 E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 60(4); 2026 > Article
-
Original Article
The impairment of CD3+ T lymphocytes in sentinel lymph node of high-risk cutaneous melanoma patients in stage IIB and IIC -
Emilija Filipović1
 , Katarina Mirjačić Martinović2, Ognjen Živković3, Nataša Medić Milijić3, Ana Lazarević3, Zoran Bukumirić4, Marko Jevrić1,5, Milan Žegarac1,5
, Katarina Mirjačić Martinović2, Ognjen Živković3, Nataša Medić Milijić3, Ana Lazarević3, Zoran Bukumirić4, Marko Jevrić1,5, Milan Žegarac1,5 -
Journal of Pathology and Translational Medicine 2026;60(4):422-435.
DOI: https://doi.org/10.4132/jptm.2026.04.02
Published online: April 15, 2026
1Clinic of Surgical Oncology, Institute of Oncology and Radiology of Serbia, Belgrade, Serbia
2Department of Experimental Oncology, Institute of Oncology and Radiology of Serbia, Belgrade, Serbia
3Department of Pathology, Institute of Oncology and Radiology of Serbia, Belgrade, Serbia
4Institute for Medical Statistics and Informatics, Faculty of Medicine, University of Belgrade, Belgrade, Serbia
5School of Medicine, University of Belgrade, Belgrade, Serbia
- Corresponding Author: Katarina Mirjačić Martinović, MD, PhD Department of Experimental Oncology, Institute of Oncology and Radiology of Serbia, Pasterova 14, 11000 Belgrade, Serbia Tel: + 381-64-210-8778, Fax: +381-(0)-11-2685-300, E-mail: katarina.mirjacic@ncrc.ac.rs
© The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 61 Views
- 3 Download
Abstract
-
Background
- The sentinel lymph node (SLN) in melanoma is almost always the first site of metastasis and its histopathological assessment is essential for the determination of staging and clinical outcome. Furthermore, this procedure offers the investigation of the early immune response in SLN as melanoma-derived factors suppress the immunity in an early stage that may facilitate metastasis. A better understanding of the immunological changes in SLN may help in the therapeutic stimulation of melanoma immunity to prevent tumor metastasis.
-
Methods
- SLN tissues without malignant cells from 74 cutaneous melanoma patients (stage I and II) were analyzed. By flow cytometry, we measured the percentage of natural killer cells, CD3+ T lymphocytes, and their expression of interferon-γ (IFN-γ) and inhibitory immune checkpoint molecules (ICMs), and the percentage of CD4+Foxp3+ regulatory T cells (Tregs).
-
Results
- Melanoma patients with worse prognosis, in stage IIB–C, had decreased percentage of total CD3+ and CD3+CD8+ T lymphocytes, trend of IFN-γ decrease, increased inhibitory programmed cell death 1 and T cell immunoglobulin and mucin-domain containing 3 ICMs, and higher percentage of Tregs in their SLNs compared with stage I-IIA patients. Furthermore, patients with nodular melanoma had decreased CD3+CD8+ cells compared with patients with superficial spreading melanoma and together with patients with localization of primary tumor on extremities had an increase in the expression of analyzed ICMs.
-
Conclusions
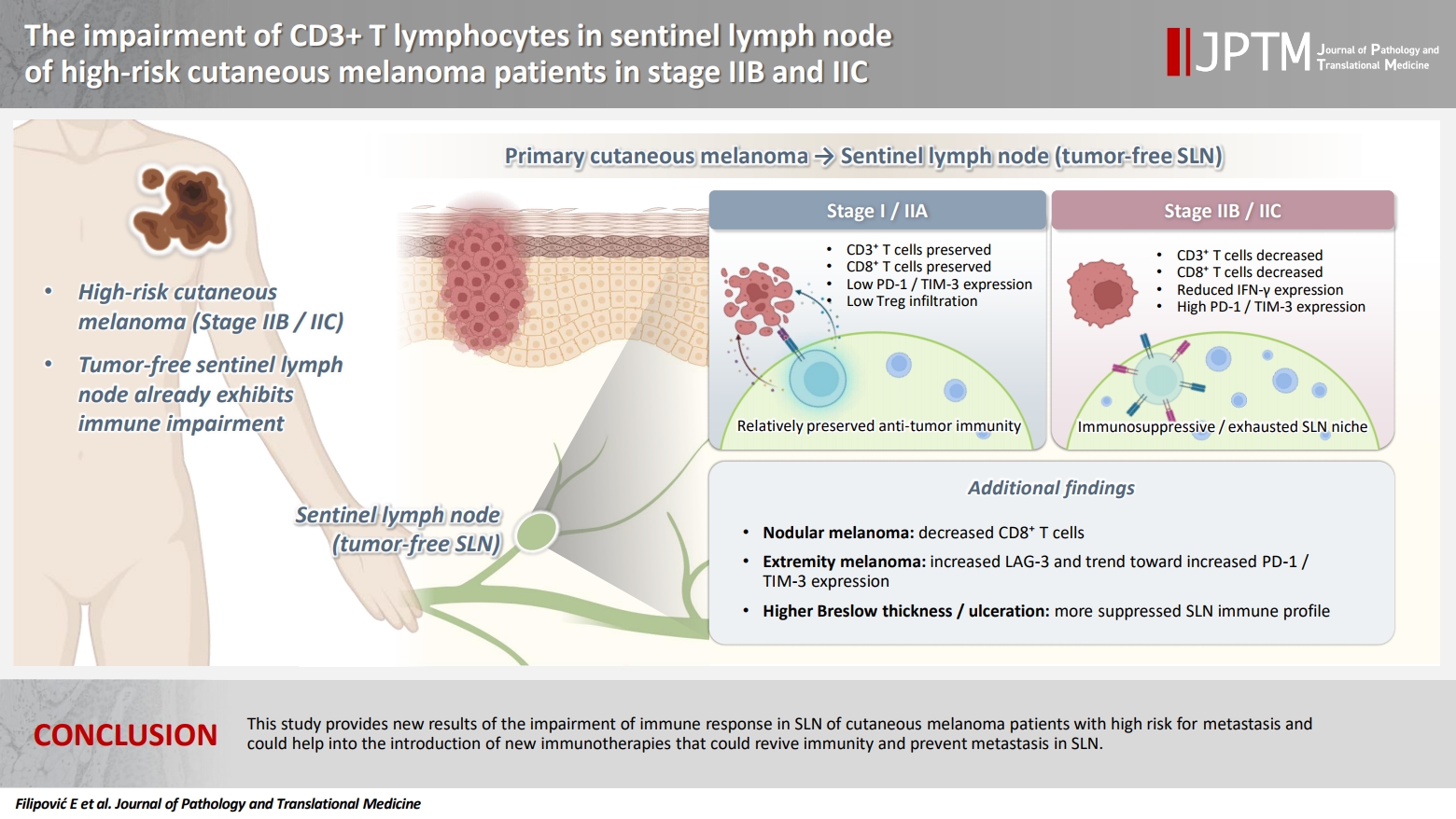
- This study provides new results of the impairment of immune response in SLN of cutaneous melanoma patients with high risk for metastasis and could help in the introduction of new immunotherapies that could restore immunity and prevent metastasis in SLN.
- Melanoma is the most severe type of skin cancer, originating from melanocytes, the cells that produce melanin. This cancer primarily affects the skin, but melanoma may rarely develop in the mouth, intestines, or eye. Although it is a rare cancer, the incidence of melanoma has continuously increased over the last 50 years [1]. Although melanoma cells spread rapidly from the primary tumor to the distant organs through the bloodstream, tumor cells often use the lymphatic system for metastatic progression [2].
- The sentinel lymph node (SLN) is the first lymph node to receive drainage directly from a tumor and is almost always the first site of melanoma metastasis. Histopathological assessment of SLN for the presence of metastatic cells is essential for melanoma staging and its results may represent a key predictor of disease outcome, recommended by the National Comprehensive Cancer Network [3]. Additionally, this procedure offers an excellent opportunity to investigate the early immune response to tumor antigens in SLN.
- It is known that lymph nodes (LNs) as secondary lymphoid tissue are the foci of lymphocytes. Under physiological conditions, they play a central role in immunosurveillance of non-self-antigens to which they are exposed via afferent lymph. Therefore, SLNs are critical sites of antigen presentation and the activation of the cells of adaptive immune system against tumor [4]. However, SLN is also the first tumor-draining LN exposed to inhibitory factors secreted from primary tumor [5]. These mediators including cytokines (interleukin [IL]-1β, IL-6, IL-8, IL-10, transforming growth factor β [TGF-β]), chemokines (CXCL1, CXCL2, CXCL8, and CCL2), growth factors (vascular endothelial growth factor [VEGF]), as well as enzyme indoleamine 2,3-dioxygenase enable cancer cell–mediated evasion of immunosurveillance and can serve as immunosuppressants, facilitating melanoma cells to invade LNs. These factors play the role in the differentiation, proliferation and activation of numerous immunosuppressive cells such as myeloid-derived suppressor cells, regulatory T cells (Tregs), tumor-associated macrophages that play an important role in tumor growth and metastasis by inhibiting anti-tumor activity of CD3+CD4+ helper T (Th) cells, CD3+CD8+ cytotoxic T lymphocytes (CTLs), natural killer (NK) cells [5,6]. These inhibitory factors also alter the functions of dendritic cells (DCs) within the SLN, leading to failures in tumor antigen presentation and T-cell activity [7]. These processes promote the maintenance of an immunosuppressive microenvironment, so-called premetastatic niche (PMN), in SLN and favor early metastasis in SLN [5,6].
- Immunomodulators and blockers of inhibitory melanoma-secreted mediators are under clinical investigation for the prevention of lymphatic metastasis as they interrupt PMN development. Understanding the mechanisms of PMN formation offers an opportunity for developing new therapeutic approaches that could prevent melanoma metastasis in high-risk melanoma patients with local, cutaneous tumor [8]. Therefore, new immune therapies, immune checkpoint inhibitors (ICIs), monoclonal antibodies (mAbs) that block inhibitory molecules that are highly expressed on the surface of immune and tumor cells in tumor microenvironment (TME) such as cytotoxic T lymphocyte-associated protein 4 (CTLA-4), programmed cell death 1 (PD-1), programmed cell death ligand 1 (PD-L1), lymphocyte activation gene-3 (LAG-3), T cell immunoglobulin and mucin-domain containing 3 (TIM-3) restore the immune system by increasing T and NK cell–mediated anti-tumor activity. Therefore, ICIs could enable tumor regression and long-term cancer control in melanoma patients [9].
- There is little data in the literature on the immunophenotypic and functional characteristics of lymphocytes in still intact, non-metastatic SLN in patients with cutaneous, localized melanoma. For this reason, this research should provide completely new data related to the potential difference in the percentage and function of T lymphocytes and their subsets, as well as the expression of inhibitory molecules, PD-1, LAG-3, and TIM-3 on their surface between patients in clinical stage II with a worse prognosis and higher possibility of metastasis compared with the patients in clinical stage I. Although, a few years ago, the Food and Drug Administration (FDA) approved the application of anti–PD-1 mAbs, pembrolizumab and nivolumab, for adjuvant therapy in high-risk melanoma patients in stage IIB or IIC [10], it remains an open question whether all these patients are candidates for treatment with this therapy, considering its potential side effects and possible resistance.
- The results of this research could contribute to a more precise selection of patients in whom this therapy would give the best clinical response. Furthermore, the results related to the expression of not only PD-1, but also the less analyzed LAG-3 and TIM-3 inhibitory molecules on the surface of SLN lymphocytes could show their importance in reducing the function of T lymphocytes, as well as the potentially great importance of their therapeutic blockade in patients with a high risk of metastasis in stage II of melanoma.
INTRODUCTION
- Patients and SLN analysis
- In this prospective study, we analyzed the samples of SLN tissue from 80 patients with cutaneous melanoma, aged over 18 years, regardless of their race, sex, or ethnic origin, who underwent the biopsy of SLN at the Institute of Oncology and Radiology of Serbia (IORS). The research was ongoing from April 2024 to August 2025. For diagnostic purposes, SLNs are routinely analyzed for the presence of melanoma cells in patients who have melanomas with Breslow thickness ≥ 0.8 mm or thinner but with the presence of ulceration (stage T1b and higher according to the TNM tumor classification), and do not have clinically and diagnostically observed signs of pathological lymphadenopathy and/or metastatic changes [11]. Patients under the age of 18, as well as patients with infectious, autoimmune diseases, acute or chronic inflammation of the other origin, were excluded from the research. For the purpose of SLN checking, preoperatively, a marker, a radioactive isotope Tc99m was injected intradermally into the region of the scar from the removed melanoma, and immediately preoperatively another marker, a vital dye (methylene blue), was injected in the same way. During the surgical intervention, a lymph node that received one or both markers was removed from the regional lymph pool, which is considered to be the SLN. SLNs are either positive or negative for melanoma cells based on the pathohistological analysis of serial sections by hematoxylin and eosin and immunohistochemical staining. In the case of a positive SLN, patients are classified in clinical stage III of the disease, and in the case of a negative SLN in stage I or II, depending on the thickness of the primary melanoma and the presence of ulceration. A random section of SLN tissue (maximum 1 mm thick) from each patient, obtained fresh by the pathologist immediately after surgery, was transferred to cryovials and cryopreserved at –150°C for storage and later analysis. As only six patients had metastasis in their SLNs (stage III), the aim of this study was to analyze the immunological parameters of 74 patients with melanoma cell-negative SLNs (clinical stage I and II). The characteristics of patients in clinical stages I and II and their primary tumors are included in Table 1.
- Mononuclear cell isolation
- In order to form single cell suspension, SLN tissue samples were mechanically minced with sterile scalpel and filtered through a 100 μm mesh to exclude undissociated fragments. Mononuclear cells (MNCs), lymphocytes, and monocytes, were isolated using Histopaque (Sigma-Aldrich Chemie, Steinheim, Germany) density gradient, centrifuged at 1,600 rpm for 40 minutes and washed three times in RPMI 1640 cell culture medium (CM) supplemented with 10% fetal calf serum (Sigma-Aldrich).
- Flow cytometric analysis
- The percentage of total T lymphocytes and their different subpopulations, the percentage of NK cells, as well as the expression of inhibitory receptors, PD-1, LAG-3, TIM-3, on the surface of total T cells in the lymphocyte population in freshly isolated MNCs originating from SLNs of patients with skin melanoma were determined by the method of direct three-color immunofluorescence on a flow cytometer (FACSCalibur, Becton Dickinson, San Jose, CA, USA) using mAbs marked with fluorescent dyes. Samples for analysis were prepared according to the method of Jackson and Warner [12]. Namely, 5 × 105 freshly isolated MNCs in a suspension of 100 μL (concentration 5 × 106 cells/mL) were incubated for 30 minutes at 4°C with 10 μL of the appropriate combination of mAbs and then washed twice by centrifugation at 1,600 rpm in cold phosphate buffer solution (PBS) (CellWASH, Becton Dickinson) and for analysis on a flow cytometer resuspended in 1% paraformaldehyde (CellFIX, Becton Dickinson).
- In the suspension of peripheral blood lymphocytes and monocytes, about 20,000 cells per sample were collected and verified as lymphocytes according to their physical characteristics: size (forward scatter) and granularity (side scatter), gated and analyzed using CellQUEST software. The degree of non-specific immunofluorescence was determined using matched isotype-identical, IgG1 mAbs controls (Becton Dickinson). In more detail, according to convention, we used the 1% level to separate negative and positive cells. The markers were placed to delineate a region of positive intensity maximum 1% of negative control cells.
- The following combinations of mAbs labeled with fluorescent dyes were used: CD8FITC/CD4PE/CD3APC, CD56FITC/PD-1PE/CD3APC, LAG-3FITC/TIM-3PE/CD3APC, CD25FITC/Foxp3PE/CD4PerCP (Becton Dickinson). Total T lymphocytes were detected and analyzed as CD3+ lymphocytes, Th lymphocytes as CD3+CD4+, CTLs as CD3+CD8+, NK cells as CD3–CD56+, and NKT-like cells as CD3+CD56+ lymphocytes. The expression in percentage of PD-1, LAG-3, and TIM-3 molecules was determined on the surface of total CD3+ T lymphocytes.
- For the analysis of the percentage of Tregs within the SLN tissue by the flow cytometry method, a sample of 1 × 106 MNCs isolated from the SLN tissue of melanoma patients was prepared and resuspended in 100 μL of CM. External antigens that determine the immunophenotype of Treg cells were labeled with 10 μL of mAbs conjugated with fluorescent dyes, CD25FITC and CD4PerCP (Becton Dickinson) and incubated for 30 minutes at 4°C. After that, the samples were washed twice by centrifugation at 1,600 rpm in a cold PBS. After the staining of external antigens, according to the standard procedure of permeabilization, the MNCs were exposed to the BD FACS solution 2 for permeabilization of cells containing the detergent saponin (Perm 2, BD Biosciences) and after that, for the labeling of intracellular Foxp3, 10 μL of anti-Foxp3 PE monoclonal antibody (Becton Dickinson) was added to each sample. After two washes in cold PBS, samples were dissolved in 1% paraformaldehyde for flow cytometer analysis. In the lymphocyte population of SLN, the percentage of Tregs was analyzed as the percentage of Foxp3+ and CD4+Foxp3+ cells.
- Interferon-γ measurement
- The flow cytometry method was used to determine the expression of synthesized interferon-γ (IFN-γ) in CD3+ T cells. A sample of 5 × 105 MNCs isolated from SLN tissue of a melanoma patient was prepared and resuspended in 500 μL CM. MNCs prepared in this way were cultured at a temperature of 37°C in polystyrene test tubes for flow cytometry with 50 ng/mL phorbol-12-myristate-13-acetate (PMA) (Sigma-Aldrich) and 500 ng/mL ionomycin (Sigma-Aldrich), which have the role to stimulate the synthesis of IFN-γ. After 1 hour of incubation with PMA and ionomycin, 10 mg/mL brefeldin A (Sigma-Aldrich) was added to prevent the transport of synthesized proteins from the cells into the external environment. After an additional 3 hours (a total of 4 hours of treatment), 10 μL of a monoclonal antibody conjugated with a fluorescent dye, CD3 FITC (Becton Dickinson), was added to the MNCs and the labeled MNCs were incubated for 30 minutes at 4°C. After that, the samples were washed twice by centrifugation at 1,600 rpm in a cold PBS. After external antigen staining, according to the standard procedure for permeabilization, the MNC sediment was exposed to Perm 2 solution and then 10 μL of anti–IFN-γPE monoclonal antibody (Becton Dickinson) was added to each sample to label intracellular IFN-γ. After two washes in cold PBS, the samples were dissolved in 1% paraformaldehyde. In the lymphocyte population of the SLN tissue, the percentage of CD3+ T cells containing IFN-γ was determined.
- Statistical analysis
- The obtained results were analyzed using the non-parametric test, the Mann-Whitney exact test of unpaired data by the GraphPad Prism program (GraphPad Software Inc., San Diego, CA, USA). Correlations between data were determined by Spearman's rank correlation. The differences between the compared groups were statistically significant or there was a correlation between investigated parameters if the calculated p-value was less than or equal to .05.
MATERIALS AND METHODS
- The percentage of T and NK cells
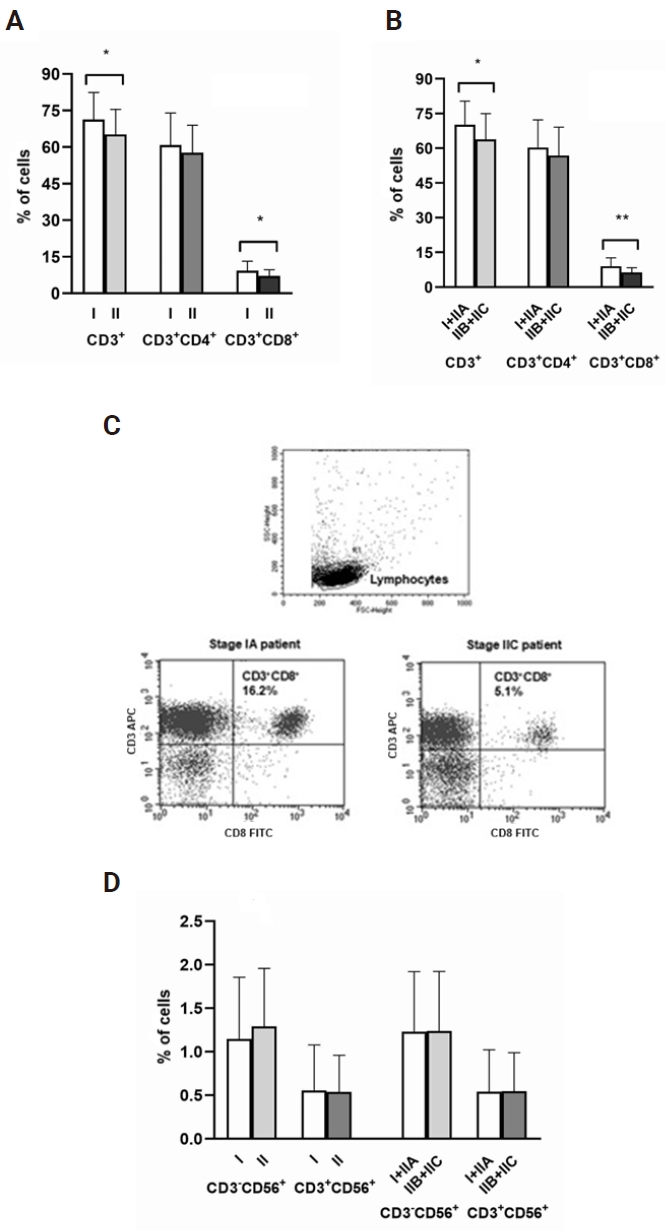
- In this study, we analyzed the percentage of T lymphocyte subsets and NK cells in the samples of SLN tissue from 74 patients with cutaneous, localized melanoma in clinical stages I and II. We have found that patients in stage II and especially in stages IIB and IIC had statistically significant decrease (p ≤ .05 and p < .01, Mann-Whitney exact test) in the percentage of total CD3+ and cytotoxic CD3+CD8+ T cells compared with the percentage of these cells in the patients in stage I, as well as in stage I and stage IIA together (Fig. 1A–C). However, there was no difference (p > .5, Mann-Whitney exact test) in the percentage of helper CD3+CD4+ T cells, as well as CD3–CD56+ NK and CD3+CD56+ NKT-like cells between investigated groups of melanoma patients (Fig. 1A, B, D).
- The expression of IFN-γ in T cells
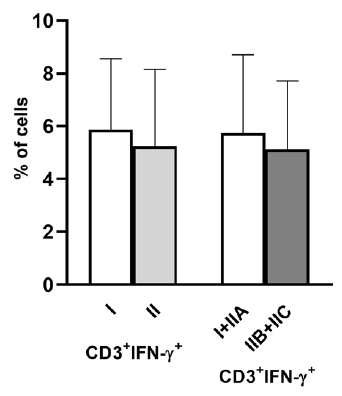
- Analyzing the expression of IFN-γ in T cells of SLNs, we have shown that there was no statistically significant difference (p > .5, Mann-Whitney exact test) in the percentage of this cytokine in CD3+ T cells between melanoma patients in stage I and stage II, as well as in stage I + IIA and stage IIB + IIC. However, there was a trend of decreased expression of IFN-γ in CD3+ T cells between the analyzed groups of melanoma patients (Fig. 2).
- The expression of PD-1, TIM-3, and LAG-3 on T cells
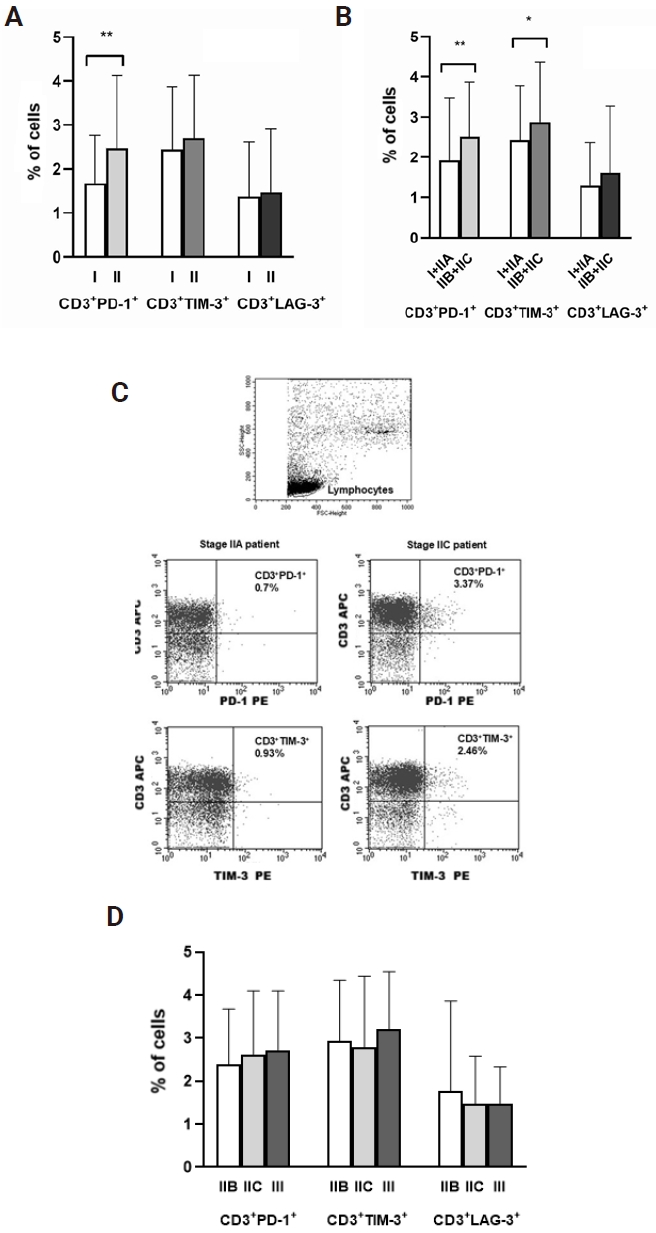
- Analyzing the expression of inhibitory molecules PD-1, TIM-3, and LAG-3 on T cells in SLN tissue we have found that the percentage of PD-1 molecule was significantly higher (p < .01, Mann-Whitney exact test) in melanoma patients in stage II compared with patients in stage I (Fig. 3A). Additionally, melanoma patients in stage IIB and IIC, besides significantly higher expression of PD-1 molecule (p < .01, Mann-Whitney exact test), had significantly increased expression of the other inhibitory molecule, TIM-3 (p ≤ .05, Mann-Whitney exact test) on CD3+ T cells compared with the patients in stage I and IIA (Fig. 3B, C). However, analyzing the expression of all analyzed inhibitory molecules on T cells in SLNs in patients in stage IIB and IIC, as well as in patients in stage III (n = 6), we found no difference (p > .5, Mann-Whitney exact test) in their values (Fig. 3D).
- The percentage of Tregs
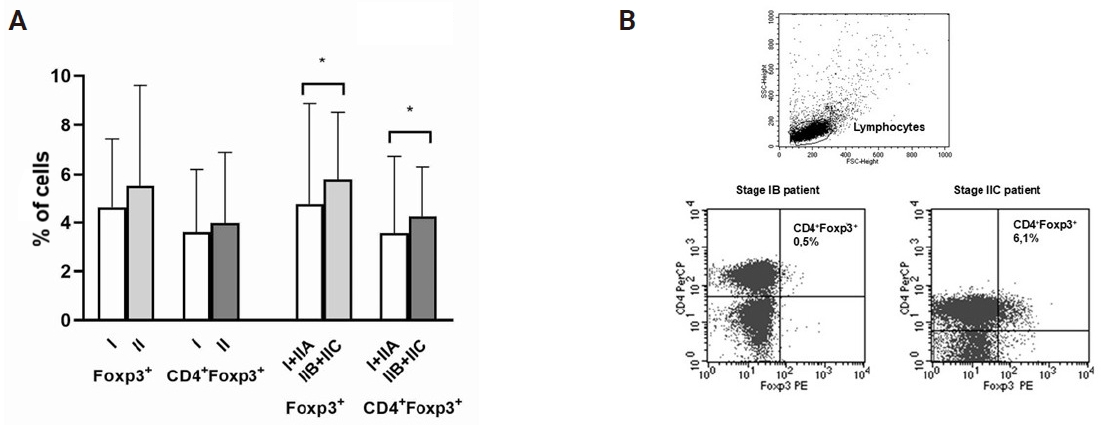
- In melanoma patients in stage I and stage II, we also analyzed the percentage of Tregs in their SLNs. We have shown that there was no statistically significant difference (p > .5, Mann-Whitney exact test) in the percentage of Foxp3+ and CD4+ Foxp3+ Tregs between melanoma patients in stage I and stage II (Fig. 4A). However, melanoma patients in stage IIB and IIC had significantly higher percentage (p ≤ .05, Mann-Whitney exact test) of Foxp3+ and CD4+ Foxp3+ Treg cells in SLNs compared with the percentage of these cells in stage I and IIA (Fig. 4A, B).
- The association between the percentage of immune cells in SLN and different histological characteristics of primary melanoma
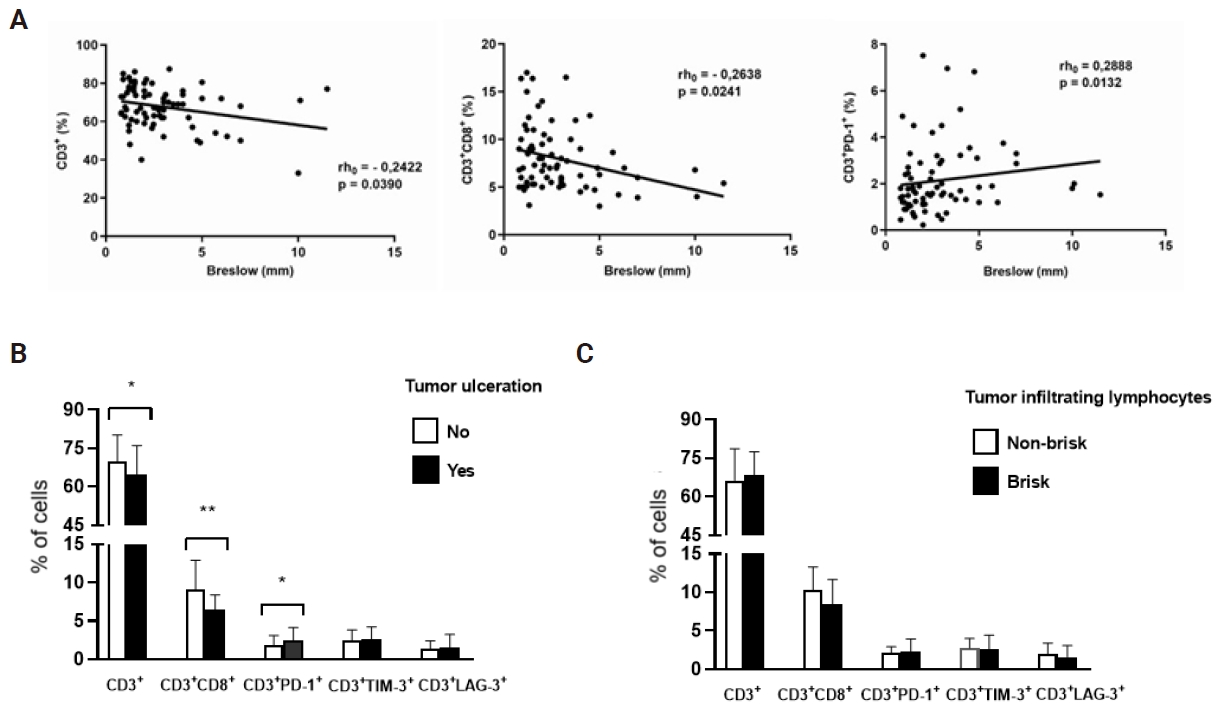
- Analyzing the association between the percentage of immune cells in SLNs and histological characteristics of primary melanoma, we found a negative correlation (p ≤ .05, Spearman rank correlation) between primary tumor thickness (Breslow) and the percentage of total CD3+, as well as CD3+CD8+ T cells in SLNs of investigated melanoma patients. Contrary to these results, we showed a positive correlation (p ≤ .05, Spearman rank correlation) between Breslow thickness and the percentage of CD3+PD-1+ T lymphocytes (Fig. 5A). Furthermore, the patients with ulceration in primary tumor had statistically significant decrease (p ≤ .05 and p < .01, Mann-Whitney exact test) in the percentage of CD3+ and CD3+CD8+ T cells, as well as significant increase (p ≤ .05, Mann-Whitney exact test) in the percentage of CD3+PD-1+ cells compared with the percentage of these cells in the patients without primary tumor ulceration. However, there was no difference (p > .5, Mann-Whitney exact test) in the percentage of CD3+TIM-3+ and CD3+LAG-3+ cells between investigated groups of melanoma patients (Fig. 5B). On the other hand, there was no statistically significant difference (p > .5, Mann-Whitney exact test) in the percentage of analyzed immune cells (CD3+ and CD3+CD8+ T cells), as well as in the expression of inhibitory PD-1, TIM-3, and LAG-3 molecules on CD3+ T cells between patients with focal (non-brisk) and dense (brisk) lymphocyte infiltrate in their primary tumors (Fig. 5C).
- The association between the percentage of immune cells in SLN and different histological subtypes and localizations of primary melanoma
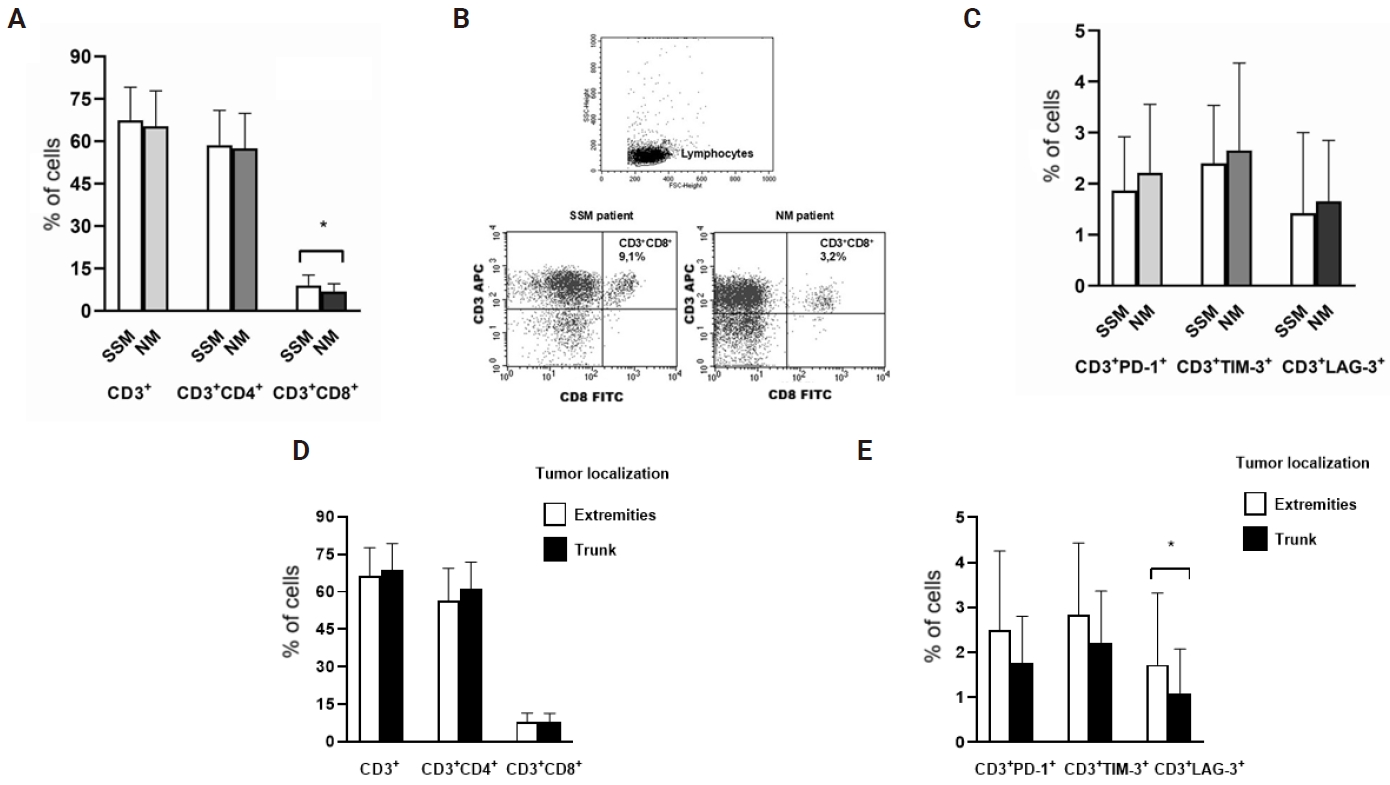
- Making a comparison in immune cells in SLNs between melanoma patients with two different histologic subtypes, we have found that patients with nodular melanoma (NM) (n = 21) had statistically significant decrease (p ≤ .05, Mann-Whitney exact test) in the percentage of cytotoxic CD3+CD8+ T cells compared with the percentage of these cells in the patients with superficial spreading melanoma (SSM) (n = 38) (Fig. 6A, B). Additionally, analyzing the expression of PD-1, TIM-3, and LAG-3 molecules on CD3+ T cells in SLN tissues of SSM and NM patients, we found no statistically significant difference (p > .5, Mann-Whitney exact test) in the expression of all analyzed inhibitory molecules between these two histologic subtypes of melanoma patients. However, there was a trend of increased expression of PD-1, TIM-3, as well as LAG-3 on CD3+ T cells in NM patients (Fig. 6C). Additionally, we analyzed the percentage of immune cells in SLNs in cutaneous melanoma patients with primary localization of tumor on extremities and trunk and found no statistically significant difference (p > .5, Mann-Whitney exact test) in the percentage of CD3+, cytotoxic CD3+CD8+ and helper CD3+CD4+ T cells between these two different tumor localizations (Fig. 6D). However, analyzing the expression of PD-1, TIM-3, and LAG-3 molecules on CD3+ T cells in SLNs, we found statistically significant increase (p ≤ .05, Mann-Whitney exact test) of LAG-3 inhibitory molecule in patients with primary melanoma localization on extremities. Additionally, there was a trend of increased expression of PD-1 and TIM-3 on CD3+ cells in these patients (Fig. 6E).
RESULTS
- Although it is well-known that melanoma cells spread rapidly to distant sites through both hematologic and lymphatic pathways, SLN is almost always the first site of melanoma metastasis. At the beginning of this process, the cells of primary tumor secrete various immunosuppressive soluble mediators [5], as well as extracellular vesicles (EVs) [13] that are transported through afferent lymphatic vessels to SLN. These factors are able to suppress anti-tumor immune response and induce remodeling and lymphangiogenesis in SLNs [6]. These processes occur before the arrival of the first metastatic cells in SLN and they have the role in the maintenance of PMN that helps in the colonization of metastatic cells in SLN [14].
- In this study we have shown that melanoma patients with worse prognosis in stage II, and especially with thicker melanoma and the presence of ulceration (stage IIB and IIC) had statistically significant decrease in the percentage of total CD3+ and cytotoxic CD3+CD8+ T cells compared with the patients in stage I melanoma, a less aggressive stadium of the cancer disease with a lower risk of spreading. Grotz et al. [15] found fewer CTLs in SLN compared with the percentage of these cells in non-SLN and healthy LN of melanoma patients with cutaneous melanoma. Total CD3+, especially CD8+ lymphocytes, exhibit cytotoxic properties, promoting the removal of cancer cells indirectly by cytokines production (IFN-γ and tumor necrosis factor α), as well as directly through the secretion of cytotoxic proteins, perforin, and granzymes [16]. Soluble mediators such as TGF-β, IL-6, IL-10, and VEGF produced in immunosuppressive microenvironment of primary tumor in stage II melanoma patients are transported to SLN and induce impairment of the functions of CD8+ cytotoxic T cells [17]. Our group found increased serum level of the immunosuppressive cytokine TGF-β1 in melanoma patients in stage IIB and IIC compared with the patients in stage IA and IB [18]. It is known that TGF-β suppresses the synthesis of perforin and granzymes, and also inhibits the ERK pathway, which is important for T-cell proliferation and cytokine production that leads to a loss of immune surveillance against melanoma [19]. In accordance with this knowledge, in this study, we found a trend of decreased expression of IFN-γ in CD3+ T cells in SLN of melanoma patients in stage II compared with patients in stage I. IFN-γ has the ability to inhibit tumor cell growth and metastasis directly through apoptosis and cell cycle arrest, as well as indirectly by the activation of anti-tumor immune cells, CTLs, NK cells, and M1 macrophages [20]. Furthermore, EVs are associated with the loss of CTLs and impairment of their effector functions through high expression of the inhibitory PD-L1 molecule on their surface [21]. Therefore, melanoma patients in clinical stage II with a lower percentage of CD3+ and CTL CD8+ T lymphocytes and decreased IFN-γ production in still intact SLNs are at greater risk for tumor cell metastasis. Furthermore, although helper CD4+ T cells [22] and especially NK cells [23] play a significant role in anti-tumor immune response, in this study, we did not find any difference in the percentage of these cells in SLNs between melanoma patients in stage I and stage II. Some authors have shown diminished NK cells but only in melanoma-bearing SLNs [24].
- The binding of T-cell inhibitory checkpoint molecules, PD-1, TIM-3, and LAG-3 to their ligands on tumor cells, as well as on numerous immunosuppressive cells in TME leads to T-cell dysfunction and exhaustion [25]. Also, it is known that PD-1–mediated T-cell failures begin early in melanoma progression [26]. Increased expression of PD-1 on T cells in SLN of stage II melanoma patients found in this study may suggest impairment in T-cell activation and function. Grotz et al. [15] showed increased expression of PD-1 on CD3+ T cells in SLN, as well as in non-SLN of cutaneous melanoma patients, compared with healthy LN [15]. Therefore, their SLNs develop an immune-tolerant microenvironment with altered immune cell profiles. Additionally, we show for the first time that melanoma patients in stage IIB and IIC, besides high expression of PD-1, had significantly increased expression of the other inhibitory molecule, TIM-3 on CD3+ T cells compared with the patients in stage I and IIA. TIM-3 is expressed on Th1, Th17, and CD8 T cells and by binding the ligands, galectin-9, phosphatidylserine, HMGB1, and CEACAM1, inhibits immune response of these T cells [27]. In physiological conditions, TIM-3 has a role in the maintenance of peripheral tolerance [28]. However, recent studies have shown an important role of TIM-3 molecule in T-cell exhaustion in cancer as TIM-3–expressing CD4+ and CD8+ T cells have impaired effector functions, are less proliferative in response to tumor antigens, and produce reduced amounts of cytokines that leads to failure in immunosurveillance [29]. Therefore, TIM-3 could become a promising target for cancer immunotherapy [30]. CD3+ T cells with increased expression of both inhibitory molecules, PD-1 and TIM-3, found in this study in patients with worse prognosis in stage IIB and IIC, could exhibit severe exhausted function as seen by their failure in IFN-γ production. This suggests that these two molecules and their pathways work synergistically in establishing T-cell inhibition [31]. Therefore, the therapeutic blockade of both TIM-3 and PD-1 pathways might be very effective in controlling tumor growth and could restore anti-tumor immunity in cutaneous melanoma patients especially in stage IIB and IIC [32,33]. However, there was no difference in the expression of all analyzed inhibitory molecules, PD-1, TIM-3, and LAG-3 on CD3+ T cells in SLNs of melanoma patients in stage IIB, IIC, as well as in stage III. Yaddanapudi et al. [24] have shown that the patients with melanoma-positive SLNs had increased PD-1 expression on T cells. As we have only six patients in stage III with melanoma-positive SLNs in this research, additional investigations are necessary. Based on the results of this study, we could not determine exactly which patients in stage IIB and IIC would be the best candidates for the treatment with immune checkpoint inhibitors. In future research, more patients are needed for this analysis although FDA now provides this therapy to all patients in stage IIB and IIC for 12 months [10].
- In physiological conditions, Treg cells have the role to establish the tolerance to self-antigens, while in cancer patients, they suppress immune responses against tumor-associated antigens [34]. In this study, melanoma patients in stage IIB and IIC had significantly higher percentage of Foxp3+ and CD4+ Foxp3+ Treg cells in SLNs compared with the percentage of these cells in patients in stage I and IIA. The presence of high number of FoxP3+ Tregs in SLNs of these melanoma patients can indicate an immunosuppressive TME, which is a known factor in promoting cancer progression and can be associated with the development of metastasis in cutaneous melanoma patients with worse prognosis [35]. Gupta et al. [36] have shown a significant association between the number of FoxP3+ cells in SLNs and the size of primary breast invasive ductal carcinoma. Furthermore, Viguier et al. [37] have found that CD4+CD25high Treg cells were overrepresented in metastatic lymph nodes compared with both tumor-free LNs and autologous peripheral blood mononuclear cells. Tregs by the production of immunosuppressive cytokines, TGF-β, IL-10, and IL-35 or directly by cell-to-cell contact could decrease the percentage of total CD3+ and CD3+CD8+ CTLs, IFN-γ expression in CD3+ T cells, and could increase the expression of inhibitory PD-1 and TIM-3 molecules [38,39] that are found in stage IIB and IIC melanoma patients in this study. Also, these cells express high levels of enzymes, CD39 and CD73, that have the role to convert extracellular ATP into adenosine. The extracellular adenosine binds to A2A and A2B receptors on the surface of effector T cells and impairs their proliferation, cytokines production, and cytotoxic anti-tumor activities [40]. All of these immunosuppressive mechanisms allow tumor cells to escape immune surveillance but also contribute to resistance to cancer immunotherapy.
- In this study, we found the negative correlation between primary tumor depth in millimeters (Breslow) and the percentage of total CD3+, as well as CD3+CD8+ T cells in SLNs of all investigated melanoma patients. Furthermore, a positive correlation between Breslow thickness and the percentage of CD3+PD-1+ T lymphocytes was found. This result is in accord with the results of Yaddanapudi et al. [24] of positive correlation between Breslow thickness and frequency of immunosuppressive CD8+CD57+PD-1+ cells in SLNs of melanoma patients in stages I, II, and III. In addition to tumor thickness, ulceration of primary melanoma represents a critical, independent poor prognostic factor [10]. It has been shown that ulcerated melanoma had high density of macrophages and DCs that together with tumor cells produce immunosuppressive IL-6 [41]. High IL-6 could be associated with decreased percentage of antitumor CD3+ and CD3+CD8+ T cells, as well as increased percentage of CD3+PD-1+ cells found in this study for melanoma patients with ulcerated tumors. These results confirm once more that patients with thicker and ulcerated melanoma with worse prognosis have lower percentage of antitumor cells, as well as increased percentage of functional exhausted CD3+ T cells with high PD-1 expression in their SLNs. Furthermore, it is known that the presence of tumor-infiltrating lymphocytes (TILs) in primary melanoma is protective factor for lymph node metastasis [42,43]. However, in our study, we did not find any difference in the percentage of T-cell subsets and the expression of inhibitory checkpoint molecules, PD-1, TIM-3, and LAG-3, on CD3+ T cells between melanoma patients with focal (non-brisk) and dense (brisk) infiltrate in primary tumors. As we do not have the data in medical documentation for 10 melanoma patients regarding lymphocyte infiltration, additional investigations are needed.
- Cutaneous melanoma is a heterogeneous cancer that consists of various histologic subtypes among which the most common are SSM (70% of the patients) and NM (20%) [44]. It is important to determine the histologic subtype of melanoma, as it has a prognostic significance for patients. It is known that the tumors of patients with NM have a higher Breslow thickness, more frequent ulcerations, higher dermal mitotic rate, and more frequent satellite lesions [45]. Therefore, NM patients have a more aggressive clinical course of disease with higher rates of recurrence and metastasis compared with patients with SSM subtype [46,47]. Furthermore, molecular analyses show the differences between SSM and NM subtypes. It is known that NM patients contain a lower mutational load compared with SSM [48], as well as decreased presence of TILs [49] and an upregulation of PD-L1 expression on tumor cells [50]. In this study, we have shown for the first time statistically significant decrease in the percentage of cytotoxic CD3+CD8+ T cells in SLNs of patients with NM compared with SSM patients. Furthermore, we have found that the patients with NM had a trend of increased expression of PD-1, TIM-3, as well as LAG-3 inhibitory molecules on their CD3+ cells. These data suggest a weaker response and evasion of immune system in SLN of NM patients compared with SSM. These differences in immune characteristics of melanoma histologic subtypes contribute to more aggressive nature of NM subtype. It is known that immunotherapy is more effective in melanoma subtypes with a higher mutation rate and TIL presence [51]. However, it is unclear whether the patients with NM have a lower efficiency of immunotherapy compared with SSM. Lattanzi et al. [52] observed no difference in survival outcomes of NM versus SSM patients treated with immunotherapy (anti–PD-1, anti–CTLA-4 mAbs), while Pala et al. [53] displayed an improved survival of NM patients treated with immunotherapy compared with SSM patients. However, we would probably find more statistically significant differences in the analyzed parameters between SSM and NM patients if there were not even 14 patients for whom we do not have data regarding the histopathological type of their primary tumors in medical documentation. For that reason, we did not include these 14 patients and one patient with acral lentiginous melanoma in the statistical analysis. Furthermore, there are no data in the literature regarding the association between the functional and immunophenotypical characteristics of T cells in SLNs and different localizations of primary melanoma. In this study, we have found for the first time increased expression of inhibitory checkpoint molecules, especially LAG-3, on CD3+ T cells in non-malignant SLNs of melanoma patients with localization of tumor on extremities. According to these results, TME in SLNs of these patients could be immunosuppressive. On the other hand, no difference was found in the percentage of T cell subsets between patients with localization of melanoma on extremities and trunk. Fadaki et al. [54] showed a statistically significant SLN-positive rate for melanoma patients with trunk localization compared with localization on extremities. However, more research is needed to fully understand the distinct biological mechanisms and potential therapeutic differences between different melanoma histological subtypes and localizations.
- Our results have shown a lower percentage of total CD3+ and CD3+CD8+ T lymphocytes, some lower IFN-γ expression in CD3+ T cells, as well as their higher expression of inhibitory PD-1 and TIM-3 molecules in melanoma patients with thicker ulcerated melanoma and worse prognosis in stage IIB and IIC. This functional exhaustion of T lymphocytes could be associated with a higher percentage of immunosuppressive Treg cells found in this research in these patients. These immunological alterations could cause progressive immune dysfunction in SLNs before the appearance of tumor cells in them. The mechanisms of these changes are very complex and multifactorial and further investigations are necessary to elucidate them in more detail. Therefore, immunosuppressive soluble mediators, cells, and signaling pathways in PMN of SLN might be targeted to inhibit the formation of PMN, repair antitumor immune response and prevent the occurrence of metastasis in SLN. This study provides the new results of the impairment of immune response in SLN of high-risk cutaneous melanoma patients, prior to lymphogenous metastasis and could help in understanding the need to introduce the new immunotherapies that could revive immune response and prevent melanoma metastasis in SLN. However, as the sample size of different clinical stages of melanoma patients analyzed in this study is relatively small, additional investigations and more patients are needed to improve this research.
DISCUSSION
Ethics Statement
All procedures performed in this study were approved by the Ethics Committee of Institute of Oncology and Radiology of Serbia (No. 14/2024/1081, date: April 3, 2024) in accordance with the 1964 Helsinki declaration and its later amendments. Informed consent was obtained from all individual participants included in the study.
Availability of Data and Material
All data generated or analyzed during the study are included in this published article. Any further information related to this study can be obtained by contacting the authors.
Code Availability
Not applicable.
Author Contributions
Conceptualization: EF, KMM, OŽ, NMM, AL, ZB, MJ, MŽ. Data curation: EF, KMM, ZB, MJ, MŽ. Formal analysis: ZB. Investigation: EF, KMM, MŽ. Methodology: EF, KMM, OŽ, NMM, AL, MŽ. Supervision: KMM, MŽ. Validation: OŽ, NMM, AL. Writing—original draft: EF, KMM, MŽ. Writing—review & editing: OŽ, NMM, AL, ZB, MJ. Approval of final manuscript: all authors.
Conflicts of Interest
The authors declare that they have no potential conflicts of interest.
Funding Statement
This work was supported by Ministry of Science, Technological Development and Innovation of the Republic of Serbia (Agreement No. 451-03-33/2026-03/200043).
Acknowledgments
We wish to thank Mrs. Jasna Popović Basić for excellent technical work.
- 1. Waseh S, Lee JB. Advances in melanoma: epidemiology, diagnosis, and prognosis. Front Med (Lausanne) 2023; 10: 1268479.ArticlePubMedPMC
- 2. du Bois H, Heim TA, Lund AW. Tumor-draining lymph nodes: at the crossroads of metastasis and immunity. Sci Immunol 2021; 6: eabg3551. ArticlePubMedPMC
- 3. Faries MB. Sentinel lymph nodes in melanoma: necessary as ever for optimal treatment. Clin Exp Metastasis 2024; 41: 369-74. ArticlePubMedPMCPDF
- 4. Delclaux I, Ventre KS, Jones D, Lund AW. The tumor-draining lymph node as a reservoir for systemic immune surveillance. Trends Cancer 2024; 10: 28-37. ArticlePubMedPMC
- 5. Patras L, Shaashua L, Matei I, Lyden D. Immune determinants of the pre-metastatic niche. Cancer Cell 2023; 41: 546-72. ArticlePubMedPMC
- 6. Suman S, Markovic SN. Melanoma-derived mediators can foster the premetastatic niche: crossroad to lymphatic metastasis. Trends Immunol 2023; 44: 724-43. ArticlePubMedPMC
- 7. Cochran AJ, Morton DL, Stern S, Lana AM, Essner R, Wen DR. Sentinel lymph nodes show profound downregulation of antigen-presenting cells of the paracortex: implications for tumor biology and treatment. Mod Pathol 2001; 14: 604-8. ArticlePubMedPDF
- 8. Wang Y, Jia J, Wang F, et al. Pre-metastatic niche: formation, characteristics and therapeutic implication. Signal Transduct Target Ther 2024; 9: 236.ArticlePubMedPMCPDF
- 9. Sabbatino F, Liguori L, Pepe S, Ferrone S. Immune checkpoint inhibitors for the treatment of melanoma. Expert Opin Biol Ther 2022; 22: 563-76. ArticlePubMedPMC
- 10. Amaral T, Ottaviano M, Arance A, et al. Cutaneous melanoma: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol 2025; 36: 10-30. ArticlePubMed
- 11. Amin MB, Greene FL, Edge SB, et al. The eighth edition AJCC cancer staging manual: continuing to build a bridge from a population-based to a more "personalized" approach to cancer staging. CA Cancer J Clin 2017; 67: 93-9. ArticlePubMed
- 12. Jackson AL, Warner NL. Preparation, staining and analysis by flow cytometry of peripheral blood leukocytes. In: Rose NR, Friedman H, Fahey JL, eds. Manual of clinical laboratory immunology. 3rd ed. Washington, DC: American Society for Microbiology, 1986; 274-81.
- 13. Kiya Y, Yoshioka Y, Nagakawa Y, Ochiya T. Extracellular vesicles are important mediators that regulate tumor lymph node metastasis via the immune system. Int J Mol Sci 2023; 24: 1362.ArticlePubMedPMC
- 14. Gillot L, Baudin L, Rouaud L, Kridelka F, Noel A. The pre-metastatic niche in lymph nodes: formation and characteristics. Cell Mol Life Sci 2021; 78: 5987-6002. ArticlePubMedPMCPDF
- 15. Grotz TE, Jakub JW, Mansfield AS, et al. Evidence of Th2 polarization of the sentinel lymph node (SLN) in melanoma. Oncoimmunology 2015; 4: e1026504. ArticlePubMedPMC
- 16. Bida M, Miya TV, Hull R, Dlamini Z. Tumor-infiltrating lymphocytes in melanoma: from prognostic assessment to therapeutic applications. Front Immunol 2024; 15: 1497522.ArticlePubMedPMC
- 17. Maus RL, Leontovich AA, Moore RM, et al. Quantitative spatial evaluation of tumor-immune interactions in the immunotherapy setting of metastatic melanoma lymph nodes. Front Immunol 2022; 13: 1024039.ArticlePubMedPMC
- 18. Martinovic KM, Milicevic M, Larsen AK, et al. Effect of cytokines on NK cell activity and activating receptor expression in high-risk cutaneous melanoma patients. Eur Cytokine Netw 2019; 30: 160-7. ArticlePubMedPDF
- 19. Dahmani A, Delisle JS. TGF-β in T cell biology: implications for cancer immunotherapy. Cancers (Basel) 2018; 10: 194.ArticlePubMedPMC
- 20. Jorgovanovic D, Song M, Wang L, Zhang Y. Roles of IFN-γ in tumor progression and regression: a review. Biomark Res 2020; 8: 49.ArticlePubMedPMCPDF
- 21. Kielbowski K, Plewa P, Szulc J, Cmil M, Bakinowska E, Pawlik A. Extracellular vesicles and PD-L1: a review of complex immunoregulatory properties and clinical importance. Biomedicines 2025; 13: 1356.ArticlePubMedPMC
- 22. Tay RE, Richardson EK, Toh HC. Revisiting the role of CD4+ T cells in cancer immunotherapy: new insights into old paradigms. Cancer Gene Ther 2021; 28: 5-17. ArticlePubMedPMCPDF
- 23. Coenon L, Geindreau M, Ghiringhelli F, Villalba M, Bruchard M. Natural killer cells at the frontline in the fight against cancer. Cell Death Dis 2024; 15: 614.ArticlePubMedPMC
- 24. Yaddanapudi K, Stamp BF, Subrahmanyam PB, et al. Single-cell immune mapping of melanoma sentinel lymph nodes reveals an actionable immunotolerant microenvironment. Clin Cancer Res 2022; 28: 2069-81. ArticlePubMedPMCPDF
- 25. Zhong T, Sun S, Zhao M, Zhang B, Xiong H. The mechanisms and clinical significance of CD8+ T cell exhaustion in anti-tumor immunity. Cancer Biol Med 2025; 22: 460-80. ArticlePubMedPMC
- 26. Hino R, Kabashima K, Kato Y, et al. Tumor cell expression of programmed cell death-1 ligand 1 is a prognostic factor for malignant melanoma. Cancer 2010; 116: 1757-66. ArticlePubMed
- 27. Zhu C, Anderson AC, Schubart A, et al. The Tim-3 ligand galectin-9 negatively regulates T helper type 1 immunity. Nat Immunol 2005; 6: 1245-52. ArticlePubMedPDF
- 28. Sabatos CA, Chakravarti S, Cha E, et al. Interaction of Tim-3 and Tim-3 ligand regulates T helper type 1 responses and induction of peripheral tolerance. Nat Immunol 2003; 4: 1102-10. ArticlePubMedPDF
- 29. Das M, Zhu C, Kuchroo VK. Tim-3 and its role in regulating anti-tumor immunity. Immunol Rev 2017; 276: 97-111. ArticlePubMedPMCPDF
- 30. Sauer N, Janicka N, Szlasa W, et al. TIM-3 as a promising target for cancer immunotherapy in a wide range of tumors. Cancer Immunol Immunother 2023; 72: 3405-25. ArticlePubMedPMCPDF
- 31. Fourcade J, Sun Z, Benallaoua M, et al. Upregulation of Tim-3 and PD-1 expression is associated with tumor antigen-specific CD8+ T cell dysfunction in melanoma patients. J Exp Med 2010; 207: 2175-86. ArticlePubMedPMCPDF
- 32. Sakuishi K, Apetoh L, Sullivan JM, Blazar BR, Kuchroo VK, Anderson AC. Targeting Tim-3 and PD-1 pathways to reverse T cell exhaustion and restore anti-tumor immunity. J Exp Med 2010; 207: 2187-94. ArticlePubMedPMCPDF
- 33. Guo CX, Huang X, Xu J, et al. Combined targeted therapy and immunotherapy for cancer treatment. World J Clin Cases 2021; 9: 7643-52. ArticlePubMedPMC
- 34. Sakaguchi S, Yamaguchi T, Nomura T, Ono M. Regulatory T cells and immune tolerance. Cell 2008; 133: 775-87. ArticlePubMedPMC
- 35. Nishikawa H, Sakaguchi S. Regulatory T cells in tumor immunity. Int J Cancer 2010; 127: 759-67. ArticlePubMed
- 36. Gupta R, Babb JS, Singh B, et al. The numbers of FoxP3+ lymphocytes in sentinel lymph nodes of breast cancer patients correlate with primary tumor size but not nodal status. Cancer Invest 2011; 29: 419-25. ArticlePubMedPMC
- 37. Viguier M, Lemaitre F, Verola O, et al. Foxp3 expressing CD4+CD25(high) regulatory T cells are overrepresented in human metastatic melanoma lymph nodes and inhibit the function of infiltrating T cells. J Immunol 2004; 173: 1444-53. ArticlePubMedPDF
- 38. Schmidt A, Oberle N, Krammer PH. Molecular mechanisms of Treg-mediated T cell suppression. Front Immunol 2012; 3: 51.ArticlePubMedPMC
- 39. Ma R, Sun JH, Wang YY. The role of transforming growth factor-β (TGF-β) in the formation of exhausted CD8 + T cells. Clin Exp Med 2024; 24: 128.ArticlePubMedPMCPDF
- 40. Kaplinsky N, Williams K, Watkins D, Adams M, Stanbery L, Nemunaitis J. Regulatory role of CD39 and CD73 in tumor immunity. Future Oncol 2024; 20: 1367-80. ArticlePubMedPMC
- 41. Barricklow Z, DiVincenzo MJ, Angell CD, Carson WE. Ulcerated cutaneous melanoma: a review of the clinical, histologic, and molecular features associated with a clinically aggressive histologic phenotype. Clin Cosmet Investig Dermatol 2022; 15: 1743-57. ArticlePubMedPMCPDF
- 42. Taylor RC, Patel A, Panageas KS, Busam KJ, Brady MS. Tumor-infiltrating lymphocytes predict sentinel lymph node positivity in patients with cutaneous melanoma. J Clin Oncol 2007; 25: 869-75. ArticlePubMed
- 43. Duprat JP, Brechtbulh ER, Costa de Sa B, et al. Absence of tumor-infiltrating lymphocyte is a reproducible predictive factor for sentinel lymph node metastasis: a multicenter database study by the Brazilian melanoma group. PLoS One 2016; 11: e0148160. ArticlePubMedPMC
- 44. Duncan LM. The classification of cutaneous melanoma. Hematol Oncol Clin North Am 2009; 23: 501-13. ArticlePubMed
- 45. Greenwald HS, Friedman EB, Osman I. Superficial spreading and nodular melanoma are distinct biological entities: a challenge to the linear progression model. Melanoma Res 2012; 22: 1-8. ArticlePubMedPMC
- 46. Green AC, Viros A, Hughes MC, et al. Nodular melanoma: a histopathologic entity? Acta Derm Venereol 2018; 98: 460-2. ArticlePubMed
- 47. Allais BS, Beatson M, Wang H, et al. Five-year survival in patients with nodular and superficial spreading melanomas in the US population. J Am Acad Dermatol 2021; 84: 1015-22. ArticlePubMed
- 48. Druskovich C, Kelley J, Aubrey J, Palladino L, Wright GP. A review of melanoma subtypes: genetic and treatment considerations. J Surg Oncol 2025; 131: 356-64. ArticlePubMedPMC
- 49. Lin RL, Wang TJ, Joyce CJ, et al. Decreased tumor-infiltrating lymphocytes in nodular melanomas compared with matched superficial spreading melanomas. Melanoma Res 2016; 26: 524-7. ArticlePubMed
- 50. Giavina-Bianchi M, Giavina-Bianchi P, Sotto MN, et al. Nodular primary cutaneous melanoma is associated with PD-L1 expression. Eur J Dermatol 2020; 30: 352-7. ArticlePubMed
- 51. Timis T, Buruiana S, Dima D, et al. Advances in cell and immune therapies for melanoma. Biomedicines 2025; 13: 98.ArticlePubMedPMC
- 52. Lattanzi M, Lee Y, Simpson D, et al. Primary melanoma histologic subtype: impact on survival and response to therapy. J Natl Cancer Inst 2019; 111: 180-8. ArticlePubMedPMCPDF
- 53. Pala L, Conforti F, Pagan E, et al. Different response to immunotherapy according to melanoma histologic subtype. J Immunother 2022; 45: 119-24. ArticlePubMed
- 54. Fadaki N, Li R, Parrett B, et al. Is head and neck melanoma different from trunk and extremity melanomas with respect to sentinel lymph node status and clinical outcome? Ann Surg Oncol 2013; 20: 3089-97. ArticlePubMedPDF
REFERENCES
Figure & Data
References
Citations
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-
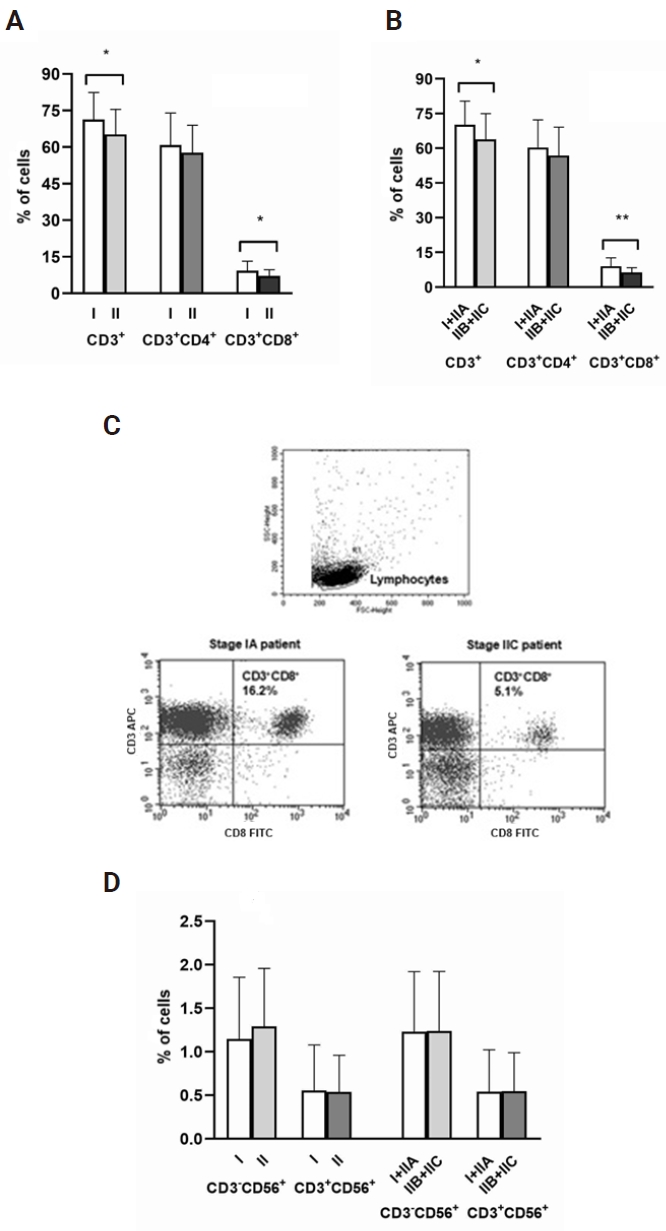
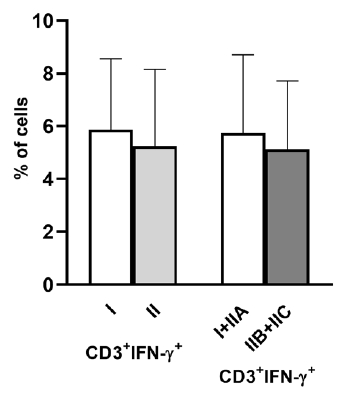
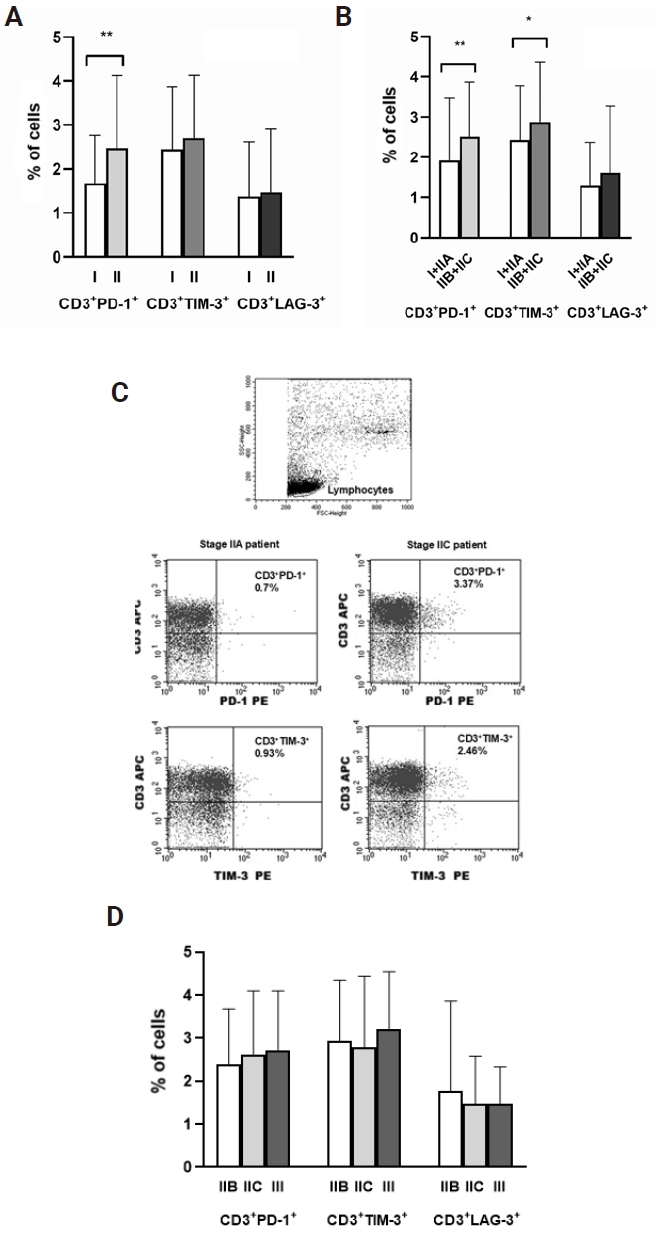
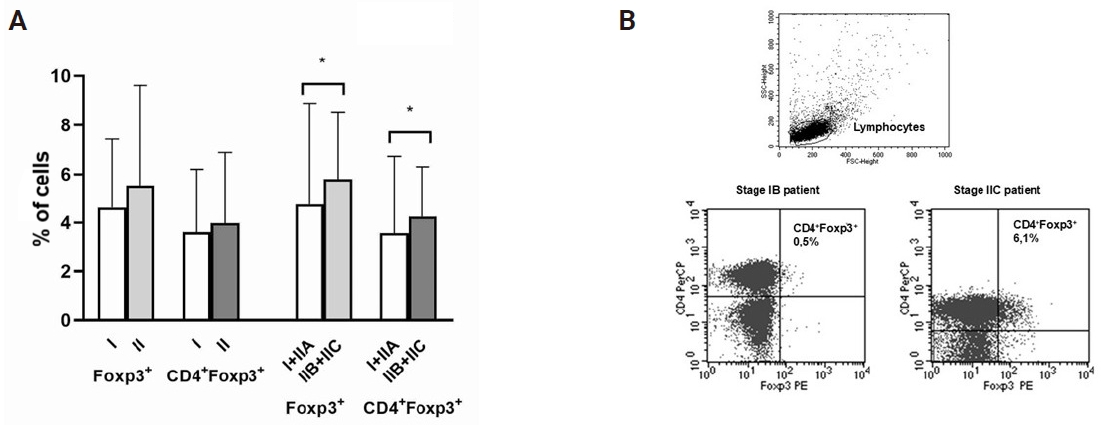
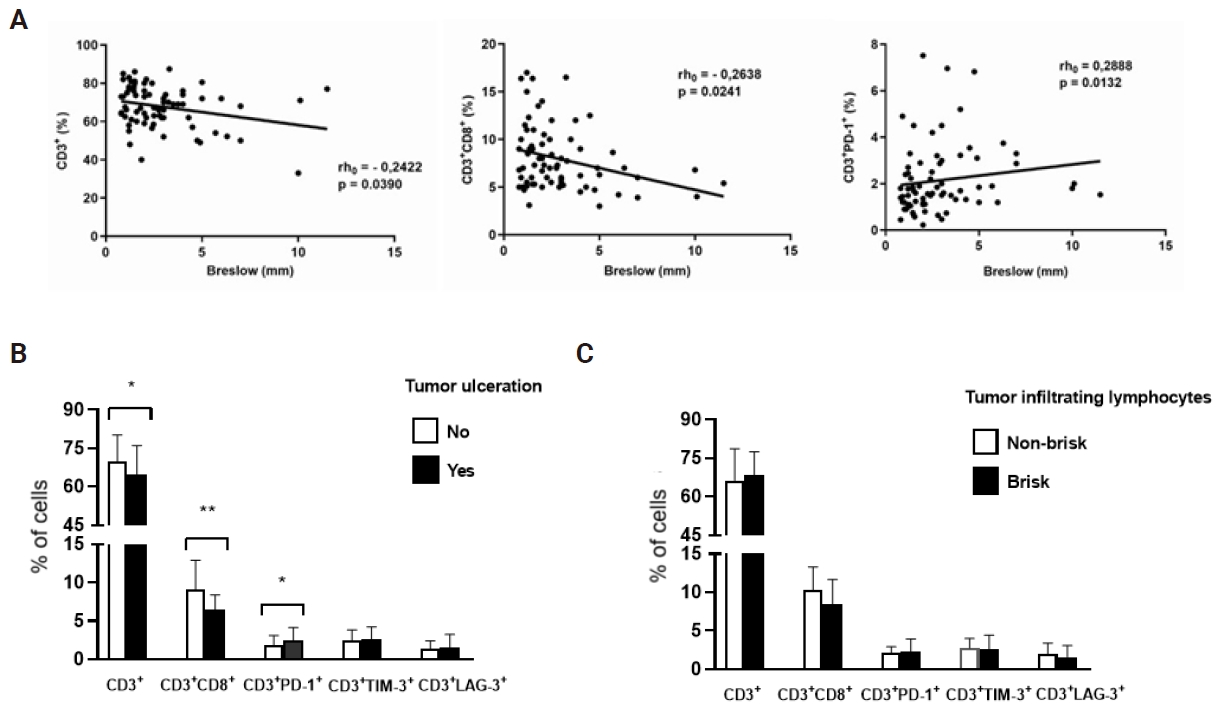
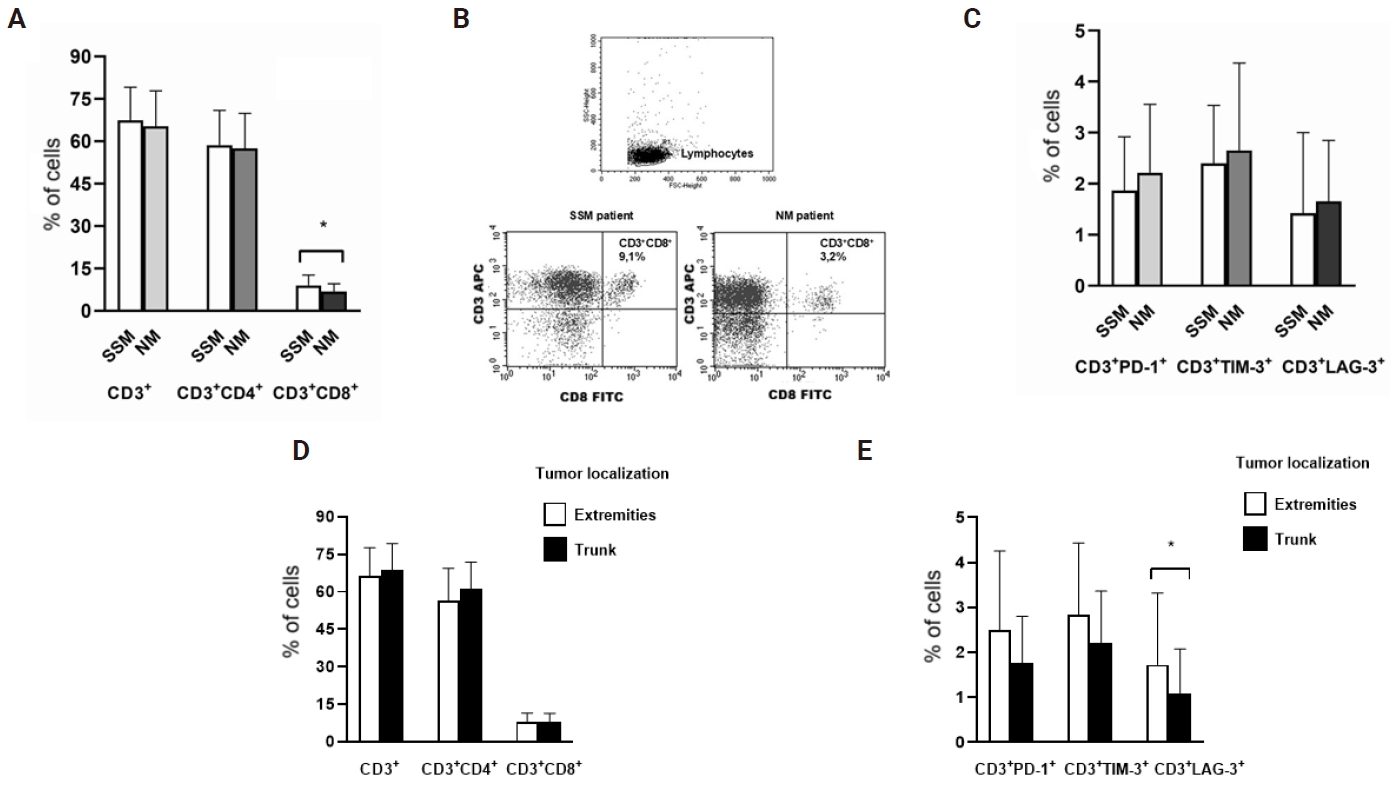
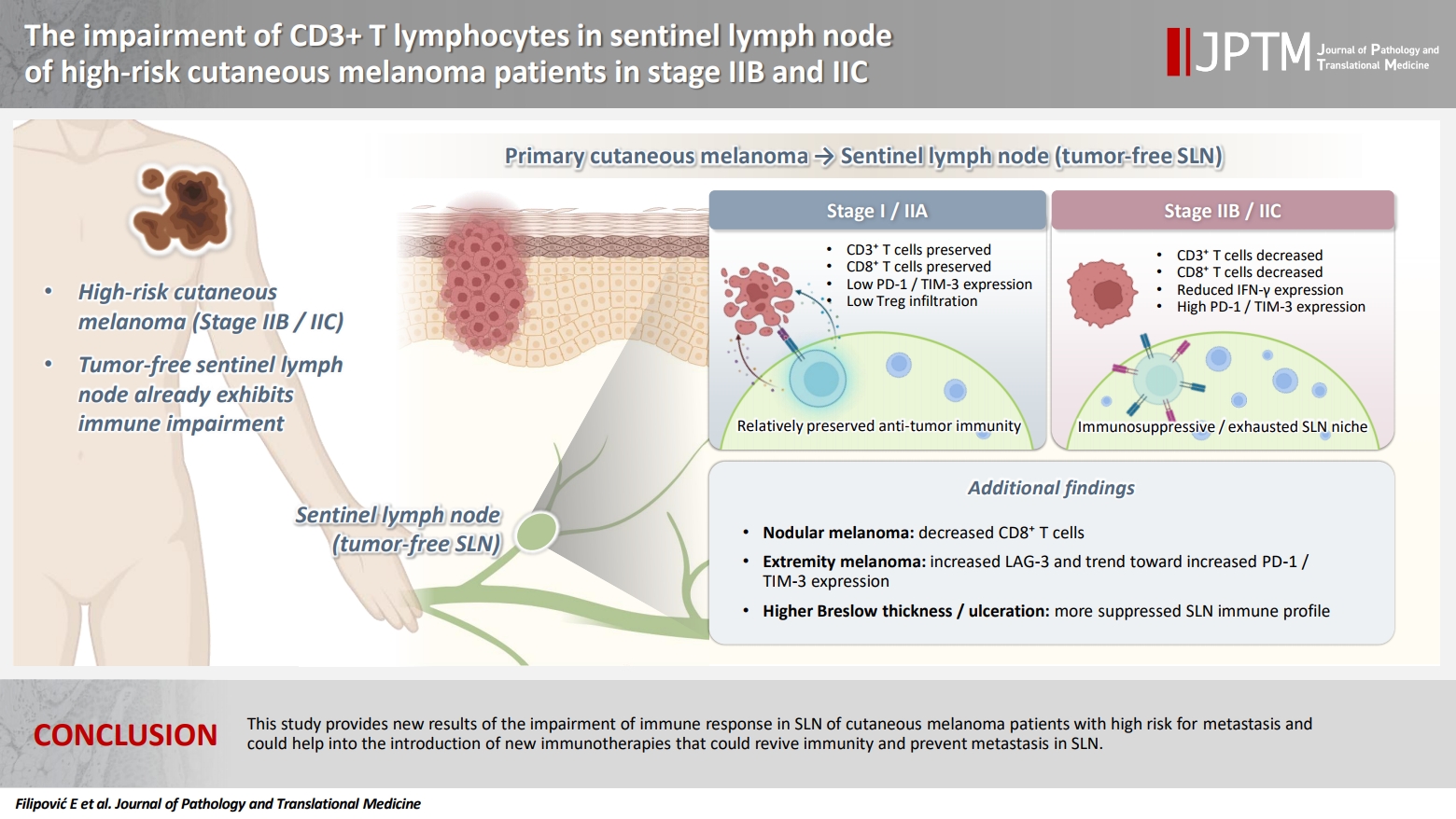
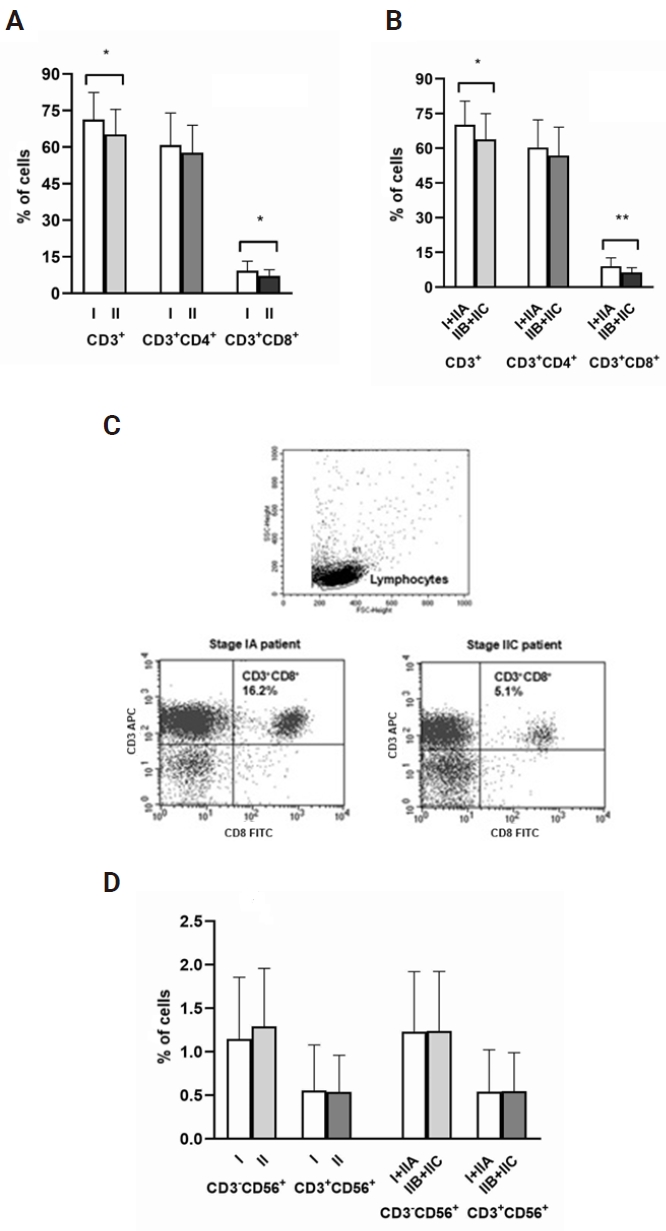
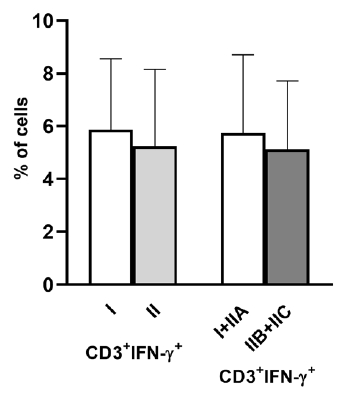
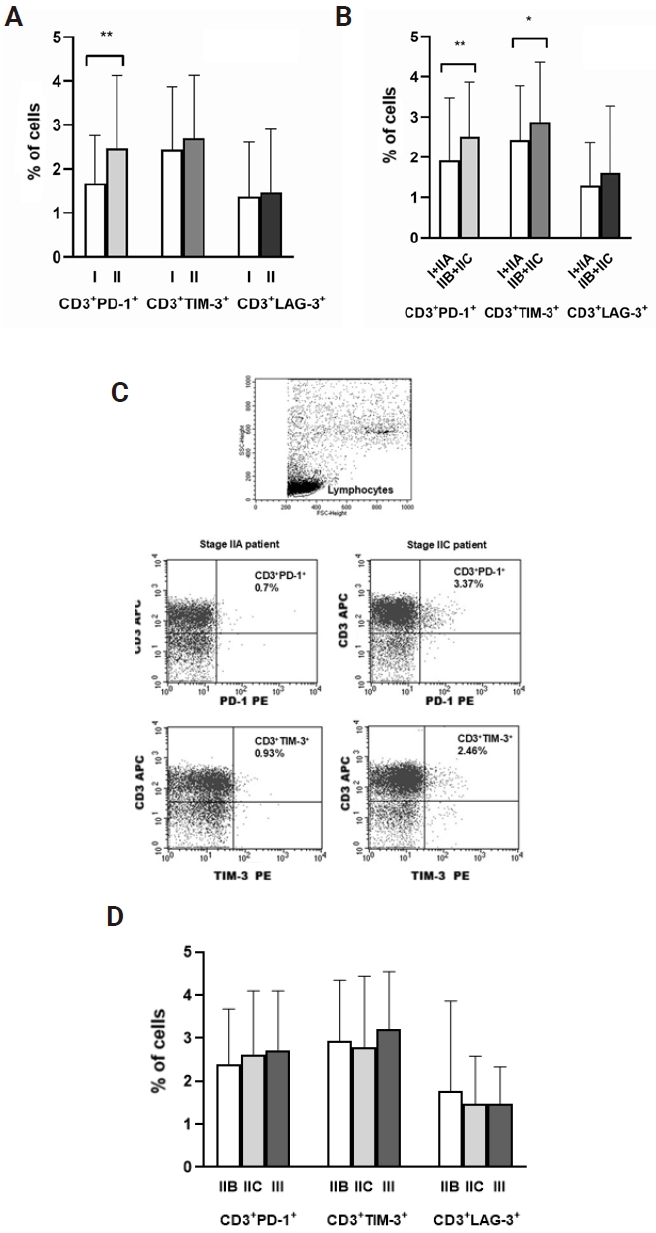
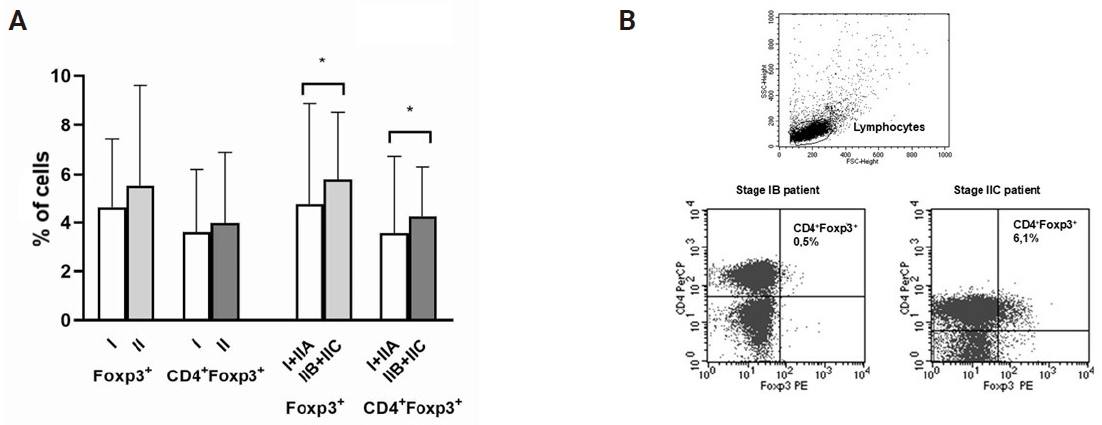
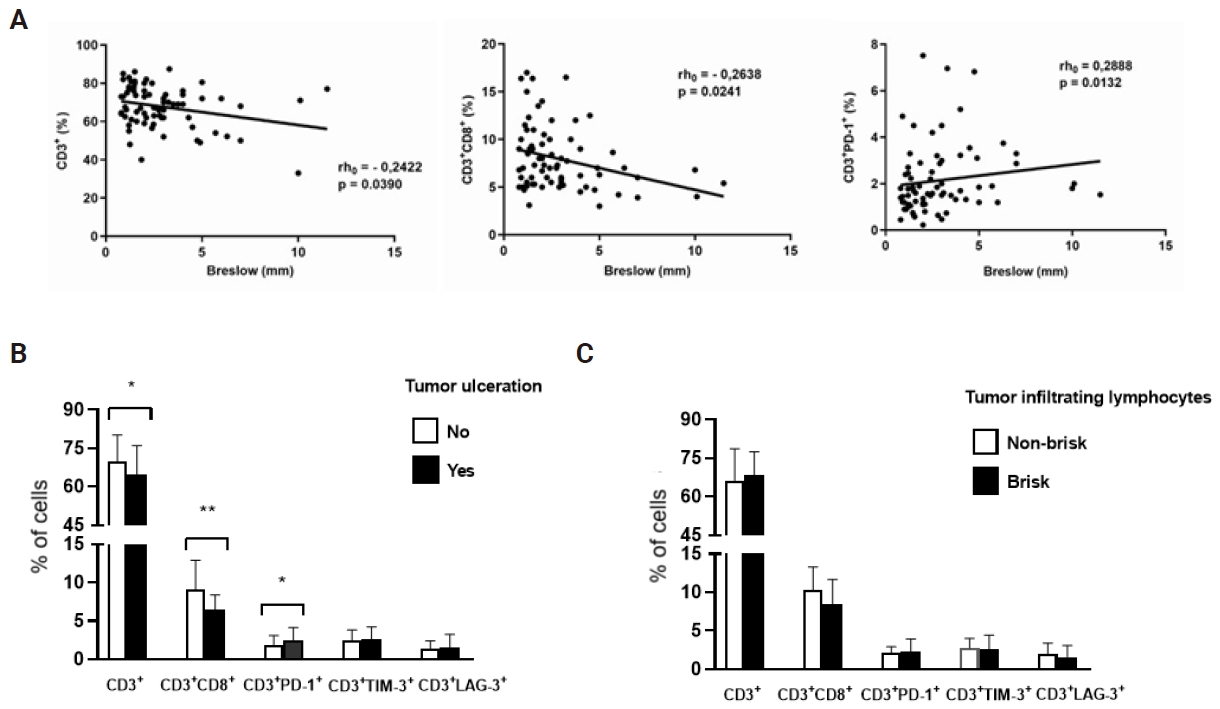
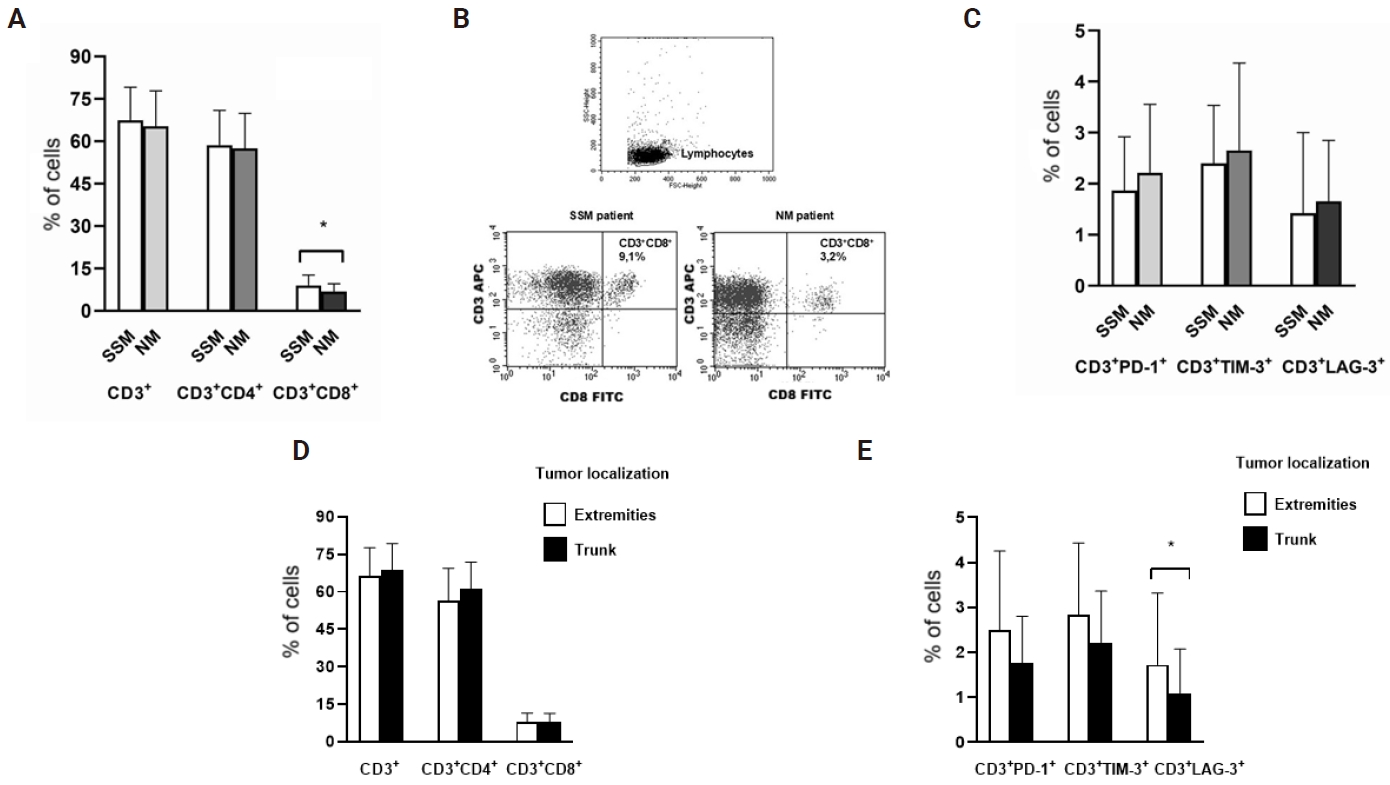

Fig. 1.
Fig. 2.
Fig. 3.
Fig. 4.
Fig. 5.
Fig. 6.
Graphical abstract
| Characteristics of patients in stage I and II | No. (%) |
|---|---|
| Sex | |
| Male | 42 (56.8) |
| Female | 32 (43.2) |
| Age (yr) | |
| Mean±SD | 61.0 ± 14.6 |
| Median (range) | 66 (21–88) |
| Stage of disease | |
| I | 30 (40.5) |
| IIA | 15 (20.3) |
| IIB | 15 (20.3) |
| IIC | 14 (18.9) |
| Tumor characteristics | |
| Breslow | |
| ≤ 2 mm | 35 (47.3) |
| > 2 mm | 39 (52.7) |
| Ulceration | |
| No | 43 (58.1) |
| Yes | 31 (41.9) |
| Tumor infiltrating lymphocytes | |
| Non-brisk | 23 (31.1) |
| Brisk | 41 (55.4) |
| Unknown | 10 (13.5) |
| Histologic subtypes | |
| SSM | 38 (51.3) |
| NM | 21 (28.4) |
| ALM | 1 (1.3) |
| Unknown | 14 (19.0) |
| Localization | |
| Extremities | 37 (50.0) |
| Trunk | 36 (48.6) |
| Head | 1 (1.4) |
| Total | 74 (100) |
SD, standard deviation; SSM, superficial spreading melanoma; NM, nodular melanoma; ALM, acral lentiginous melanoma.

