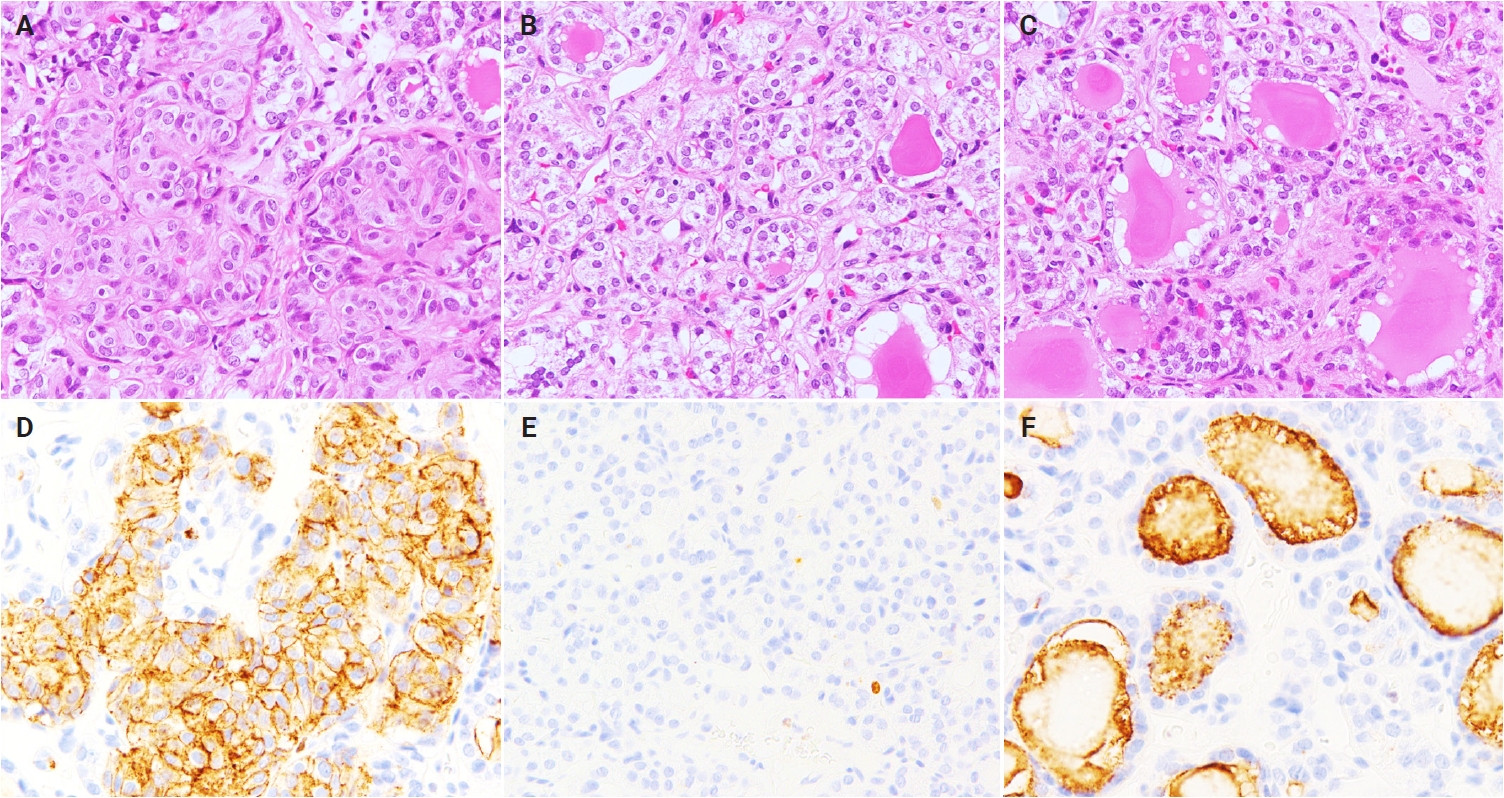
- HTT components consistently exhibited characteristic membranous immunoreactivity for Ki-67 (Fig. 3A, D). In contrast, most areas of the NIFTP-like areas lacked Ki-67 staining (Fig. 3B, E). However, focal apical Ki-67 immunostaining was observed, predominantly in areas adjacent to HTT components (Figs. 3C, F, 4).
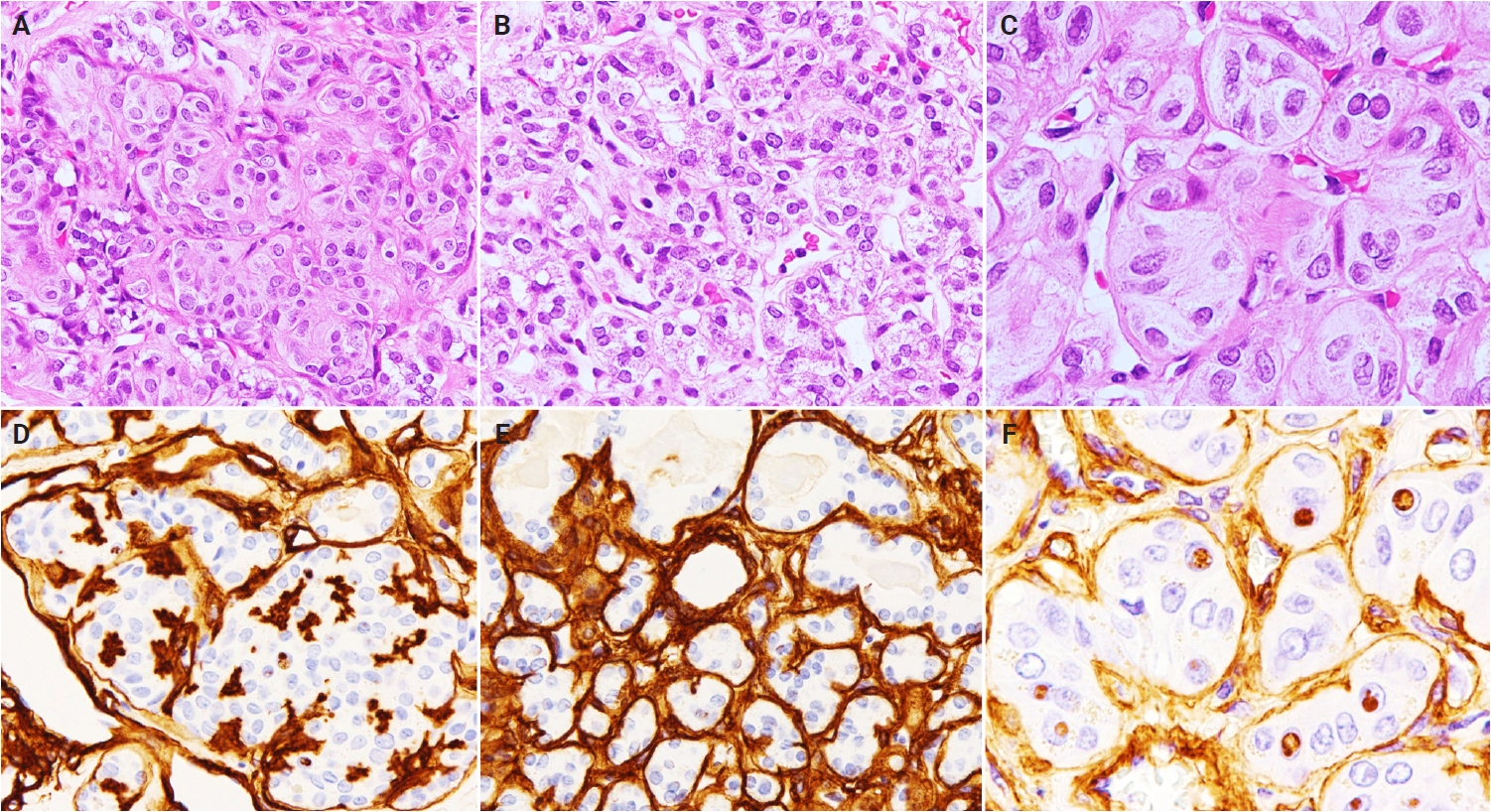
- All HTT components showed intratrabecular deposition of type IV collagen-positive material (Fig. 5A, D), whereas this feature was absent in NIFTP-like areas (Fig. 5B, E). In addition, the intranuclear cytoplasmic inclusions in the HTT components were positive for type IV collagen (Fig. 5C, F).
- None of the control cases (pure NIFTPs, follicular adenomas, or normal thyroid follicular cells) showed membranous or apical Ki-67 immunoreactivity. We observed type IV collagen deposition surrounding tumor nests but not between tumor cells.
- Genetic analyses of four tumors containing both HTT components and NIFTP-like areas demonstrated that the two components shared identical molecular profiles (Table 2). In three tumors (cases 7–9), both components harbored PAX8::GLIS3 fusion, whereas no RAS (KRAS, HRAS, and NRAS) mutations, characteristic of NIFTP, were detected. The remaining tumor showed no PAX8::GLIS3 fusion or RAS mutations. No additional point mutations or gene fusions, including BRAFV600E, RET, or PAX8::PPARγ rearrangements, were identified in any tumors. No cases showed TERT promoter hotspot mutations (C228T/C250T), although the rs2853669 polymorphism was present with variable genotypes.
- Three pure HTT tumors were included as controls; all demonstrated PAX8::GLIS3 fusion and lacked RAS mutations. TERT promoter hotspot mutations were absent, and rs2853669 was detected in all cases.
RESULTS
- All ten tumors examined in this study contained areas fulfilling established diagnostic criteria for HTT [1,2,11]. These areas consistently exhibited a trabecular growth pattern with PTC-like nuclear features, prominent intratrabecular hyalinization, and characteristic membranous Ki‑67 immunoreactivity. In addition, NGS confirmed the presence of PAX8::GLIS3 fusion in three of four cases tested, which, together with the histological and immunophenotypic findings, is highly specific and essentially pathognomonic for HTT [3-6]. Therefore, a diagnosis of HTT based on these components is unequivocal.
- In contrast, other areas within the same tumors showed a predominantly follicular growth pattern with PTC-type nuclear features but lacked papillary architecture, the defining features of HTT, and evidence of invasive growth. These findings are not inconsistent with the histological diagnostic criteria for NIFTP [7]. Accordingly, each tumor appeared to contain two morphologically distinct components: one consistent with the HTT component and the other resembling NIFTP, coexisting within a single lesion.
- To further elucidate the nature of these unusual lesions, we performed molecular analyses focusing on PAX8::GLIS3 fusion and RAS mutations. Both HTT components and NIFTP-like areas shared identical molecular profiles: PAX8::GLIS3 fusion was detected in three of four cases, and no RAS mutations were identified in any tumors. This molecular concordance strongly argues against the presence of two independent neoplasms. Instead, the findings support the interpretation that the NIFTP-like areas represent a morphological variant within the spectrum of HTT rather than a distinct coexisting tumor.
- Our results demonstrate that HTT can exhibit areas closely resembling NIFTP morphology, a phenomenon not previously described to our knowledge. This observation expands the recognized morphological spectrum of HTT and highlights its greater heterogeneity than that traditionally appreciated. In tumors with a predominant NIFTP-like pattern, the characteristic features of HTT may be subtle or overlooked, creating a potential diagnostic pitfall. In such settings, focal apical Ki‑67 immunoreactivity may be a useful ancillary clue supporting the diagnosis of HTT. Accordingly, HTT should be considered in the differential diagnosis of follicular-patterned lesions with PTC-type nuclear features to avoid misclassification as NIFTP.
- An additional notable finding was the presence of type IV collagen with intranuclear cytoplasmic inclusions in HTT cells. These inclusions are generally regarded as cytoplasmic invaginations surrounded by the nuclear membrane [12-14] and, in PTC, are not known to contain basement membrane components [13]. Because type IV collagen is a basement membrane protein [14,15], its presence within these inclusions was unexpected and should theoretically not occur if the inclusions consisted solely of cytoplasmic material. One possible explanation is that the intranuclear cytoplasmic inclusions in HTT incorporate basement membrane substances, including type IV collagen. Regardless of the underlying mechanism, this feature may serve as a useful diagnostic clue for distinguishing HTT from PTC.
- This study has several limitations. The sample size was small, reflecting the rarity of HTT and tumors with mixed HTT and NIFTP-like morphology. As the cohort spans more than 40 years, many archival specimens were older than five years and unsuitable for reliable NGS analysis, and separate macrodissection required each component to contain at least a 5‑mm square of viable tissue; therefore, only four tumors were eligible for molecular testing. Although the two components were intermingled in many areas, macrodissection was performed only on clearly demarcated areas to minimize cross‑contamination, and the absence of discordant driver alterations argues against contamination as the cause of the uniform molecular profiles. Case 10 lacked detectable PAX8::GLIS3 fusion; however, fusion‑negative HTTs have been reported, and the diagnosis should not rely solely on molecular findings when characteristic histological and immunophenotypic features are present. Finally, our molecular testing targeted selected alterations, and broader genomic profiling may further clarify the relationships between these components. Further studies with larger cohorts are required to validate our observations.
- In summary, our findings demonstrate that tumors containing both HTT and NIFTP‑like areas share a uniform molecular profile, including the presence of PAX8::GLIS3 fusion. In this study, “NIFTP‑like” refers only to the morphological resemblance to NIFTP and does not imply a separate neoplastic process. Taken together, the molecular and immunohistochemical concordance indicates that these follicular‑patterned areas represent a morphological variant within the spectrum of HTT. This study clarifies the histogenesis of these tumors and highlights key diagnostic clues—particularly apical Ki‑67 staining—that may prevent misclassification as NIFTP in follicular‑patterned thyroid lesions.
DISCUSSION
Ethics Statement
All procedures performed in the current study were approved by the Institutional Review Board (IRB) of Kuma Hospital on October 12, 2023 (approval No. 20231012-4) in accordance with the 1964 Helsinki declaration and its later amendments. All study participants provided informed consent.
Availability of Data and Material
Data supporting the findings of this study are available from the corresponding author upon request.
Code Availability
Not applicable.
Author Contributions
Conceptualization: RK, MH (Mitsuyoshi Hirokawa). Data curation: RK, SU. Formal analysis: RK, SU. Investigation: RK, SU. Methodology: RK, MH (Mitsuyoshi Hirokawa). Supervision: AS, MH (Miyoko Higuchi), MH (Mitsuyoshi Hirokawa), HK, TA. Validation: RK, SU. Writing—original draft: RK, MH (Mitsuyoshi Hirokawa). Writing—review & editing: AS, MH (Mitsuyoshi Hirokawa), HK, TA. Approval of final manuscript: all authors.
Conflicts of Interest
The authors declare that they have no potential conflicts of interest.
Funding Statement
No funding to declare.
| Case No. | Age (yr) | Sex | Tumor sizea (mm) | Location | Original diagnosis | Encapsulation | Predominant histology | Nuclear score | Ki-67 membranous staining | Ki-67 apical (NIFTP-like) | Type IV collagen (intra-trabecular) | Type IV collagen-positive pseudoinclusions (HTT) | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HTT | NIFTP-like | HTT | NIFTP-like | HTT | NIFTP-like | ||||||||||
| 1 | 62 | F | 30 | Left lobe | HTT | Partial | HTT | 3 | 3 | + | – | + | + | – | + |
| 2 | 28 | M | 54 | Right lobe | HTT | Partial | NIFTP | 3 | 2 | + | – | + | + | – | + |
| 3 | 64 | F | 6 | Isthmus | HTT | Partial | HTT | 3 | 3 | + | – | + | + | – | + |
| 4 | 66 | M | 40 | Left lobe | HTT | Absent | HTT | 3 | 3 | + | – | + | + | – | + |
| 5 | 75 | F | 17 | Right lobe | HTT | Absent | HTT | 3 | 3 | + | – | + | + | – | + |
| 6 | 42 | F | 16 | Right lobe | HTT | Absent | HTT | 3 | 3 | + | – | + | + | – | + |
| 7 | 45 | F | 15 | Isthmus | HTT | Partial | HTT | 3 | 3 | + | – | + | + | – | + |
| 8 | 56 | F | 23 | Right lobe | HTT | Partial | HTT | 3 | 3 | + | – | + | + | – | + |
| 9 | 35 | F | 15 | Right lobe | HTT | Absent | NIFTP | 3 | 3 | + | – | + | + | – | + |
| 10 | 55 | F | 11 | Right lobe | HTT | Absent | NIFTP | 3 | 3 | + | – | + | + | – | + |
Only four tumors (cases 7–10 in Table 1) fulfilled the technical requirements for molecular testing, including (1) archival tissue age ≤5 years to ensure reliable NGS performance and (2) availability of ≥5‑mm viable tissue in both HTT and NIFTP‑like areas for separate macrodissection. The same case numbers are used in Table 2 to indicate the tumors that underwent molecular analysis.
NGS, next-generation sequencing; HTT, hyalinizing trabecular tumor; NIFTP, noninvasive follicular thyroid neoplasm with papillary-like nuclear features; +, present; –, absent.
- 1. Baloch ZW, Asa SL, Barletta JA, et al. Overview of the 2022 WHO classification of thyroid neoplasms. Endocr Pathol 2022; 33: 27-63. ArticlePubMedPDF
- 2. Hirokawa M, Carney JA. Cell membrane and cytoplasmic staining for MIB-1 in hyalinizing trabecular adenoma of the thyroid gland. Am J Surg Pathol 2000; 24: 575-8. ArticlePubMed
- 3. Nikiforova MN, Nikitski AV, Panebianco F, et al. GLIS rearrangement is a genomic hallmark of hyalinizing trabecular tumor of the thyroid gland. Thyroid 2019; 29: 161-73. ArticlePubMedPMC
- 4. Marchio C, Da Cruz Paula A, Gularte-Merida R, et al. PAX8-GLIS3 gene fusion is a pathognomonic genetic alteration of hyalinizing trabecular tumors of the thyroid. Mod Pathol 2019; 32: 1734-43. ArticlePubMedPMCPDF
- 5. Nikiforova MN, Nikiforov YE, Ohori NP. GLIS rearrangements in thyroid nodules: a key to preoperative diagnosis of hyalinizing trabecular tumor. Cancer Cytopathol 2019; 127: 560-6. ArticlePubMedPDF
- 6. Alsugair Z, Descotes F, Lopez J, Decaussin-Petrucci M. Hyalinizing trabecular tumor of the thyroid: interest of GLIS3 immunohistochemical study to detect PAX8::GLIS3 rearrangement. Hum Pathol 2025; 157: 105761.ArticlePubMed
- 7. Nikiforov YE, Seethala RR, Tallini G, et al. Nomenclature revision for encapsulated follicular variant of papillary thyroid carcinoma: a paradigm shift to reduce overtreatment of indolent tumors. JAMA Oncol 2016; 2: 1023-9. ArticlePubMedPMC
- 8. Cipriani NA, Johnson DN, Sarne DH, Angelos P, Reeves W, Antic T. The significance of RAS-like mutations and microRNA profiling in predicting malignancy in thyroid biopsy specimens. Endocr Pathol 2022; 33: 446-56. ArticlePubMedPDF
- 9. Hernandez-Prera JC, Wenig BM. RAS-mutant follicular thyroid tumors: a continuous challenge for pathologists. Endocr Pathol 2024; 35: 167-84. ArticlePubMedPDF
- 10. Takada N, Hirokawa M, Ohbayashi C, et al. Re-evaluation of MIB-1 immunostaining for diagnosing hyalinizing trabecular tumour of the thyroid: semi-automated techniques with manual antigen retrieval are more accurate than fully automated techniques. Endocr J 2018; 65: 239-44. ArticlePubMed
- 11. Ohori NP, Hirokawa M, Rossi ED, Bongiovanni M, Bellevicine C. Challenging subtypes and mimics of papillary thyroid carcinoma: highlights from a 22nd International Congress of Cytology Slide Seminar (case reports). Acta Cytol 2026 Jan 21 [Epub]. https://doi.org/10.1159/000550625. ArticlePubMed
- 12. Kaneko C, Shamoto M, Niimi H, Osada A, Shimizu M, Shinzato M. Studies on intranuclear inclusions and nuclear grooves in papillary thyroid cancer by light, scanning electron and transmission electron microscopy. Acta Cytol 1996; 40: 417-22. ArticlePubMed
- 13. Inoue T, Ohno N, Oishi N, Mochizuki K, Katoh R, Kondo T. Three-dimensional structural analysis of papillary thyroid carcinoma nuclei with serial block-face scanning electron microscopy (SBF-SEM). Pathol Int 2023; 73: 341-50. ArticlePubMedPMC
- 14. Ohtsuki Y, Kimura M, Murao S, et al. Immunohistochemical and electron microscopy studies of a case of hyalinizing trabecular tumor of the thyroid gland, with special consideration of the hyalinizing mass associated with it. Med Mol Morphol 2009; 42: 189-94. ArticlePubMedPDF
- 15. Katoh R, Jasani B, Williams ED. Hyalinizing trabecular adenoma of the thyroid: a report of three cases with immunohistochemical and ultrastructural studies. Histopathology 1989; 15: 211-24. ArticlePubMed
REFERENCES
Figure & Data
References
Citations
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-
- Related articles
-
- Mutational status of non-invasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP): molecular analysis should be performed for NIFTPs with nuclear score 3
- Noninvasive follicular thyroid neoplasm with papillary-like nuclear features: its updated diagnostic criteria, preoperative cytologic diagnoses and impact on the risk of malignancy
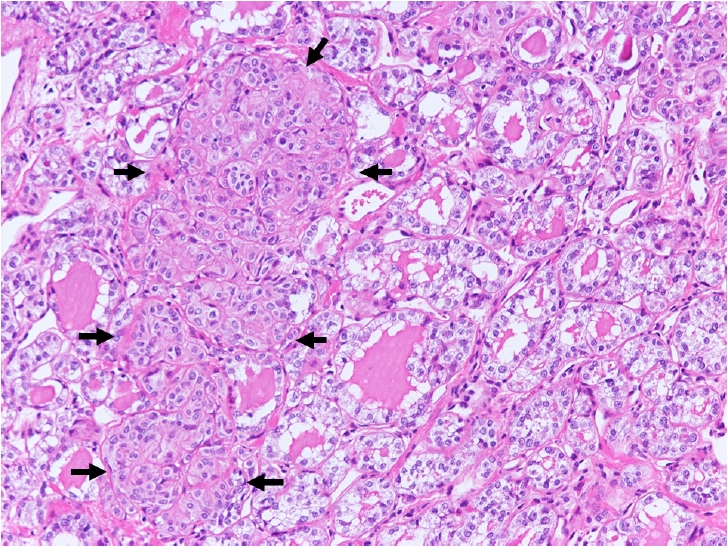
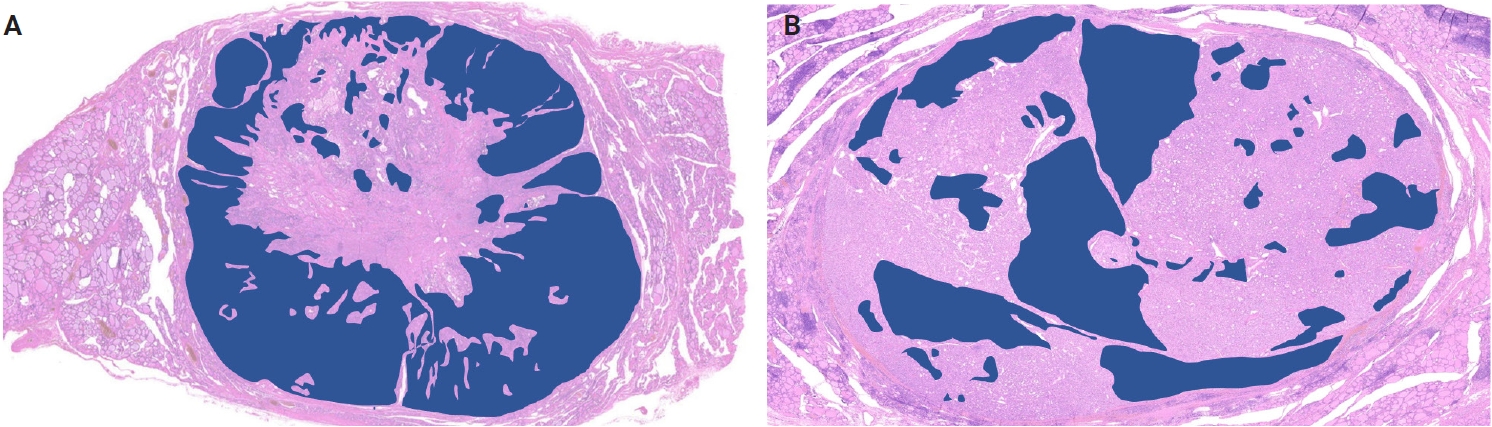
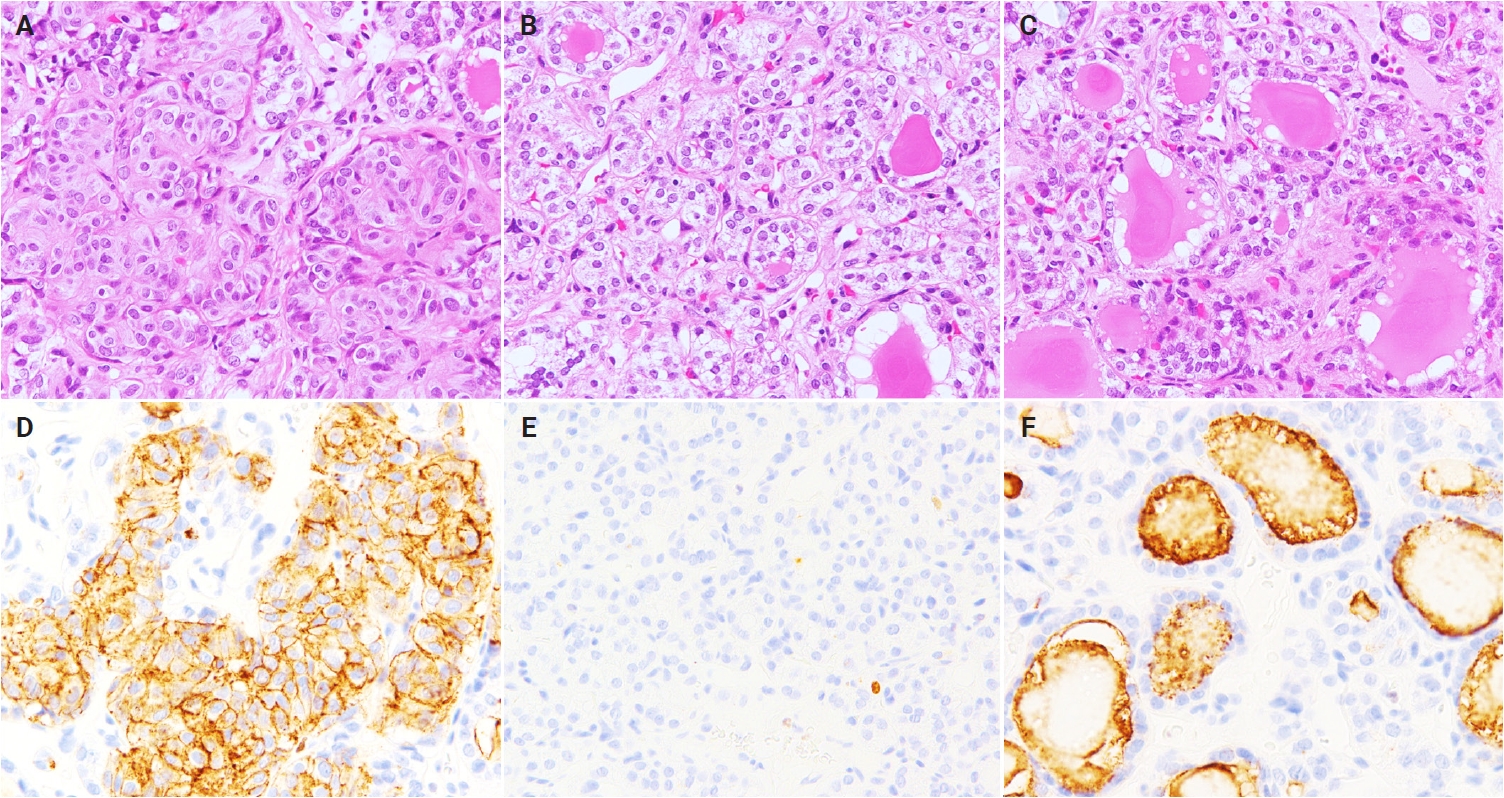
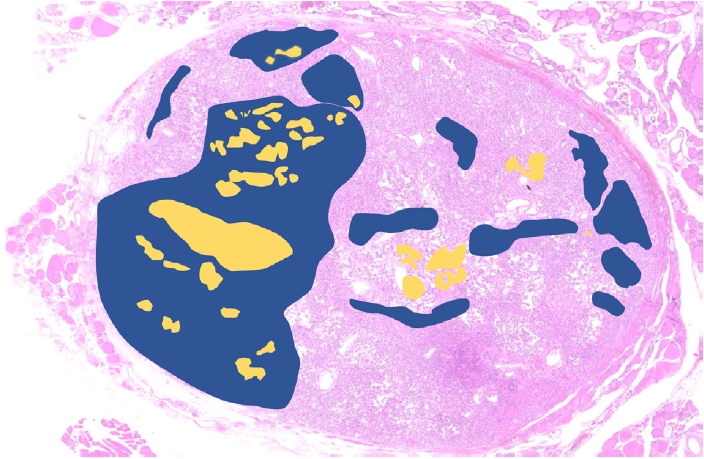
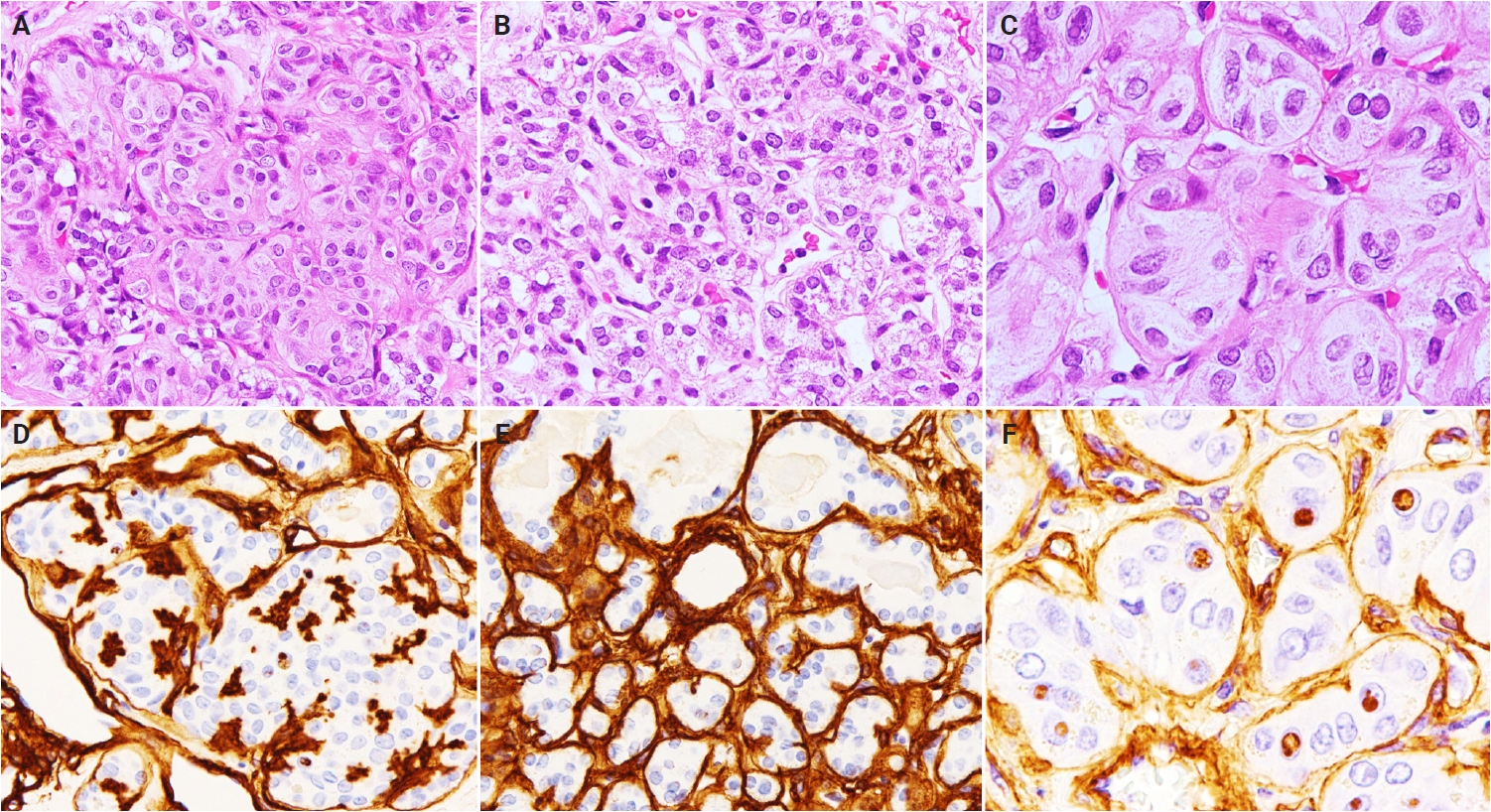

Fig. 1.
Fig. 2.
Fig. 3.
Fig. 4.
Fig. 5.
Graphical abstract
| Case No. | Age (yr) | Sex | Tumor size |
Location | Original diagnosis | Encapsulation | Predominant histology | Nuclear score | Ki-67 membranous staining | Ki-67 apical (NIFTP-like) | Type IV collagen (intra-trabecular) | Type IV collagen-positive pseudoinclusions (HTT) | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HTT | NIFTP-like | HTT | NIFTP-like | HTT | NIFTP-like | ||||||||||
| 1 | 62 | F | 30 | Left lobe | HTT | Partial | HTT | 3 | 3 | + | – | + | + | – | + |
| 2 | 28 | M | 54 | Right lobe | HTT | Partial | NIFTP | 3 | 2 | + | – | + | + | – | + |
| 3 | 64 | F | 6 | Isthmus | HTT | Partial | HTT | 3 | 3 | + | – | + | + | – | + |
| 4 | 66 | M | 40 | Left lobe | HTT | Absent | HTT | 3 | 3 | + | – | + | + | – | + |
| 5 | 75 | F | 17 | Right lobe | HTT | Absent | HTT | 3 | 3 | + | – | + | + | – | + |
| 6 | 42 | F | 16 | Right lobe | HTT | Absent | HTT | 3 | 3 | + | – | + | + | – | + |
| 7 | 45 | F | 15 | Isthmus | HTT | Partial | HTT | 3 | 3 | + | – | + | + | – | + |
| 8 | 56 | F | 23 | Right lobe | HTT | Partial | HTT | 3 | 3 | + | – | + | + | – | + |
| 9 | 35 | F | 15 | Right lobe | HTT | Absent | NIFTP | 3 | 3 | + | – | + | + | – | + |
| 10 | 55 | F | 11 | Right lobe | HTT | Absent | NIFTP | 3 | 3 | + | – | + | + | – | + |
| Case | Histological component | Point mutations | Fusions | TERT promoter | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| RAS(K/H/N)/RAS-like | BRAF (V600E) | RET | Others | PAX8::PPARG | RET::CCDC6 | PAX8::GLIS3 | PAX8::GLIS1 | C228T/C250T | rs2853669 | ||
| 7 | HTT | – | – | – | – | – | – | + | – | – | T/T |
| NIFTP | – | – | – | – | – | – | + | – | – | ||
| 8 | HTT | – | – | – | – | – | – | + | – | – | C/T |
| NIFTP | – | – | – | – | – | – | + | – | – | ||
| 9 | HTT | – | – | – | – | – | – | + | – | – | C/T |
| NIFTP | – | – | – | – | – | – | + | – | – | ||
| 10 | HTT | – | – | – | – | – | – | – | – | – | T/T |
| NIFTP | – | – | – | – | – | – | – | – | – | ||
| Control 1 | HTT | – | – | – | – | – | – | + | – | – | C/T |
| Control 2 | HTT | – | – | – | – | – | – | + | – | – | C/T |
| Control 3 | HTT | – | – | – | – | – | – | + | – | – | C/C |
HTT, hyalinizing trabecular tumor; NIFTP, noninvasive follicular thyroid neoplasm with papillary-like nuclear features; +, presence; –, absence. Greatest dimension.
Only four tumors (cases 7–10 in NGS, next-generation sequencing; HTT, hyalinizing trabecular tumor; NIFTP, noninvasive follicular thyroid neoplasm with papillary-like nuclear features; +, present; –, absent.

