 E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 48(3); 2014 > Article
-
Original Article
Classic Papillary Thyroid Carcinoma with Tall Cell Features and Tall Cell Variant Have Similar Clinicopathologic Features - Woo Jin Oh1, Young Sub Lee1, Uiju Cho1, Ja Seong Bae2, Sohee Lee2, Min Hee Kim3, Dong Jun Lim3, Gyeong Sin Park1, Youn Soo Lee1, Chan Kwon Jung1
-
Korean Journal of Pathology 2014;48(3):201-208.
DOI: https://doi.org/10.4132/KoreanJPathol.2014.48.3.201
Published online: June 26, 2014
1Department of Hospital Pathology, The Catholic University of Korea College of Medicine, Seoul, Korea.
2Department of Surgery, The Catholic University of Korea College of Medicine, Seoul, Korea.
3Department of Internal Medicine, The Catholic University of Korea College of Medicine, Seoul, Korea.
- Corresponding Author: Chan Kwon Jung, M.D. Department of Hospital Pathology, Seoul St. Mary's Hospital, The Catholic University of Korea College of Medicine, 222 Banpo-daero, Seocho-gu, Seoul 137-701, Korea. Tel: +82-2-2258-1622, Fax: +82-2-2258-1627, ckjung@catholic.ac.kr
© 2014 The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Background
- The tall cell variant of papillary thyroid carcinoma (TCVPTC) is more aggressive than classic papillary thyroid carcinoma (PTC), but the percentage of tall cells needed to diagnose TCVPTC remains controversial. In addition, little is known about the clinicopathologic features of classic PTC with tall cell features (TCF).
-
Methods
- We retrospectively selected and reviewed the clinicopathologic features and presence of the BRAF mutation in 203 cases of classic PTC, 149 cases of classic PTC with TCF, and 95 cases of TCVPTCs, which were defined as PTCs having <10%, 10-50%, and ≥50% tall cells, respectively.
-
Results
- TCVPTCs and classic PTCs with TCF did not vary significantly in clinicopathologic characteristics such as pathologic (p) T stage, extrathyroidal extension, pN stage, lateral lymph node metastasis, or BRAF mutations; however, these features differed significantly in TCVPTCs and classic PTCs with TCF in comparison to classic PTCs. Similar results were obtained in a subanalysis of patients with microcarcinomas (≤1.0 cm in size).
-
Conclusions
- Classic PTCs with TCF showed a similar BRAF mutation rate and clinicopathologic features to TCVPTCs, but more aggressive characteristics than classic PTCs.
- Patients
- We performed a retrospective review of a prospectively maintained database of patients with PTC under approval by the Institutional Review Board of The Catholic University of Korea Seoul St. Mary's Hospital (KC13RISI0917). A total of 2,139 patients underwent surgery for PTC St. Mary's Hospital between January 2012 and December 2013. We enrolled a total of 244 consecutive patients with TCVPTC (n=95) and classic PTC with TCF (n=149) and also selected 203 consecutive patients with classic PTC as a control group. The age of the patients at the time of diagnosis ranged from 22 to 79 years (mean 47.6 years for classic PTC, mean 51.0 years for classic PTC with TCF, and mean 47.1 years for TCVPTC).
- Histopathologic review
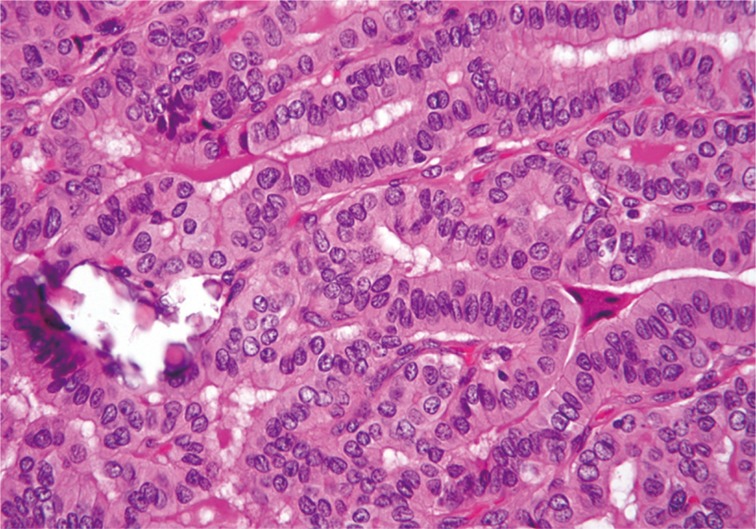
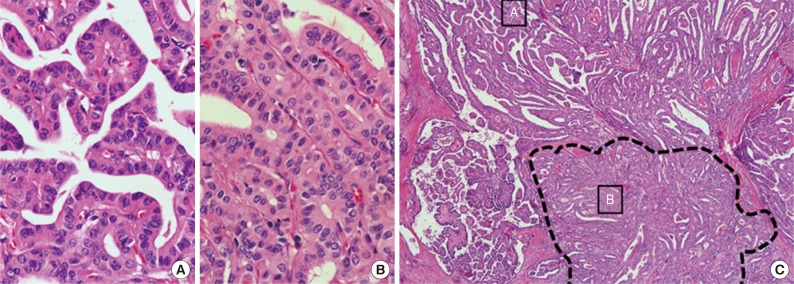
- All classic PTC, classic PTC with TCF and TCVPTC cases were reviewed by three board-certified surgical pathologists (C.K.J, G.S.P, and Y.S.L) with special interest in thyroid to identify clinicopathologic characteristics and the percentage of tall cells. Tall cells were defined as cells with a height at least three times their width, abundant eosinophilic cytoplasm and nuclear features characteristic of classic PTCs such as enlarged, irregular, clear nuclei with grooves and pseudo-inclusions (Fig. 1).2,5,13,19 A tumor was classified as a classic PTC if it had any well-formed papillary structure and contained <10% tall cells. A tumor was further defined as classic PTC with TCF if it harbored between 10% and 50% tall cells (Fig. 2) and as a TCVPTC if it contained 50% or more tall cells. The 50% criterion for TCVPTC was based on the World Health Organization classification and previous studies on TCVPTC.5,12,13,15,18,19,20,21 To determine whether samples reached the cutoff values of 10% and 50% of tall cells in the whole sections of tumor tissue, we used a digital training set which has the known percentage calculated from digitization of whole slide imaging. Discrepancies between the observers were found in less than 10% of the reviewed slides. A consensus was reached when there was discrepancy between the observers. We excluded any cases with tumor necrosis or marked mitotic activity (≥3 mitoses/10 high power field, 400×) because these pathologic features themselves could be related to tumor aggressiveness.5,6,19,20 In cases with multiple tumor foci, the largest tumors were selected as the primary lesions. TNM staging was performed according to the American Joint Committee's Cancer staging manual 7th edition.
- BRAF mutation analysis
- Of a total of 447 PTC cases, 417 underwent BRAF mutation testing. Genomic DNA was extracted from two or three 10-µm thick paraffin tissue sections using the QIAamp DNA Mini kit (Qiagen, Hilden, Germany). The tissue sections were manually microdissected to enrich for tumor cells. We screened for mutations in exon 15 of the BRAF gene using polymerase chain reaction amplification and direct DNA sequencing, as described previously.8,22
- Statistical analysis
- We used Student's t-test to compare two different groups of continuous parametric data with a normal distribution. Pearson's chi-square test was used to assess the relationship between categorical variables. For the multivariate analysis, we included all variables with a univariate probability (p) value of <.10 in a binary logistic regression test. Two-sided p-values <.05 were considered to be statistically significant. Statistical analysis was performed with SPSS ver. 16.0 (SPSS Inc., Chicago, IL, USA).
MATERIALS AND METHODS
- Out of a total of 2,139 patients with PTCs, 149 (7.0%) had classic PTC with TCF and 95 (4.4%) had TCVPTC.
- Comparison of clinicopathologic characteristics among histopathologic types
- When the clinicopathologic features of classic PTCs were compared with those of TCVPTCs and classic PTCs with TCF, patients with classic PTCs were younger at the time of surgery and showed lower pT and pN stages, a lower rate of extrathyroidal extension, a lower rate of lateral lymph node metastasis, and a lower frequency of BRAF mutations (Table 1). All BRAF mutations were V600E mutations. There were no statistically significant differences between TCVPTCs and classic PTCs with TCF with regard to mean age and clinicopathologic features such as pT, extrathyroidal extension, pN, lateral lymph node metastasis, or rate of BRAF mutation (Table 1). In multivariate analysis (Table 2), age group, extrathyroidal extension, lymph node metastasis, and BRAF mutations of classic PTC were significantly different from those of TCVPTCs and classic PTCs with TCF. The clinicopathologic features of TCVPTCs were not significantly different from those of classic PTCs with TCF.
- Subanalysis of microcarcinomas (≤1.0 cm in size) according to histologic subtype
- Patients with classic PTCs were younger at surgery and showed a higher frequency of single lesions, lower pT and pN stages, a lower rate of extrathyroidal extension, and a lower frequency of BRAF mutations, compared to patients with classic PTCs with TCF or TCVPTCs (Table 3). There were no statistically significant differences in clinicopathologic characteristics between TCVPTCs and classic PTCs with TCF (Table 3).
- Subanalysis of unifocal tumors according to histologic subtype
- We only included unifocal cancers to eliminate any possible bias from tumor multifocality. We further analyzed the clinicopathologic differences between classic PTCs, classic PTCs with TCF or TCVPTCs. The results for unifocal cancers were in the same range: clinicopathologic features of classic PTCs were significantly different from those of classic PTCs with TCF or TCVPTCs, but no significant differences were observed in clinicopathologic characteristics between TCVPTCs and classic PTCs with TCF (Appendices 1, 2).
- Subanalysis of histologic subtypes according to patient age groups (<45 years vs ≥45 years)
- In a multivariate subanalysis by patient age group (Table 4), there were no significant differences in clinicopathologic variables between patients under or over the age of 45 in the classic PTC with TCF and TCVPTC groups. The clinicopathologic features of classic PTCs were significantly different from those of classic PTCs with TCF or TCVPTCs across age groups.
RESULTS
- We demonstrated that classic PTC with TCF (PTC with 10% to 50% tall cells) had the same demographic and clinicopathologic characteristics as TCVPTC, and these tumors showed more aggressive features than classic PTC.
- TCVPTC typically affects older patients and has a larger size, higher stage at presentation, higher rate of extrathyroidal extension, greater risk of recurrence, and poorer disease-specific survival compared to classic PTC.3,4,9,16,18,19,23 Bernstein et al.24 indicated that despite controlling for size, TCVs of papillary thyroid microcarcinomas were still associated with higher pT and, pN stage and aggressive pathologic features such as extrathyroidal extension. In our study, we also demonstrated that microcarcinomas with a tall cell component were more aggressive than those with classic PTC morphology.
- There is controversy regarding the high incidence of lymph node metastasis in TCVPTC. Some authors have demonstrated that patients with TCVPTC have a higher rate of nodal metastases than patients with classic PTC.4,16 Bernstein et al.24 showed that microcarcinomas with TCVPTC have a higher rate of central lymph node metastasis than microcarcinomas with classic PTC (39% vs 13%). However, other authors did not find significant differences in the lymph node positivity rate between classic PTCs and TCVPTCs.3,17,19 For example, Ganly et al.19 demonstrated no differences in nodal metastases among TCVPTCs, classic PTCs with TCF and classic PTCs. Such discrepancies might be caused by different patient ages or different criteria regarding the percentage of tall cells necessary for a diagnosis of TCVPTC. In our multivariate analysis according to the age groups, there were significant differences in the rates of lymph node metastasis between classic PTC and classic PTC with TCF in patients under the age of 45 years. However, the differences in lymph node metastasis rate disappeared in patients over the age of 45 years. Johnson et al.16 and Bernstein et al.24 used a 30% threshold of tall cells and showed a higher rate of nodal positivity in TCVPTCs. Investigators who used a 50% to 75% threshold of tall cells for TCVPTC diagnosis did not find a significant differences in nodal positivity between TCVPTCs and classic PTCs.17,19
- Various investigators have used different thresholds of 10%,15 30%,11,15,24 50%,5,12,13,15,18,19,20,21 70%,3 or 75%2,14,17 tall cells to define TCVPTC. Ghossein and LiVolsi5 and Regalbuto et al.18 suggested a cut-off of at least 50% tall cells to classify TCVPTC.
- In our study, we used a 10% threshold for classic PTCs with TCF and a 50% threshold for TCVPTCs. Using this definition, lymph node metastases were significantly more frequent in classic PTCs with TCF and TCVPTCs than in classic PTCs. We also demonstrated a statistically significant difference between classic PTCs and classic PTCs with TCF (10% to 50% tall cells) with regard to lymph node status such as pN and lateral lymph node metastasis (Table 1).
- Beninato et al.15 reported that patients with classic PTC with TCF (tumors with ≥10% tall cells) have more aggressive tumor features such as older age at onset, higher stage, more extrathyroidal extension (3% to 14%), more lymph node metastases (40% to 68%), increased lymphovascular invasion (2% to 17%), and a higher frequency of positive surgical margins, compared with classic PTC. These aggressive features have been shown to be associated with a greater risk of recurrence and were maintained with increasing tall cell percentage (≥10%, ≥30%, ≥50%) within PTCs with tall cells.15 Other authors have suggested that classic PTCs with TCF may be significantly associated with older age at presentation, larger tumor size, higher frequency of extrathyroidal extension, and BRAF mutations regardless of the percentage of tall cells.13 We also demonstrated a statistically significant difference in clinicopathologic features and BRAF mutations between classic PTCs and classic PTCs with TCF (10% to 50% tall cells) (Table 1).
- The more aggressive clinicopathologic features of classic PTCs with TCF and TCVPTCs at presentation translate into worse outcomes.19 Recent clinical guidelines also suggest that TCVPTCs require more aggressive surgical resection.25 The aggressive nature of TCVPTC may be related to a higher prevalence of BRAF mutations.26 BRAF mutations in PTC have been correlated with aggressive tumor behavior, including extrathyroidal extension, tumor recurrence, advanced tumor stage at presentation and lymph node metastasis,27 even in microcarcinomas.28 The BRAF oncogene is a strong activator of the mitogen-activated protein kinase signaling pathway, which leads to uncontrolled cell proliferation and transformation into malignancy.29 BRAF mutation also plays a role in extracellular matrix remodeling and is associated with an increase in matrix metalloproteinases, a desmoplastic stromal reaction, and invasiveness.30 Finkelstein et al.21 demonstrated a significant association between the presence of the BRAF mutation and fibrosis, desmoplastic stromal reaction, and infiltrating tumor borders. The BRAF mutation occurs commonly in Korean patients with PTC, ranging in frequency from 52% to 87% of all cases.8 The prevalence of the BRAF mutation worldwide is reported to be as high as 80% to 100% in TCVPTCs.29 For example, Bernstein et al.24 demonstrated that the BRAF mutation was detected in 93% of all microcarcinomas with TCVPTC. In our study, the prevalence of the BRAF mutation was 96.9% and 96.4% in classic PTCs with TCF and TCVPTCs, respectively.
- Age at presentation is the single most important prognostic factor in thyroid cancer.1 In our study, we found that classic PTCs with TCF and TCVPTCs were more frequent in patients over the age of 45. Interestingly, PTCs with ≥10% tall cells were pathologically more aggressive than classic PTCs regardless of age groups (<45 years and ≥45 years).
- Our study has some limitations, such as a retrospective design, relatively small sample size, and the fact that the data were collected by one institution. Furthermore, we did not analyze the outcomes and prognosis of patients because the follow-up period was too short.
- In conclusion, PTCs with more than 10% tall cells show more aggressive clinicopathologic features than classic PTCs regardless of tumor size and age. Classic PTCs with TCF have a similar BRAF mutation rate and clinicopathologic characteristics to those of TCVPTCs. Therefore, we suggest that the presence of any tall cells should be noted in pathologic reports because of their clinical significance.
DISCUSSION
Acknowledgments
Acknowledgments
- 1. LiVolsi VA. Papillary thyroid carcinoma: an update. Mod Pathol 2011; 24(Suppl 2): S1-S9. ArticlePubMedPDF
- 2. LiVolsi VA. Papillary carcinoma tall cell variant (TCV): a review. Endocr Pathol 2010; 21: 12-15. ArticlePubMedPDF
- 3. Ostrowski ML, Merino MJ. Tall cell variant of papillary thyroid carcinoma: a reassessment and immunohistochemical study with comparison to the usual type of papillary carcinoma of the thyroid. Am J Surg Pathol 1996; 20: 964-974. PubMed
- 4. Michels JJ, Jacques M, Henry-Amar M, Bardet S. Prevalence and prognostic significance of tall cell variant of papillary thyroid carcinoma. Hum Pathol 2007; 38: 212-219. ArticlePubMed
- 5. Ghossein R, LiVolsi VA. Papillary thyroid carcinoma tall cell variant. Thyroid 2008; 18: 1179-1181. ArticlePubMed
- 6. Urano M, Kiriyama Y, Takakuwa Y, Kuroda M. Tall cell variant of papillary thyroid carcinoma: its characteristic features demonstrated by fine-needle aspiration cytology and immunohistochemical study. Diagn Cytopathol 2009; 37: 732-737. ArticlePubMed
- 7. Choi YJ, Shin JH, Kim JH, Jung SL, Son EJ, Oh YL. Tall cell variant of papillary thyroid carcinoma: sonographic and clinical findings. J Ultrasound Med 2011; 30: 853-858. PubMed
- 8. Jung CK, Im SY, Kang YJ, et al. Mutational patterns and novel mutations of the BRAF gene in a large cohort of Korean patients with papillary thyroid carcinoma. Thyroid 2012; 22: 791-797. ArticlePubMed
- 9. Hawk WA, Hazard JB. The many appearances of papillary carcinoma of the thyroid. Cleve Clin Q 1976; 43: 207-215. ArticlePubMed
- 10. Morris LG, Shaha AR, Tuttle RM, Sikora AG, Ganly I. Tall-cell variant of papillary thyroid carcinoma: a matched-pair analysis of survival. Thyroid 2010; 20: 153-158. ArticlePubMedPMC
- 11. Terry JH, St John SA, Karkowski FJ, et al. Tall cell papillary thyroid cancer: incidence and prognosis. Am J Surg 1994; 168: 459-461. ArticlePubMed
- 12. Ghossein RA, Leboeuf R, Patel KN, et al. Tall cell variant of papillary thyroid carcinoma without extrathyroid extension: biologic behavior and clinical implications. Thyroid 2007; 17: 655-661. ArticlePubMed
- 13. Lee SH, Jung CK, Bae JS, Jung SL, Choi YJ, Kang CS. Liquid-based cytology improves preoperative diagnostic accuracy of the tall cell variant of papillary thyroid carcinoma. Diagn Cytopathol 2014; 42: 11-17. ArticlePubMed
- 14. Min HS, Lee C, Jung KC. Correlation of immunohistochemical markers and BRAF mutation status with histological variants of papillary thyroid carcinoma in the Korean population. J Korean Med Sci 2013; 28: 534-541. ArticlePubMedPMCPDF
- 15. Beninato T, Scognamiglio T, Kleiman DA, et al. Ten percent tall cells confer the aggressive features of the tall cell variant of papillary thyroid carcinoma. Surgery 2013; 154: 1331-1336. ArticlePubMed
- 16. Johnson TL, Lloyd RV, Thompson NW, Beierwaltes WH, Sisson JC. Prognostic implications of the tall cell variant of papillary thyroid carcinoma. Am J Surg Pathol 1988; 12: 22-27. ArticlePubMed
- 17. Akslen LA, LiVolsi VA. Prognostic significance of histologic grading compared with subclassification of papillary thyroid carcinoma. Cancer 2000; 88: 1902-1908. ArticlePubMed
- 18. Regalbuto C, Malandrino P, Frasca F, et al. The tall cell variant of papillary thyroid carcinoma: clinical and pathological features and outcomes. J Endocrinol Invest 2013; 36: 249-254. PubMed
- 19. Ganly I, Ibrahimpasic T, Rivera M, et al. Prognostic implications of papillary thyroid carcinoma with tall-cell features. Thyroid 2014; 24: 662-670. ArticlePubMed
- 20. Rivera M, Ghossein RA, Schoder H, Gomez D, Larson SM, Tuttle RM. Histopathologic characterization of radioactive iodine-refractory fluorodeoxyglucose-positron emission tomography-positive thyroid carcinoma. Cancer 2008; 113: 48-56. ArticlePubMed
- 21. Finkelstein A, Levy GH, Hui P, et al. Papillary thyroid carcinomas with and without BRAF V600E mutations are morphologically distinct. Histopathology 2012; 60: 1052-1059. ArticlePubMed
- 22. Jung CK, Choi YJ, Lee KY, et al. The cytological, clinical, and pathological features of the cribriform-morular variant of papillary thyroid carcinoma and mutation analysis of CTNNB1 and BRAF genes. Thyroid 2009; 19: 905-913. ArticlePubMed
- 23. Jalisi S, Ainsworth T, Lavalley M. Prognostic outcomes of tall cell variant papillary thyroid cancer: a meta-analysis. J Thyroid Res 2010; 2010: 325602.ArticlePubMedPMCPDF
- 24. Bernstein J, Virk RK, Hui P, et al. Tall cell variant of papillary thyroid microcarcinoma: clinicopathologic features with BRAF(V600E) mutational analysis. Thyroid 2013; 23: 1525-1531. ArticlePubMed
- 25. American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer. Cooper DS, Doherty GM, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid 2009; 19: 1167-1214. ArticlePubMed
- 26. Adeniran AJ, Zhu Z, Gandhi M, et al. Correlation between genetic alterations and microscopic features, clinical manifestations, and prognostic characteristics of thyroid papillary carcinomas. Am J Surg Pathol 2006; 30: 216-222. ArticlePubMed
- 27. Tufano RP, Teixeira GV, Bishop J, Carson KA, Xing M. BRAF mutation in papillary thyroid cancer and its value in tailoring initial treatment: a systematic review and meta-analysis. Medicine (Baltimore) 2012; 91: 274-286. PubMed
- 28. Xing M. BRAF mutation in papillary thyroid microcarcinoma: the promise of better risk management. Ann Surg Oncol 2009; 16: 801-803. ArticlePubMedPMC
- 29. Xing M. BRAF mutation in thyroid cancer. Endocr Relat Cancer 2005; 12: 245-262. ArticlePubMed
- 30. Mesa C Jr, Mirza M, Mitsutake N, et al. Conditional activation of RET/PTC3 and BRAFV600E in thyroid cells is associated with gene expression profiles that predict a preferential role of BRAF in extracellular matrix remodeling. Cancer Res 2006; 66: 6521-6529. ArticlePubMedPDF
REFERENCES
Appendix
Appendix 1.
| Characteristic | Classic PTC (A) (%) | Classic PTC with TCF (B) (%) | TCVPTC (C) (%) | p-value (A vs B+C) | p-value (A vs B) | p-value (B vs C) |
|---|---|---|---|---|---|---|
| No. of cases | 111 | 65 | 49 | |||
| Mean age (yr) | 44.8 | 51.2 | 43.9 | NS | .011 | .46 |
| Age (yr) | NS | .012 | .02 | |||
| < 45 | 52 (46.8) | 18 (27.7) | 24 (49.0) | |||
| ≥ 45 | 59 (53.2) | 47 (72.3) | 25 (51.0) | |||
| Gender | NS | NS | NS | |||
| Female | 89 (80.2) | 51 (78.5) | 41 (83.7) | |||
| Male | 22 (19.8) | 14 (21.5) | 8 (16.3) | |||
| pT stage | .000 | .000 | NS | |||
| pT1 | 70 (63.1) | 20 (30.8) | 12 (24.5) | |||
| pT2 | 2 (1.8) | 1 (1.5) | 0 (0) | |||
| pT3 | 39 (35.1) | 44 (67.7) | 37 (75.5) | |||
| pT4 | 0 (0) | 0 (0) | 0 (0) | |||
| ETE | .000 | .000 | NS | |||
| Absent | 72 (64.9) | 21 (32.3) | 12 (24.5) | |||
| Present | 39 (35.1) | 44 (67.7) | 37 (75.5) | |||
| pN stagea | .000 | .007 | NS | |||
| pN0 | 66 (59.5) | 24 (38.1) | 13 (26.5) | |||
| pN1 | 45 (40.5) | 39 (61.9) | 36 (73.5) | |||
| Lateral LNM | .005 | .005 | NS | |||
| Absent | 107 (96.4) | 53 (84.1) | 43 (87.8) | |||
| Present | 4 (3.6) | 10 (15.9) | 6 (12.2) | |||
| BRAF mutationb | .002 | .018 | NS | |||
| Absent | 18 (16.2) | 2 (3.6) | 1 (2.4) | |||
| Present | 93 (83.8) | 54 (96.4) | 41 (97.6) |
Appendix 2.
| Characteristic | Classic PTC (A) (%) | Classic PTC with TCF (B) (%) | TCVPTC (C) (%) | p-value (A vs B+C) | p-value (A vs B) | p-value (B vs C) |
|---|---|---|---|---|---|---|
| No. of cases | 96 | 29 | 21 | |||
| Mean age (yr) | 45.3 | 52.8 | 46.5 | |||
| Age (yr) | .037 | .023 | NS | |||
| < 45 | 46 (47.9) | 7 (24.1) | 8 (38.1) | |||
| ≥ 45 | 50 (52.1) | 22 (75.9) | 13 (61.9) | |||
| Gender | NS | NS | NS | |||
| Female | 75 (78.1) | 24 (82.8) | 19 (90.5) | |||
| Male | 21 (21.9) | 5 (17.2) | 2 (9.5) | |||
| pT stage | .019 | NS | NS | |||
| pT1a | 67 (69.8) | 15 (51.7) | 10 (47.6) | |||
| pT3 | 29 (30.2) | 14 (48.3) | 11 (52.4) | |||
| pN stagea | .032 | NS | NS | |||
| pN0 | 61 (63.5) | 14 (50.0) | 8 (38.1) | |||
| pN1 | 35 (36.5) | 14 (50.0) | 13 (61.9) | |||
| Lateral LNM | NS | .041 | NS | |||
| Absent | 94 (97.9) | 25 (89.3) | 20 (95.2) | |||
| Present | 2 (2.1) | 3 (10.7) | 1 (4.8) | |||
| BRAF mutationb | .047 | NS | NS | |||
| Absent | 16 (16.7) | 1 (4.0) | 1 (5.3) | |||
| Present | 80 (83.3) | 24 (96.0) | 18 (94.7) |
| Characteristic | Classic PTC (A) (%) | Classic PTC with TCF (B) (%) | TCVPTC (C) (%) | p-value (A vs B+C) | p-value (A vs B) | p-value (B vs C) |
|---|---|---|---|---|---|---|
| No. of cases | 203 | 149 | 95 | |||
| Mean age | 47.6 | 51.0 | 47.1 | .000 | .000 | .017 |
| Age (yr) | .002 | .000 | .042 | |||
| < 45 | 95 (46.8) | 41 (27.5) | 38 (40.0) | |||
| ≥ 45 | 108 (53.2) | 108 (72.5) | 57 (60.0) | |||
| Gender | NS | NS | NS | |||
| Female | 164 (80.8) | 123 (82.6) | 82 (86.3) | |||
| Male | 39 (19.2) | 26 (17.4) | 13 (13.7) | |||
| Multifocality | NS | .040 | NS | |||
| Single | 111 (54.7) | 65 (43.6) | 49 (51.6) | |||
| Multiple | 92 (45.3) | 84 (56.4) | 46 (48.4) | |||
| pT stage | .000 | .000 | NS | |||
| pT1 | 126 (62.0) | 41 (27.5) | 23 (24.2) | |||
| pT2 | 3 (1.5) | 3 (2.0) | 0 (0) | |||
| pT3 | 74 (36.5) | 104 (69.8) | 71 (74.7) | |||
| pT4 | 0 (0) | 1 (0.7) | 1 (1.1) | |||
| ETE | .000 | .000 | NS | |||
| Absent | 129 (63.5) | 44 (29.5) | 23 (24.2) | |||
| Present | 74 (36.5) | 105 (70.5) | 72 (75.8) | |||
| pN stagea | .000 | .003 | NS | |||
| pN0 | 105 (51.7) | 51 (35.4) | 27 (29.0) | |||
| pN1 | 98 (48.3) | 93 (64.6) | 66 (71.0) | |||
| Lateral LNM | .003 | .002 | NS | |||
| Absent | 191 (94.1) | 121 (84.0) | 81 (87.1) | |||
| Present | 12 (5.9) | 23 (16.0) | 12 (12.9) | |||
| BRAF mutationb | .000 | .000 | NS | |||
| Absent | 34 (16.7) | 4 (3.1) | 3 (3.6) | |||
| Present | 169 (83.3) | 127 (96.9) | 80 (96.4) |
| Characteristic |
Odds ratio (95% confidence interval) |
||
|---|---|---|---|
| A vs B+C | A vs B | B vs C | |
| Age (< 45 yr vs ≥ 45 yr) | 1.92 (1.22-3.01)a | 2.39 (1.42-4.04)a | 0.66 (0.36-1.23) |
| Gender (female vs male) | 0.88 (0.50-1.56) | 1.03 (0.54-1.95) | 0.63 (0.28-1.42) |
| Multifocality (unifocal vs multifocal) | 1.28 (0.83-1.97) | 1.50 (0.92-2.44) | 0.68 (0.38-1.21) |
| ETE (absent vs present) | 3.30 (2.13-5.10)a | 2.81 (1.70-4.64)a | 1.57 (0.82-2.98) |
| LN metastasis (absent vs present) | 1.84 (1.17-2.90)a | 1.71 (1.01-2.90)a | 1.10 (0.58-2.07) |
| BRAF mutation (absent vs present) | 5.14 (2.15-12.65)a | 5.26 (1.75-15.76)a | 0.82 (0.17-3.91) |
| Characteristic | Classic PTC (A) (%) | Classic PTC with TCF (B) (%) | TCVPTC (C) (%) | p-value (A vs B+C) | p-value (A vs B) | p-value (B vs C) |
|---|---|---|---|---|---|---|
| No. of cases | 164 | 67 | 43 | |||
| Mean age (yr) | 45.6 | 51.3 | 48.7 | .001 | .000 | NS |
| Age (yr) | .003 | .006 | NS | |||
| < 45 | 76 (46.3) | 18 (26.9) | 13 (30.2) | |||
| ≥ 45 | 88 (53.7) | 49 (73.1) | 30 (69.8) | |||
| Gender | .034 | NS | NS | |||
| Female | 132 (80.5) | 60 (89.6) | 39 (90.7) | |||
| Male | 32 (19.5) | 7 (10.4) | 4 (9.3) | |||
| Multifocality | .033 | .035 | NS | |||
| Single | 96 (58.5) | 29 (43.3) | 21 (48.8) | |||
| Multiple | 68 (41.5) | 38 (56.7) | 22 (51.2) | |||
| pT stage | .000 | .000 | NS | |||
| pT1a | 120 (73.2) | 28 (41.8) | 17 (39.5) | |||
| pT3 | 44 (26.8) | 39 (58.2) | 26 (60.5) | |||
| pN stagea | .014 | NS | NS | |||
| pN0 | 94 (57.3) | 29 (45.3) | 15 (36.6) | |||
| pN1 | 70 (42.7) | 35 (54.7) | 26 (63.4) | |||
| Lateral LNM | .045 | .007 | NS | |||
| Absent | 160 (97.6) | 57 (89.1) | 40 (97.6) | |||
| Present | 4 (2.4) | 7 (10.9) | 1 (2.4) | |||
| BRAF mutationb | .001 | .005 | NS | |||
| Absent | 29 (17.7) | 2 (3.3) | 2 (5.1) | |||
| Present | 135 (82.3) | 59 (96.7) | 37 (94.9) |
| Characteristic |
Odds ratio (95% confidence interval) |
||
|---|---|---|---|
| A vs B+C | A vs B | B vs C | |
| Age < 45 yr | |||
| Gender (female vs male) | 0.68 (0.29-1.60) | 0.96 (0.35-2.58) | 0.44 (0.11-1.72) |
| Multifocality (unifocal vs multifocal) | 0.93 (0.45-1.89) | 1.44 (0.59-3.47) | 0.37 (0.13-1.04) |
| ETE (absent vs present) | 2.91 (1.45-5.85)a | 2.99 (1.25-7.10)a | 0.82 (0.28-2.38) |
| LN metastasis (absent vs present) | 2.95 (1.33-6.56)a | 3.76 (1.25-11.30)a | 0.53 (0.15-1.92) |
| BRAF mutation (absent vs present) | 16.58 (2.04-135.07)a | 7.75E8 | 0.00 |
| Age ≥ 45 yr | |||
| Gender (female vs male) | 1.04 (0.48-2.28) | 1.06 (0.45-2.48) | 0.83 (0.30-2.29) |
| Multifocality (unifocal vs multifocal) | 1.48 (0.86-2.57) | 1.43 (0.79-2.61) | 0.96 (0.47-1.97) |
| ETE (absent vs present) | 3.62 (2.05-6.38)a | 2.80 (1.50-5.21)a | 2.18 (0.92-5.15) |
| LN metastasis (absent vs present) | 1.49 (0.84-2.63) | 1.31 (0.70-2.46) | 1.34 (0.64-2.84) |
| BRAF mutation (absent vs present) | 3.55 (1.27-9.97)a | 3.33 (1.04-10.71)a | 1.03 (0.17-6.15) |
Figure & Data
References
Citations
- Clinicopathologic characteristics of papillary thyroid carcinoma, tall cell subtype and subtype with tall cell features, an institutional experience
Xueting Jin, Shunsuke Koga, Xiao Zhou, Niaz Z. Khan, Zubair W. Baloch
Human Pathology.2025; 161: 105867. CrossRef - Association Between BRAF V600E Allele Frequency and Aggressive Behavior in Papillary Thyroid Microcarcinoma
Luiza Tatar, Saruchi Bandargal, Marc P. Pusztaszeri, Véronique-Isabelle Forest, Michael P. Hier, Jasmine Kouz, Raisa Chowdhury, Richard J. Payne
Cancers.2025; 17(15): 2553. CrossRef - Papillary Thyroid Carcinoma and Body Mass Index: The Role of Immune System in Tumor Microenvironment
Rebecca Sparavelli, Riccardo Giannini, Francesca Signorini, Gabriele Materazzi, Alessio Basolo, Ferruccio Santini, Clara Ugolini
International Journal of Molecular Sciences.2025; 26(17): 8290. CrossRef - External validation of a deep learning-based algorithm for detection of tall cells in papillary thyroid carcinoma: A multicenter study
Sebastian Stenman, Sylvain Bétrisey, Paula Vainio, Jutta Huvila, Mikael Lundin, Nina Linder, Anja Schmitt, Aurel Perren, Matthias S. Dettmer, Caj Haglund, Johanna Arola, Johan Lundin
Journal of Pathology Informatics.2024; 15: 100366. CrossRef - Focal Tall Cell Change in Papillary Thyroid Carcinoma: Lessons Learned from Practices Adopting Rigid Criteria (Height to Width Ratio of 3)
Esther Diana Rossi, Liron Pantanowitz
Endocrine Pathology.2024; 35(1): 80. CrossRef - Predicting tall-cell subtype of papillary thyroid carcinomas independently with preoperative multimodal ultrasound
Bei-Bei Ye, Yun-Yun Liu, Ying Zhang, Bo-Ji Liu, Le-Hang Guo, Qing Wei, Yi-Feng Zhang, Hui-Xiong Xu
British Journal of Radiology.2024; 97(1159): 1311. CrossRef - TERT mutations and aggressive histopathologic characteristics of radioiodine-refractory papillary thyroid cancer
Ju Yeon Pyo, Yoon Jin Cha, SoonWon Hong
Journal of Pathology and Translational Medicine.2024; 58(6): 310. CrossRef - Papillary Thyroid Carcinomas with Tall Cell Features: An Intermediate Entity Between Classic and Tall Cell Subtypes
Athanasios Bikas, Kristine Wong, Theodora Pappa, Sara Ahmadi, Craig B. Wakefield, Ellen Marqusee, Pingping Xiang, Benjamin Altshuler, Jacob Haase, Justine A. Barletta, Iñigo Landa, Erik K. Alexander
Thyroid.2023; 33(6): 697. CrossRef - A novel nomogram for identifying high-risk patients among active surveillance candidates with papillary thyroid microcarcinoma
Li Zhang, Peisong Wang, Kaixuan Li, Shuai Xue
Frontiers in Endocrinology.2023;[Epub] CrossRef - The Impact of BRAF V600E Mutation Allele Frequency on the Histopathological Characteristics of Thyroid Cancer
Mawaddah Abdulhaleem, Saruchi Bandargal, Marc Philippe Pusztaszeri, Mohannad Rajab, Hannah Greenspoon, Joshua Ross Krasner, Sabrina Daniela Da Silva, Véronique-Isabelle Forest, Richard J. Payne
Cancers.2023; 16(1): 113. CrossRef - Protruding Huge Thyroid Mass Concurrent Hemorrhage and Skin Necrosis: A Case Report
Solji An, Joonseon Park, Kwangsoon Kim, Ja Seong Bae, Jeong Soo Kim
Journal of Endocrine Surgery.2023; 23(4): 143. CrossRef - CD56 Expression in Papillary Thyroid Carcinoma Is Highly Dependent on the Histologic Subtype: A Potential Diagnostic Pitfall
Uiju Cho, Yourha Kim, Sora Jeon, Chan Kwon Jung
Applied Immunohistochemistry & Molecular Morphology.2022; 30(5): 389. CrossRef - Aggressive histopathological variants of papillary thyroid carcinoma, diagnostic challenge, and clinical significance—A case series
PK Pravanya, KR Anila, Shaji Thomas, A Sreekumar, K Jayasree
Medical Journal of Dr. D.Y. Patil Vidyapeeth.2022; 15(6): 922. CrossRef - Tall cell variant papillary thyroid carcinoma impacts disease-free survival at the 10 % cut-point on multivariate analysis
Shabnam Samankan, Leah Militello, Gabriella Seo, Sedef Everest, Quinn O'Malley, Sarah L. Spaulding, Monica Xing, Ammar Matloob, John Beute, Raymond Chai, Scott Doyle, Mark L. Urken, Margaret Brandwein-Weber
Pathology - Research and Practice.2022; 236: 154012. CrossRef - A population-based study of the three major variants of papillary thyroid carcinoma
Junming Xu, Yingying Zhang, Jun Liu, Shenglong Qiu, Min Wang
Journal of International Medical Research.2021;[Epub] CrossRef - Tall cell percentage alone in PTC without aggressive features should not guide patients’ clinical management
Anello Marcello Poma, David Viola, Elisabetta Macerola, Agnese Proietti, Eleonora Molinaro, Dario De Vietro, Rossella Elisei, Gabriele Materazzi, Paolo Miccoli, Fulvio Basolo, Clara Ugolini
The Journal of Clinical Endocrinology & Metabolism.2021; 106(10): e4109. CrossRef - Molecular Pathology of Non-familial Follicular Epithelial–Derived Thyroid Cancer in Adults: From RAS/BRAF-like Tumor Designations to Molecular Risk Stratification
Paula Soares, Antónia Afonso Póvoa, Miguel Melo, João Vinagre, Valdemar Máximo, Catarina Eloy, José Manuel Cameselle-Teijeiro, Manuel Sobrinho-Simões
Endocrine Pathology.2021; 32(1): 44. CrossRef - Deep Neck Infection: Atypical Presentation of Papillary Thyroid Cancer
Apichana Mahattanapreut, Rangsima Aroonroch, Chalermchai Chintrakarn, Chutintorn Sriphrapradang, Dinesh K. Chhetri
Case Reports in Otolaryngology.2021; 2021: 1. CrossRef - The evolving concept of aggressive histological variants of differentiated thyroid cancer
Juan C. Hernandez-Prera
Seminars in Diagnostic Pathology.2020; 37(5): 228. CrossRef - Papillary Thyroid Cancer—Aggressive Variants and Impact on Management: A Narrative Review
Andrés Coca-Pelaz, Jatin P. Shah, Juan C. Hernandez-Prera, Ronald A. Ghossein, Juan P. Rodrigo, Dana M. Hartl, Kerry D. Olsen, Ashok R. Shaha, Mark Zafereo, Carlos Suarez, Iain J. Nixon, Gregory W. Randolph, Antti A. Mäkitie, Luiz P. Kowalski, Vincent Van
Advances in Therapy.2020; 37(7): 3112. CrossRef - Contemporary evaluation and management of tall cell variant of papillary thyroid carcinoma
Sara Cartwright, Abbey Fingeret
Current Opinion in Endocrinology, Diabetes & Obesity.2020; 27(5): 351. CrossRef - Le carcinome papillaire de la thyroïde avec contingent à cellules hautes : facteurs pronostiques
I. Riahi, H. Jaafoura, H. Saibi, E. Chebil, I. Ben Nacef, M. Ksentini, T. Ben Ghachem, R. Lahiani, M. Ben Salah
Annales d'Endocrinologie.2020; 81(4): 345. CrossRef - Updates in the Pathologic Classification of Thyroid Neoplasms: A Review of the World Health Organization Classification
Yanhua Bai, Kennichi Kakudo, Chan Kwon Jung
Endocrinology and Metabolism.2020; 35(4): 696. CrossRef - Tall Cell Variant of Papillary Thyroid Carcinoma: Impact of Change in WHO Definition and Molecular Analysis
Kristine S. Wong, Sara E. Higgins, Ellen Marqusee, Matthew A. Nehs, Trevor Angell, Justine A. Barletta
Endocrine Pathology.2019; 30(1): 43. CrossRef - Histopatological and molecular genetic characteristics of clinically aggressive variants of papillary thyroid carcinoma
A. V. Bogolyubova, A. Yu. Abrosimov, L. S. Selivanova, P. V. Belousov
Arkhiv patologii.2019; 81(1): 46. CrossRef - Papillary Thyroid Cancers with Focal Tall Cell Change are as Aggressive as Tall Cell Variants and Should Not be Considered as Low-Risk Disease
Pim J. Bongers, Wouter P. Kluijfhout, Raoul Verzijl, Mattan Lustgarten, Marloes Vermeer, David P. Goldstein, Karen Devon, Lorne E. Rotstein, Sylvia L. Asa, James D. Brierley, Richard W. Tsang, Shereen Ezzat, Menno R. Vriens, Ozgur Mete, Jesse D. Pasternak
Annals of Surgical Oncology.2019; 26(8): 2533. CrossRef - A case-based approach to aggressive variants of papillary thyroid carcinoma with literature review
JosephAntoine Flordelis Chatto, AnnetteLaurente Salillas
Thyroid Research and Practice.2019; 16(3): 128. CrossRef - Clinically Relevant Prognostic Parameters in Differentiated Thyroid Carcinoma
Tyler Janovitz, Justine A. Barletta
Endocrine Pathology.2018; 29(4): 357. CrossRef - Prediction of novel target genes and pathways involved in tall cell variant papillary thyroid carcinoma
Fada Xia, Bo Jiang, Yong Chen, Xin Du, Yao Peng, Wenlong Wang, Zhuolu Wang, Xinying Li
Medicine.2018; 97(51): e13802. CrossRef - Papillary thyroid carcinoma with tall cell features is as aggressive as tall cell variant: a meta-analysis
Huy Gia Vuong, Nguyen Phuoc Long, Nguyen Hoang Anh, Tran Diem Nghi, Mai Van Hieu, Le Phi Hung, Tadao Nakazawa, Ryohei Katoh, Tetsuo Kondo
Endocrine Connections.2018; 7(12): R286. CrossRef - TERT Promoter Mutation in an Aggressive Cribriform Morular Variant of Papillary Thyroid Carcinoma
Eun Ji Oh, Sohee Lee, Ja Seong Bae, Yourha Kim, Sora Jeon, Chan Kwon Jung
Endocrine Pathology.2017; 28(1): 49. CrossRef - Update on the cytologic features of papillary thyroid carcinoma variants
Marc Pusztaszeri, Manon Auger
Diagnostic Cytopathology.2017; 45(8): 714. CrossRef - Molecular correlates and rate of lymph node metastasis of non-invasive follicular thyroid neoplasm with papillary-like nuclear features and invasive follicular variant papillary thyroid carcinoma: the impact of rigid criteria to distinguish non-invasive f
Uiju Cho, Ozgur Mete, Min-Hee Kim, Ja Seong Bae, Chan Kwon Jung
Modern Pathology.2017; 30(6): 810. CrossRef - BRAF-positive paucicellular variant of anaplastic carcinoma in the presence of tall cell variant papillary thyroid cancer
O. V. Dolzhansky, E. M. Paltseva, D. N. Khmelkova, F. A. Konovalov, I. V. Kanivets, A. V. Lavrov, D. V. Pyankov, S. A. Korostelev, O. A. Levendyuk, V. M. Pominalnaya, D. N. Fedorov
Arkhiv patologii.2017; 79(3): 27. CrossRef - A comparison of the clinicopathological features and prognoses of the classical and the tall cell variant of papillary thyroid cancer: a meta-analysis
Zeming Liu, Wen Zeng, Tianwen Chen, Yawen Guo, Chao Zhang, Chunping Liu, Tao Huang
Oncotarget.2017; 8(4): 6222. CrossRef - Clinical utility of TERT promoter mutations and ALK rearrangement in thyroid cancer patients with a high prevalence of the BRAF V600E mutation
Ja Seong Bae, Yourha Kim, Sora Jeon, Se Hee Kim, Tae Jung Kim, Sohee Lee, Min-Hee Kim, Dong Jun Lim, Youn Soo Lee, Chan Kwon Jung
Diagnostic Pathology.2016;[Epub] CrossRef - Tall cell variant of papillary thyroid carcinoma: current evidence on clinicopathologic features and molecular biology
Xiaofei Wang, Wenli Cheng, Chongqing Liu, Jingdong Li
Oncotarget.2016; 7(26): 40792. CrossRef - The Warthin-Like Variant of Papillary Thyroid Carcinoma: A Comparison with Classic Type in the Patients with Coexisting Hashimoto’s Thyroiditis
Min-kyung Yeo, Ja Seong Bae, Sohee Lee, Min-Hee Kim, Dong-Jun Lim, Youn Soo Lee, Chan Kwon Jung
International Journal of Endocrinology.2015; 2015: 1. CrossRef - BRAF Immunohistochemistry Using Clone VE1 is Strongly Concordant with BRAFV600E Mutation Test in Papillary Thyroid Carcinoma
Jung-Soo Pyo, Jin Hee Sohn, Guhyun Kang
Endocrine Pathology.2015; 26(3): 211. CrossRef - Pathologie de la thyroïde. Cas no 3. Carcinome papillaire de la thyroïde, variante à cellules hautes
Emmanuelle Leteurtre
Annales de Pathologie.2015; 35(5): 402. CrossRef
 PubReader
PubReader Cite this Article
Cite this Article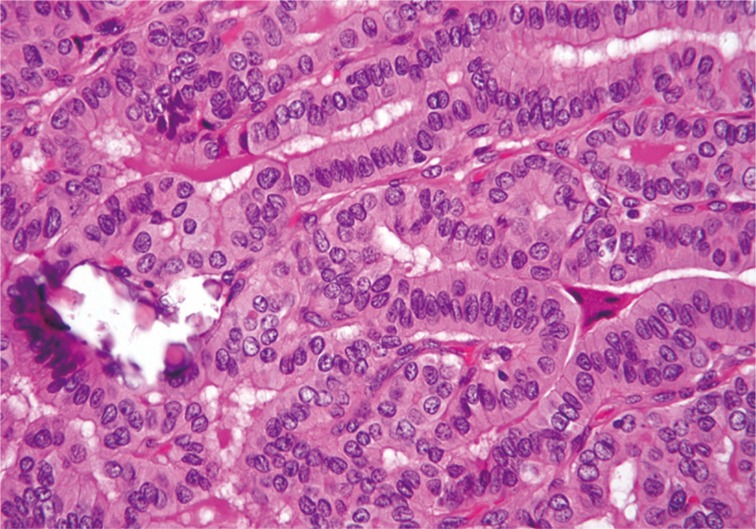
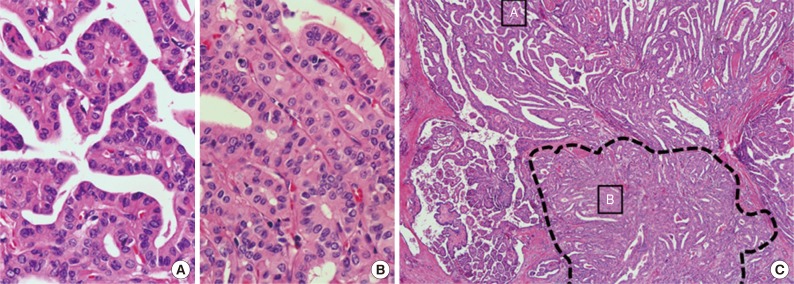


Fig. 1
Fig. 2
| Characteristic | Classic PTC (A) (%) | Classic PTC with TCF (B) (%) | TCVPTC (C) (%) | p-value (A vs B+C) | p-value (A vs B) | p-value (B vs C) |
|---|---|---|---|---|---|---|
| No. of cases | 111 | 65 | 49 | |||
| Mean age (yr) | 44.8 | 51.2 | 43.9 | NS | .011 | .46 |
| Age (yr) | NS | .012 | .02 | |||
| < 45 | 52 (46.8) | 18 (27.7) | 24 (49.0) | |||
| ≥ 45 | 59 (53.2) | 47 (72.3) | 25 (51.0) | |||
| Gender | NS | NS | NS | |||
| Female | 89 (80.2) | 51 (78.5) | 41 (83.7) | |||
| Male | 22 (19.8) | 14 (21.5) | 8 (16.3) | |||
| pT stage | .000 | .000 | NS | |||
| pT1 | 70 (63.1) | 20 (30.8) | 12 (24.5) | |||
| pT2 | 2 (1.8) | 1 (1.5) | 0 (0) | |||
| pT3 | 39 (35.1) | 44 (67.7) | 37 (75.5) | |||
| pT4 | 0 (0) | 0 (0) | 0 (0) | |||
| ETE | .000 | .000 | NS | |||
| Absent | 72 (64.9) | 21 (32.3) | 12 (24.5) | |||
| Present | 39 (35.1) | 44 (67.7) | 37 (75.5) | |||
| pN stage |
.000 | .007 | NS | |||
| pN0 | 66 (59.5) | 24 (38.1) | 13 (26.5) | |||
| pN1 | 45 (40.5) | 39 (61.9) | 36 (73.5) | |||
| Lateral LNM | .005 | .005 | NS | |||
| Absent | 107 (96.4) | 53 (84.1) | 43 (87.8) | |||
| Present | 4 (3.6) | 10 (15.9) | 6 (12.2) | |||
| BRAF mutation |
.002 | .018 | NS | |||
| Absent | 18 (16.2) | 2 (3.6) | 1 (2.4) | |||
| Present | 93 (83.8) | 54 (96.4) | 41 (97.6) |
| Characteristic | Classic PTC (A) (%) | Classic PTC with TCF (B) (%) | TCVPTC (C) (%) | p-value (A vs B+C) | p-value (A vs B) | p-value (B vs C) |
|---|---|---|---|---|---|---|
| No. of cases | 96 | 29 | 21 | |||
| Mean age (yr) | 45.3 | 52.8 | 46.5 | |||
| Age (yr) | .037 | .023 | NS | |||
| < 45 | 46 (47.9) | 7 (24.1) | 8 (38.1) | |||
| ≥ 45 | 50 (52.1) | 22 (75.9) | 13 (61.9) | |||
| Gender | NS | NS | NS | |||
| Female | 75 (78.1) | 24 (82.8) | 19 (90.5) | |||
| Male | 21 (21.9) | 5 (17.2) | 2 (9.5) | |||
| pT stage | .019 | NS | NS | |||
| pT1a | 67 (69.8) | 15 (51.7) | 10 (47.6) | |||
| pT3 | 29 (30.2) | 14 (48.3) | 11 (52.4) | |||
| pN stage |
.032 | NS | NS | |||
| pN0 | 61 (63.5) | 14 (50.0) | 8 (38.1) | |||
| pN1 | 35 (36.5) | 14 (50.0) | 13 (61.9) | |||
| Lateral LNM | NS | .041 | NS | |||
| Absent | 94 (97.9) | 25 (89.3) | 20 (95.2) | |||
| Present | 2 (2.1) | 3 (10.7) | 1 (4.8) | |||
| BRAF mutation |
.047 | NS | NS | |||
| Absent | 16 (16.7) | 1 (4.0) | 1 (5.3) | |||
| Present | 80 (83.3) | 24 (96.0) | 18 (94.7) |
| Characteristic | Classic PTC (A) (%) | Classic PTC with TCF (B) (%) | TCVPTC (C) (%) | p-value (A vs B+C) | p-value (A vs B) | p-value (B vs C) |
|---|---|---|---|---|---|---|
| No. of cases | 203 | 149 | 95 | |||
| Mean age | 47.6 | 51.0 | 47.1 | .000 | .000 | .017 |
| Age (yr) | .002 | .000 | .042 | |||
| < 45 | 95 (46.8) | 41 (27.5) | 38 (40.0) | |||
| ≥ 45 | 108 (53.2) | 108 (72.5) | 57 (60.0) | |||
| Gender | NS | NS | NS | |||
| Female | 164 (80.8) | 123 (82.6) | 82 (86.3) | |||
| Male | 39 (19.2) | 26 (17.4) | 13 (13.7) | |||
| Multifocality | NS | .040 | NS | |||
| Single | 111 (54.7) | 65 (43.6) | 49 (51.6) | |||
| Multiple | 92 (45.3) | 84 (56.4) | 46 (48.4) | |||
| pT stage | .000 | .000 | NS | |||
| pT1 | 126 (62.0) | 41 (27.5) | 23 (24.2) | |||
| pT2 | 3 (1.5) | 3 (2.0) | 0 (0) | |||
| pT3 | 74 (36.5) | 104 (69.8) | 71 (74.7) | |||
| pT4 | 0 (0) | 1 (0.7) | 1 (1.1) | |||
| ETE | .000 | .000 | NS | |||
| Absent | 129 (63.5) | 44 (29.5) | 23 (24.2) | |||
| Present | 74 (36.5) | 105 (70.5) | 72 (75.8) | |||
| pN stage |
.000 | .003 | NS | |||
| pN0 | 105 (51.7) | 51 (35.4) | 27 (29.0) | |||
| pN1 | 98 (48.3) | 93 (64.6) | 66 (71.0) | |||
| Lateral LNM | .003 | .002 | NS | |||
| Absent | 191 (94.1) | 121 (84.0) | 81 (87.1) | |||
| Present | 12 (5.9) | 23 (16.0) | 12 (12.9) | |||
| BRAF mutation |
.000 | .000 | NS | |||
| Absent | 34 (16.7) | 4 (3.1) | 3 (3.6) | |||
| Present | 169 (83.3) | 127 (96.9) | 80 (96.4) |
| Characteristic | Odds ratio (95% confidence interval) |
||
|---|---|---|---|
| A vs B+C | A vs B | B vs C | |
| Age (< 45 yr vs ≥ 45 yr) | 1.92 (1.22-3.01) |
2.39 (1.42-4.04) |
0.66 (0.36-1.23) |
| Gender (female vs male) | 0.88 (0.50-1.56) | 1.03 (0.54-1.95) | 0.63 (0.28-1.42) |
| Multifocality (unifocal vs multifocal) | 1.28 (0.83-1.97) | 1.50 (0.92-2.44) | 0.68 (0.38-1.21) |
| ETE (absent vs present) | 3.30 (2.13-5.10) |
2.81 (1.70-4.64) |
1.57 (0.82-2.98) |
| LN metastasis (absent vs present) | 1.84 (1.17-2.90) |
1.71 (1.01-2.90) |
1.10 (0.58-2.07) |
| BRAF mutation (absent vs present) | 5.14 (2.15-12.65) |
5.26 (1.75-15.76) |
0.82 (0.17-3.91) |
| Characteristic | Classic PTC (A) (%) | Classic PTC with TCF (B) (%) | TCVPTC (C) (%) | p-value (A vs B+C) | p-value (A vs B) | p-value (B vs C) |
|---|---|---|---|---|---|---|
| No. of cases | 164 | 67 | 43 | |||
| Mean age (yr) | 45.6 | 51.3 | 48.7 | .001 | .000 | NS |
| Age (yr) | .003 | .006 | NS | |||
| < 45 | 76 (46.3) | 18 (26.9) | 13 (30.2) | |||
| ≥ 45 | 88 (53.7) | 49 (73.1) | 30 (69.8) | |||
| Gender | .034 | NS | NS | |||
| Female | 132 (80.5) | 60 (89.6) | 39 (90.7) | |||
| Male | 32 (19.5) | 7 (10.4) | 4 (9.3) | |||
| Multifocality | .033 | .035 | NS | |||
| Single | 96 (58.5) | 29 (43.3) | 21 (48.8) | |||
| Multiple | 68 (41.5) | 38 (56.7) | 22 (51.2) | |||
| pT stage | .000 | .000 | NS | |||
| pT1a | 120 (73.2) | 28 (41.8) | 17 (39.5) | |||
| pT3 | 44 (26.8) | 39 (58.2) | 26 (60.5) | |||
| pN stage |
.014 | NS | NS | |||
| pN0 | 94 (57.3) | 29 (45.3) | 15 (36.6) | |||
| pN1 | 70 (42.7) | 35 (54.7) | 26 (63.4) | |||
| Lateral LNM | .045 | .007 | NS | |||
| Absent | 160 (97.6) | 57 (89.1) | 40 (97.6) | |||
| Present | 4 (2.4) | 7 (10.9) | 1 (2.4) | |||
| BRAF mutation |
.001 | .005 | NS | |||
| Absent | 29 (17.7) | 2 (3.3) | 2 (5.1) | |||
| Present | 135 (82.3) | 59 (96.7) | 37 (94.9) |
| Characteristic | Odds ratio (95% confidence interval) |
||
|---|---|---|---|
| A vs B+C | A vs B | B vs C | |
| Age < 45 yr | |||
| Gender (female vs male) | 0.68 (0.29-1.60) | 0.96 (0.35-2.58) | 0.44 (0.11-1.72) |
| Multifocality (unifocal vs multifocal) | 0.93 (0.45-1.89) | 1.44 (0.59-3.47) | 0.37 (0.13-1.04) |
| ETE (absent vs present) | 2.91 (1.45-5.85) |
2.99 (1.25-7.10) |
0.82 (0.28-2.38) |
| LN metastasis (absent vs present) | 2.95 (1.33-6.56) |
3.76 (1.25-11.30) |
0.53 (0.15-1.92) |
| BRAF mutation (absent vs present) | 16.58 (2.04-135.07) |
7.75E8 | 0.00 |
| Age ≥ 45 yr | |||
| Gender (female vs male) | 1.04 (0.48-2.28) | 1.06 (0.45-2.48) | 0.83 (0.30-2.29) |
| Multifocality (unifocal vs multifocal) | 1.48 (0.86-2.57) | 1.43 (0.79-2.61) | 0.96 (0.47-1.97) |
| ETE (absent vs present) | 3.62 (2.05-6.38) |
2.80 (1.50-5.21) |
2.18 (0.92-5.15) |
| LN metastasis (absent vs present) | 1.49 (0.84-2.63) | 1.31 (0.70-2.46) | 1.34 (0.64-2.84) |
| BRAF mutation (absent vs present) | 3.55 (1.27-9.97) |
3.33 (1.04-10.71) |
1.03 (0.17-6.15) |
TCF, tall cell features; TCVPTC, tall cell variant of papillary thyroid carcinoma; NS, not significant; ETE, extrathyrodial extension; LNM, lymph node metastasis. Two tumors of unknown pN stage (pNx) are excluded;
PTC, papillary thyroid carcinoma; TCF, tall cell features; TCVPTC, tall cell variant of papillary thyroid carcinoma; NS, not significant; LNM, lymph node metastasis. One tumors of unknown pN stage (pNx) are excluded;
TCF, tall cell features; TCVPTC, tall cell variant of papillary thyroid carcinoma; NS, not significant; ETE, extrathyrodial extension; LNM, lymph node metastasis. Seven tumors of unknown pN stage (pNx) are excluded;
A, classic papillary thyroid carcinoma; B, classic papillary thyroid carcinoma with tall cell features; C, tall cell variant of papillary thyroid carcinoma; ETE, extrathyrodial extension; LN, lymph node. p<.05.
TCF, tall cell features; TCVPTC, tall cell variant of papillary thyroid carcinoma; NS, not significant; LNM, lymph node metastasis. Five tumors of unknown pN stage (pNx) are excluded;
A, classic papillary thyroid carcinoma; B, classic papillary thyroid carcinoma with tall cell features; C, tall cell variant of papillary thyroid carcinoma; OR, odds ratio; CI, confidence interval; ETE, extrathyrodial extension; LN, lymph node. p<.05.

