 E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 56(2); 2022 > Article
-
Original Article
Fatty acid synthetase expression in triple-negative breast cancer -
Jin Hee Park1
 , Hye Seung Han1, So Dug Lim1, Wook Youn Kim1, Kyoung Sik Park2, Young Bum Yoo2, Seung Eun Lee1, Wan-Seop Kim1
, Hye Seung Han1, So Dug Lim1, Wook Youn Kim1, Kyoung Sik Park2, Young Bum Yoo2, Seung Eun Lee1, Wan-Seop Kim1 -
Journal of Pathology and Translational Medicine 2022;56(2):73-80.
DOI: https://doi.org/10.4132/jptm.2021.10.27
Published online: January 21, 2022
1Department of Pathology, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea
2Department of Surgery, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea
-
Corresponding Author: Seung Eun Lee, MD, PhD, Department of Pathology, Konkuk University Medical Center, Konkuk University School of Medicine, 120-1 Neungdong-ro, Gwangjin-gu, Seoul 05030, Korea, Tel: +82-2-2030-5644, Fax: +82-2-2030-5629, E-mail: 20150063@kuh.ac.kr
Corresponding Author: Wan-Seop Kim, MD, PhD, Department of Pathology, Konkuk University Medical Center, Konkuk University School of Medicine, 120-1 Neungdong-ro, Gwangjin-gu, Seoul 05030, Korea, Tel: +82-2-2030-5642, Fax: +82-2-2030-5629, E-mail: wskim@kuh.ac.kr
© 2022 The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Background
- Triple-negative breast cancer (TNBC) has a relatively poor prognosis. Research has identified potential metabolic targets, including fatty acid metabolism, in TNBC. The absence of effective target therapies for TNBC led to exploration of the role of fatty acid synthetase (FASN) as a potential target for TNBC therapy. Here, we analyzed the expression of FASN, a representative lipid metabolism–related protein, and investigated the association between FASN expression and Ki-67 and the programmed death ligand 1 (PD-L1) biomarkers in TNBC.
-
Methods
- Immunohistochemical expression of FASN was analyzed in 166 patients with TNBC. For analytical purposes, patients with 0–1+ FASN staining were grouped as low-grade FASN and patients with 2–3+ FASN staining as high-grade FASN.
-
Results
- FASN expression was observed in 47.1% of TNBC patients. Low and high expression of FASN was identified in 75.9% and 24.1%, respectively, and no statistically significant difference was found in T category, N category, American Joint Committee on Cancer stage, or recurrence rate between the low and high-FASN expression groups. Ki-67 proliferation level was significantly different between the low and high-FASN expression groups. FASN expression was significantly related to Ki-67 as the level increased. There was no significant difference in PD-L1 positivity between the low- and high-FASN expression groups.
-
Conclusions
- We identified FASN expression in 166 TNBC patients. The Ki-67 proliferation index was positively correlated with FASN level, indicating higher proliferation activity as FASN increases. However, there was no statistical association with PD-L1 SP142, the currently FDA-approved assay, or FASN expression level.
- Among ER- and HER-2–negative breast cancer patients, 166 patients who could be tracked and whose paraffin embedded tissue blocks were in good condition were enrolled in the study. Patient clinical records were used in a retrospective manner to identify clinical information including age, immunohistochemical study, TNM stage, recurrence, chemotherapy, and radiation therapy. We also wanted to quantify the degree of expression and correlate it with clinical information through immunostaining of FASN.
- Patient selection and clinicopathologic evaluation
- From January 2012 to December 2018, 166 TNBC patients who underwent primary breast cancer surgical resection at Konkuk University Medical Center (KUMC) Seoul, Korea, were analyzed. Clinicopathological information was obtained by reviewing medical records and hematoxylin and eosin (H&E)–stained sections. The TNBC histopathological data were determined by histological subtype, category T, category N, American Joint Committee on Cancer (AJCC) stage, and Bloom-Richardson histological grade.
- Tissue microarray
- All 166 H&E-stained slides were reviewed, and the most representative part of each was selected. Two 3 mm tissue cores derived from representative tumors of formalin-fixed paraffin-embedded tissue blocks were collected. An on-slide control tissue (tonsillar tissue) was used.
- Immunohistochemistry
- Immunohistochemistry (IHC) was performed using a Ventana Discovery XT automated slide stainer (Ventana Medical Systems, Tucson, AZ, USA), following antigen retrieval with Cell Conditioning 1 (CC1; citrate buffer pH 6.0, Ventana Medical System) at 37°C for 32 minutes. This was followed by a standard Ventana signal amplification and counterstaining with hematoxylin. Slides were mounted and examined by light microscopy. Appropriate positive and negative controls for IHC were included. We used anti-fatty acid synthase antibodies (Abcam, Cambridge, UK) and SP142 antibodies (Ventana, Mannheim, Germany) in this study.
- Interpretation of IHC results
- All IHC markers were determined using light microscopy to assess the proportion and intensity of stained cells. In this study, we classified breast cancer phenotypes according to ER, PR, and HER-2 IHC results and Ki-67 [18]. ER and PR positivity were used to define a cutoff value of 1% positively-stained nuclei [19]. HER-2 staining was analyzed according to the American Society of Clinical Oncology (ASCO)/College of American Pathologists guidelines [20]. HER-2 expression was considered positive when strong (3+) membranous staining was observed, whereas cases with scores of 0 to 1+ were considered negative [10]. The results of immunohistochemical staining for lipid metabolism–related proteins were scored as previously described [21]. Briefly, FASN staining was considered positive when > 10% of the tumor cells were stained, and the intensity was scored from 0 to 3. For analytical purposes, patients with 0–1+ FASN staining were grouped as low-grade FASN and patients with 2–3+ FASN staining as high-grade FASN [15]. SP142 score was assessed as previously described [6].
- Statistical analysis
- Data analysis was performed using SPSS ver. 20.0 (IBM Corp., Armonk, NY, USA) for Windows. Chi-square and Fisher’s exact tests were used to assess continuous and categorical variables, respectively. Statistical significance was assumed at a p-value < .05. Kaplan-Meier survival curves and log-rank statistics were employed to evaluate the time interval to tumor metastasis and survival duration. A Cox proportional hazards model was used to assess the risk factors of shorter disease-free survival and overall survival.
MATERIALS AND METHODS
- Clinicopathological characteristics of TNBC
- A total of 166 TNBC patient results were analyzed in this study, and the clinicopathological characteristics are presented in Table 1. The median age at diagnosis was 51 years (range, 28 to 83 years). The major histologic type of TNBC in KUMC was invasive ductal carcinoma (92.8%), with eight carcinomas with medullary features, three pleomorphic carcinomas, and one metaplastic carcinoma. About 85% of the cases were histologic grade 3, and 66% of the cases were AJCC stage 2. Of these 166 patients, 10 (6.0%) received neoadjuvant chemotherapy, 154 (92.8%) received adjuvant chemotherapy, and 140 (84.3%) received radiation therapy. Among the 166 patients, 26 (15.7%) recurred during follow-up observation. The median time until recurrence was 13.5 months.
- Expression of FASN in TNBC
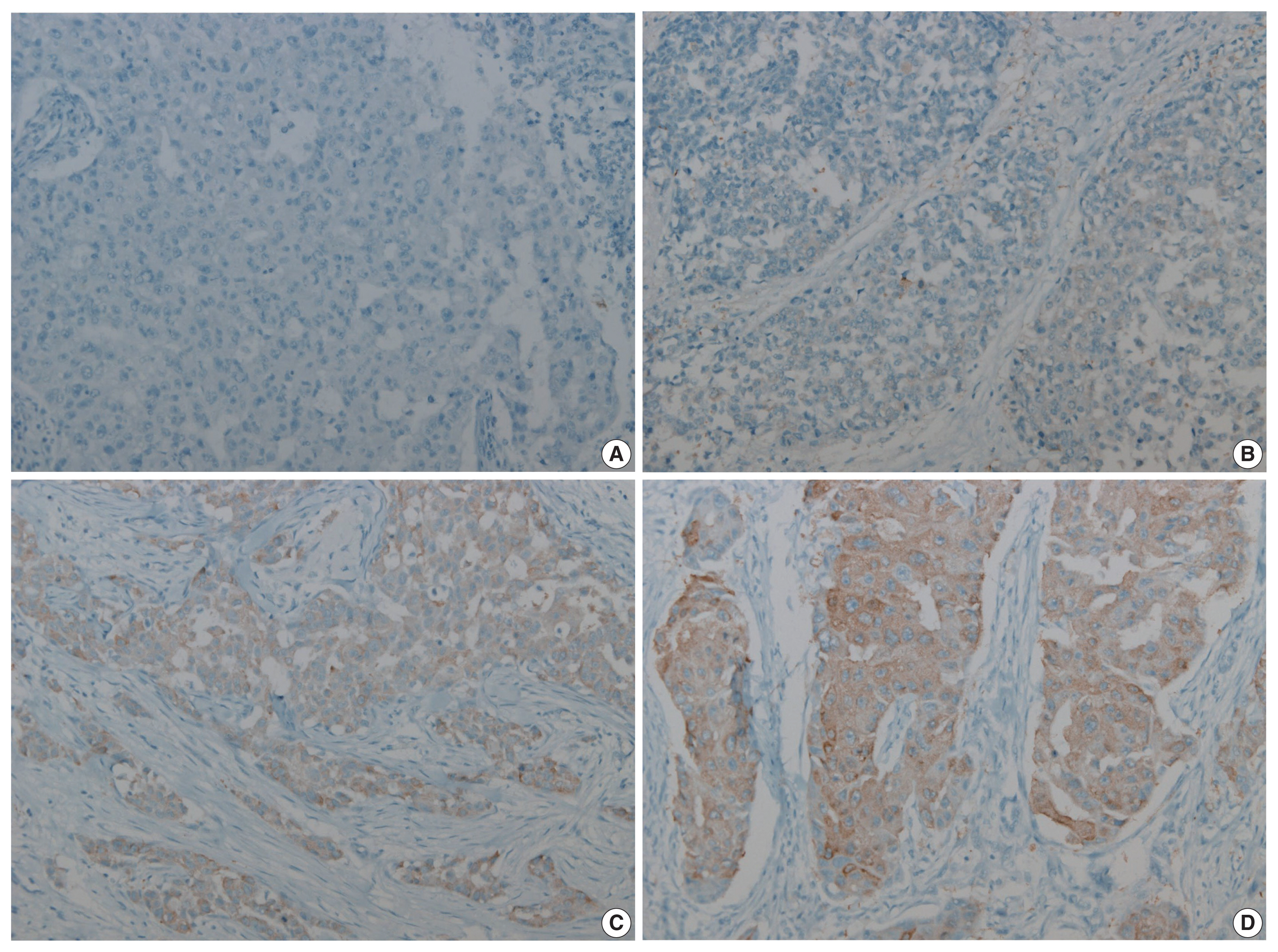
- Two pathologists independently observed and agreed to the final score values, and in some cases, IHC study was performed up to three times. The FASN expression levels in breast cancer patients were classified as grade 0, 1, 2, or 3 according to staining intensity. FASN expression was observed in 47.1% (95/166) of TNBC patients. Intensity grades of 1, 2, or 3 were seen in 33.1% (55/166), 13.3% (22/166), and 10.8% (18/166) of TNBC patients, respectively. Grades 0 and 1 were classified as the low-FASN group and grades 2 and 3 as the high-FASN group (Fig. 1). Low and high expression of FASN was identified in 75.9% (126/166) and 24.1% (40/166) of TNBC patients, respectively. Table 2 shows a comparison between the clinicopathological data of 40 patients with high FASN expression compared with that of 126 patients with low FASN expression. In the high-FASN expression group, more patients were younger than 50 years, while in the low-FASN group, more patients were older than 50 years old. The major cancer type was invasive ductal carcinoma and most were histologic grade 3; therefore, there was no association with high and low FASN expression. No statistically significant differences in T category, N category, AJCC stage, and recurrence rate were found between the high- and low-FASN expression groups.
- Correlation with immunohistochemical study of Ki-67
- The Ki-67 proliferation level was statistically different between the FASN low and high expression groups, with median Ki-67 levels of 60% (range, 40% to 80%) and 73% (range, 55% to 87%), respectively, using the Mann-Whitney U test (p = .003) (Table 3). The Spearman correlation coefficient was 0.257, indicating weak correlation between Ki-67 proliferation level and FASN expression level (p = .001).
- Correlation with PD-L1 SP142 IHC assay
- Two pathologists independently observed and agreed to the final score values. PD-L1 expression was assessed using the PD-L1 SP142 assay. Of the 166 cases, 94 available cases were used to perform IHC for PD-L1 SP142. At the 1% cutoff value, 52.6% (50/94) of cases were positive for PD-L1 SP142 in infiltrating immune cells (ICs). We analyzed the correlation between FASN expression level and percentage of PD-L1 SP142 positive infiltrating ICs, but no correlation was identified. There was no statistically significant PD-L1 SP142 positivity between the low- and high-FASN expression groups. A representative case of SP142 expression in the expression of high FASN was confirmed (Fig. 2).
RESULTS
- TNBC has no available special treatment other than chemotherapy after surgery, so early detection of recurrence through short-term follow-up observations will help patients with treatment and prognosis [22]. The development of interval breast cancer within the time interval between screening examinations has more adverse biological features, poorer survival outcomes, and is more highly associated with TNBC [23]. TNBC has high prevalence in young women under 50 and is more common in African Americans [24]. TNBC is known to have relatively poor prognosis compared to non-triple-negative breast cancer, most likely resulting from lack of special treatment methods such as hormone treatment or targeted treatment other than non-specific chemotherapy [25].
- The TNBC subtype was classified into four distinct types by Burstein et al. [26] and is being actively studied because of different prognoses and target therapies. Clinical results and treatment responses have changed depending on classification [27]. These inherent differences related to TNBC sub-classification have resulted in a renewed effort to identify driver mutations and more appropriate targeted treatment [28]. For potential therapy, activated progesterone receptor, platinum, tyrosine kinase inhibitor, PI3K/mTOR inhibitor, anti–PD-L1 inhibitors, and/or androgen receptor targeted PI3K inhibitors are thought to be possible [29]. Therefore, these treatments are being attempted in TNBC patients to identify whether they can benefit from a more appropriate and targeted treatment. We performed IHC for FASN, a representative lipid metabolism–related protein, as a candidate for a potential specific target in TNBC.
- FASN is a key lipogenic enzyme and is known to be overexpressed in various human cancers [30]. FASN is a lipid-producing enzyme that is expressed at low levels in normal human tissues but is reported to be highly expressed in breast, colon, prostate, ovarian, and endometrial cancers [11–14]. It has been hypothesized that useful indicators of prognosis can be found based on differences in the degree of expression between normal and cancer tissues, and patients with high FASN expression level have been reported to show lower disease-free survival and decreased survival rate [31]. High FASN expression was identified in 45% of TNBC cases [15] and high-FASN groups have been significantly associated with positive nodal status [15,16]. Therefore, FASN has emerged as a potential target, and FASN inhibitors are being evaluated in clinical trials [32]. First-generation (e.g., orlistat and cerulenin) and next-generation (TVB-3166 and TVB-2640) FASN-targeting drugs have been developed [33]. Adipophilin (ADP) and FASN are two lipid metabolism–related proteins of clinicopathological relevance for IHC expression in salivary duct carcinoma. ADP-positive expression was associated with the presence of prominent nuclear pleomorphism, high Ki-67, and poor prognosis [30].
- In this study, we evaluated the association of FASN expression between clinicopathological features, including PD-L1 SP142 expression, and further evaluated its usefulness as a biomarker in TNBC. FASN expression was observed in 47.1% (95/166) of TNBC patients in our study. Staining intensity grades of 1, 2, and 3 were found in 33.1% (55/166), 13.3% (22/166), and 10.8% (18/166) of TNBC patients, respectively. Low (grade 0,1) and high (grade 2,3) expression of FASN was identified in 75.9% (126/166) and 24.1% (40/166) of TNBC, respectively. However, we could not identify an association with lymph node stage or TNM stage [15].
- Ki-67 IHC is used as a proliferation marker in breast cancer and is a low-cost measurement method suitable for extensive use in clinical practice [34]. Higher Ki-67 level is associated with increased early recurrence and aggression, resulting in a lower patient survival rate [35]. In a Japanese study, when Ki-67 was greater than 10%, it was related with a high recurrence rate and low survival rate [36]. The Breast Cancer Working Group proposed guidelines for Ki-67 assessment in breast cancer and use of this potentially important marker based on current evidence [37]. Less than 5% of patients do not require chemotherapy, and more than 30% show chemotherapy indication. The ER negative case is referred to as insufficient evaluation for Ki-67 [37]. Another group reported that high Ki-67 expression (cutoff value of 30%) was correlated with early recurrence in luminal B/HER-2 negative breast cancer [38]. TNBC patients in the high Ki-67 group seem to benefit more from treatment with carboplatin [39]. The majority of TNBC cases has high Ki-67 expression level (≥ 20%), which is used as a proliferation factor [40]. In our study, 92.8% of cases had Ki-67 expression ≥ 20%. However, the Ki-67 proliferation level was statistically different between the FASN low and high expression groups. The median Ki-67 value of the low- and high-FASN expression groups was 60% (range, 40% to 80%) and 73% (range, 55% to 87%), respectively.
- In 2019, the FDA-approved atezolizumab (TECENTRIQ, Genentech Inc.) treatment in combination with paclitaxel was approved for TNBC patients whose PD-L1 stained tumor-infiltrating ICs were over 1% intensity [41]. PD-L1 is a cell membrane protein expressed in tumor cells and ICs [42]. PD-L1 expression is increased in TNBC and is a positive predictor of immunotherapy [43]. PD-L1 IHC using the VENTANA SP142 assay, the current FDA-approved assay, improved clinical outcome in atezolizumab plus nab-paclitaxel-treated patients [44]. In our study, we investigated the association between PD-L1 and FASN expression level and unfortunately identified no association.
- TNBC represents a small proportion of breast cancer subtypes but has the worst outcome [45]. Although this study was based on data from a small number of TNBC cases and short-term follow-up surveys, we included 166 TNBC patients in the study. More research on the expression of FASN on TNBC and its potential inhibitors will help identify new target treatments. Further research is needed on how FASN correlates with other factors in TNBC. In addition, further studies are required with a larger number of TNBC patients to investigate the specific role of FASN in TNBC and the possibility for FASN inhibition as a target treatment for TNBC.
- In conclusion, we showed FASN expression in TNBC patients and Ki-67 proliferation index to be positively correlated with FASN level, indicating higher proliferation activity as FASN increases. However, there was no statistical association with PD-L1 SP142, the currently FDA-approved assay, or FASN expression level.
DISCUSSION
Ethics Statement
The KUMC Institutional Review Board anonymized the archive data prior to the study and waived the requirement for prior consent (KUMC 2021-07-032).
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
Code Availability
Not applicable.
Author Contributions
Conceptualization: SEL, WSK. Data curation: KSP, YBY, JHP. Formal analysis: SEL, WYK. Funding acquisition: WSK. Investigation: JHP. Methodology: SEL. Supervision: WSK, HSH. Validation: SEL, SDL. Writing—original draft: JHP, SEL. Writing—review & editing: SEL, WSK, JHP. Approval of final manuscript: all authors.
Conflicts of Interest
The authors declare that they have no potential conflicts of interest.
Funding Statement
This research was supported by the Bio & Medical Technology Development Program of the National Research Foundation (NRF) funded by the Korean government (Ministry of Science and ICT) (No. 2019M3E5D3073475).

| Low (n = 126) | High (n = 40) | p-value | |
|---|---|---|---|
| Age (yr) | .018a | ||
| < 50 | 58 (46.0) | 27 (67.5) | |
| > 50 | 68 (54.0) | 13 (32.5) | |
| Histologic type | .319b | ||
| IDC, NOS | 116 (92.1) | 38 (95.0) | |
| Carcinoma with medullary feature | 7 (5.6) | 1 (2.5) | |
| Pleomorphic carcinoma | 3 (2.4) | 0 | |
| Metaplastic carcinoma | 0 | 1 (2.5) | |
| T category | .080b | ||
| 1 | 44 (66.7) | 22 (33.3) | |
| 2 | 73 (83.0) | 15 (17.0) | |
| 3 | 8 (72.7) | 3 (27.3) | |
| 4 | 1 (100) | 0 | |
| N category | .614b | ||
| 0 | 79 (72.5) | 30 (27.5) | |
| 1 | 33 (82.5) | 7 (17.5) | |
| 2 | 8 (88.9) | 1 (11.1) | |
| 3 | 2 (50.0) | 2 (50.0) | |
| AJCC stage | .075b | ||
| 1 | 18 (54.5) | 15 (45.5) | |
| 2 | 91 (82.7) | 19 (17.3) | |
| 3 | 13 (68.4) | 6 (31.6) | |
| N/A | 4 (100) | 0 | |
| Histologic grade | .097a | ||
| 2 | 15 (11.9) | 9 (22.5) | |
| 3 | 111 (88.1) | 31 (77.5) | |
| Neoadjuvant CTx | 10 (7.94) | 0 | .120b |
| CTx | 119 (94.4) | 35 (87.5) | .140a |
| RTx | 105 (83.3) | 35 (87.5) | .528a |
| Recur | 23 (18.3) | 3 (7.5) | .135b |
| Mann-Whitney U test | Ki-67 | p-value |
|---|---|---|
| Low FASN, median (range) | 60 (40–80) | .003 |
| High FASN, median (range) | 72.75 (55.13–87.7) | |
| Spearman’s correlation | ||
| FASN expression level | ρ = 0.257 | .001 |
- 1. Gluz O, Liedtke C, Gottschalk N, Pusztai L, Nitz U, Harbeck N. Triple-negative breast cancer: current status and future directions. Ann Oncol 2009; 20: 1913-27. ArticlePubMed
- 2. Diana A, Franzese E, Centonze S, et al. Triple-negative breast cancers: systematic review of the literature on molecular and clinical features with a focus on treatment with innovative drugs. Curr Oncol Rep 2018; 20: 76.ArticlePubMedPDF
- 3. Lee KK, Kim JY, Jung JH, Park JY, Park HY. Clinicopathological feature and recurrence pattern of triple negative breast cancer. J Korean Surg Soc 2010; 79: 14-9. Article
- 4. Bianchini G, Balko JM, Mayer IA, Sanders ME, Gianni L. Triple-negative breast cancer: challenges and opportunities of a heterogeneous disease. Nat Rev Clin Oncol 2016; 13: 674-90. ArticlePubMedPMCPDF
- 5. Marotti JD, de Abreu FB, Wells WA, Tsongalis GJ. Triple-negative breast cancer: next-generation sequencing for target identification. Am J Pathol 2017; 187: 2133-8. PubMed
- 6. Lee SE, Park HY, Lim SD, Han HS, Yoo YB, Kim WS. Concordance of programmed death-ligand 1 expression between SP142 and 22C3/SP263 assays in triple-negative breast cancer. J Breast Cancer 2020; 23: 303-13. ArticlePubMedPMCPDF
- 7. Rugo HS, Loi S, Adams S, et al. PD-L1 immunohistochemistry assay comparison in atezolizumab plus nab-paclitaxel-treated advanced triple-negative breast cancer. J Natl Cancer Inst 2021; 113: 1733-43. ArticlePubMedPMCPDF
- 8. Sun X, Wang M, Wang M, et al. Metabolic reprogramming in triple-negative breast cancer. Front Oncol 2020; 10: 428.ArticlePubMedPMC
- 9. Gong Y, Ji P, Yang YS, et al. Metabolic-pathway-based subtyping of triple-negative breast cancer reveals potential therapeutic targets. Cell Metab 2021; 33: 51-64. ArticlePubMed
- 10. Cha YJ, Kim HM, Koo JS. Expression of lipid metabolism-related proteins differs between invasive lobular carcinoma and invasive ductal carcinoma. Int J Mol Sci 2017; 18: 232.ArticlePubMedPMC
- 11. Sebastiani V, Visca P, Botti C, et al. Fatty acid synthase is a marker of increased risk of recurrence in endometrial carcinoma. Gynecol Oncol 2004; 92: 101-5. ArticlePubMed
- 12. Wang Y, Kuhajda FP, Li JN, et al. Fatty acid synthase (FAS) expression in human breast cancer cell culture supernatants and in breast cancer patients. Cancer Lett 2001; 167: 99-104. ArticlePubMed
- 13. Yang Y, Morin PJ, Han WF, et al. Regulation of fatty acid synthase expression in breast cancer by sterol regulatory element binding protein-1c. Exp Cell Res 2003; 282: 132-7. ArticlePubMed
- 14. Kusakabe T, Nashimoto A, Honma K, Suzuki T. Fatty acid synthase is highly expressed in carcinoma, adenoma and in regenerative epithelium and intestinal metaplasia of the stomach. Histopathology 2002; 40: 71-9. ArticlePubMedPDF
- 15. Giro-Perafita A, Sarrats A, Perez-Bueno F, et al. Fatty acid synthase expression and its association with clinico-histopathological features in triple-negative breast cancer. Oncotarget 2017; 8: 74391-405. ArticlePubMedPMC
- 16. Jiang W, Xing XL, Zhang C, et al. MET and FASN as prognostic biomarkers of triple negative breast cancer: a systematic evidence landscape of clinical study. Front Oncol 2021; 11: 604801.ArticlePubMedPMC
- 17. Flores FH, Vinas G, Oliveras G, et al. Triple negative breast cancer: clinicopathologic characteristics and fatty acid synthase (FASN) expression as a potential target. Ann Oncol 2014; 25(Suppl 4):IV60.Article
- 18. Goldhirsch A, Wood WC, Coates AS, et al. Strategies for subtypes: dealing with the diversity of breast cancer: highlights of the St. Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2011. Ann Oncol 2011; 22: 1736-47. ArticlePubMedPMC
- 19. Hammond ME, Hayes DF, Dowsett M, et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for immunohistochemical testing of estrogen and progesterone receptors in breast cancer (unabridged version). Arch Pathol Lab Med 2010; 134: e48-72. PubMed
- 20. Wolff AC, Hammond ME, Schwartz JN, et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for human epidermal growth factor receptor 2 testing in breast cancer. Arch Pathol Lab Med 2007; 131: 18-43. PubMed
- 21. Sarrio D, Rodriguez-Pinilla SM, Hardisson D, Cano A, Moreno-Bueno G, Palacios J. Epithelial-mesenchymal transition in breast cancer relates to the basal-like phenotype. Cancer Res 2008; 68: 989-97. ArticlePubMedPDF
- 22. Ma D, Jiang YZ, Xiao Y, et al. Integrated molecular profiling of young and elderly patients with triple-negative breast cancer indicates different biological bases and clinical management strategies. Cancer 2020; 126: 3209-18. ArticlePubMedPDF
- 23. Li J, Holm J, Bergh J, et al. Breast cancer genetic risk profile is differentially associated with interval and screen-detected breast cancers. Ann Oncol 2015; 26: 517-22. ArticlePubMed
- 24. Dietze EC, Sistrunk C, Miranda-Carboni G, O’Regan R, Seewaldt VL. Triple-negative breast cancer in African-American women: disparities versus biology. Nat Rev Cancer 2015; 15: 248-54. ArticlePubMedPMCPDF
- 25. Foulkes WD, Smith IE, Reis-Filho JS. Triple-negative breast cancer. N Engl J Med 2010; 363: 1938-48. ArticlePubMed
- 26. Burstein MD, Tsimelzon A, Poage GM, et al. Comprehensive genomic analysis identifies novel subtypes and targets of triple-negative breast cancer. Clin Cancer Res 2015; 21: 1688-98. ArticlePubMedPDF
- 27. Garrido-Castro AC, Lin NU, Polyak K. Insights into molecular classifications of triple-negative breast cancer: improving patient selection for treatment. Cancer Discov 2019; 9: 176-98. ArticlePubMedPMCPDF
- 28. D’Ippolito E, Iorio MV. MicroRNAs and triple negative breast cancer. Int J Mol Sci 2013; 14: 22202-20. ArticlePubMedPMC
- 29. Le Du F, Eckhardt BL, Lim B, et al. Is the future of personalized therapy in triple-negative breast cancer based on molecular subtype? Oncotarget 2015; 6: 12890-908. ArticlePubMedPMC
- 30. Hirai H, Tada Y, Nakaguro M, et al. The clinicopathological significance of the adipophilin and fatty acid synthase expression in salivary duct carcinoma. Virchows Arch 2020; 477: 291-9. ArticlePubMedPMCPDF
- 31. Kim S, Lee Y, Koo JS. Differential expression of lipid metabolism-related proteins in different breast cancer subtypes. PLoS One 2015; 10: e0119473.ArticlePubMedPMC
- 32. Giro-Perafita A, Rabionet M, Planas M, et al. EGCG-derivative G28 shows high efficacy inhibiting the mammosphere-forming capacity of sensitive and resistant TNBC models. Molecules 2019; 24: 1027.ArticlePubMedPMC
- 33. Wang W, Bai L, Li W, Cui J. The lipid metabolic landscape of cancers and new therapeutic perspectives. Front Oncol 2020; 10: 605154.ArticlePubMedPMC
- 34. Mrklic I, Capkun V, Pogorelic Z, Tomic S. Prognostic value of Ki-67 proliferating index in triple negative breast carcinomas. Pathol Res Pract 2013; 209: 296-301. ArticlePubMed
- 35. Ahmed ST, Ahmed AM, Musa DH, Sulayvani FK, Al-Khyatt M, Pity IS. Proliferative index (Ki67) for prediction in breast duct carcinomas. Asian Pac J Cancer Prev 2018; 19: 955-9. PubMedPMC
- 36. Miyashita M, Ishida T, Ishida K, et al. Histopathological subclassification of triple negative breast cancer using prognostic scoring system: five variables as candidates. Virchows Arch 2011; 458: 65-72. ArticlePubMedPDF
- 37. Nielsen TO, Leung SC, Rimm DL, et al. Assessment of Ki67 in breast cancer: updated recommendations from the international Ki67 in breast cancer working group. J Natl Cancer Inst 2021; 113: 808-19. PubMed
- 38. Zong Y, Zhu L, Wu J, et al. Progesterone receptor status and Ki-67 index may predict early relapse in luminal B/HER2 negative breast cancer patients: a retrospective study. PLoS One 2014; 9: e95629.ArticlePubMedPMC
- 39. Wang W, Wu J, Zhang P, et al. Prognostic and predictive value of Ki-67 in triple-negative breast cancer. Oncotarget 2016; 7: 31079-87. ArticlePubMedPMC
- 40. Pan Y, Yuan Y, Liu G, Wei Y. P53 and Ki-67 as prognostic markers in triple-negative breast cancer patients. PLoS One 2017; 12: e0172324.ArticlePubMedPMC
- 41. Mavratzas A, Seitz J, Smetanay K, Schneeweiss A, Jager D, Fremd C. Atezolizumab for use in PD-L1-positive unresectable, locally advanced or metastatic triple-negative breast cancer. Future Oncol 2020; 16: 4439-53. ArticlePubMed
- 42. Dong H, Strome SE, Salomao DR, et al. Tumor-associated B7-H1 promotes T-cell apoptosis: a potential mechanism of immune evasion. Nat Med 2002; 8: 793-800. ArticlePubMedPDF
- 43. Peg V, Lopez-Garcia MA, Comerma L, et al. PD-L1 testing based on the SP142 antibody in metastatic triple-negative breast cancer: summary of an expert round-table discussion. Future Oncol 2021; 17: 1209-18. ArticlePubMed
- 44. Li Y, Vennapusa B, Chang CW, et al. Prevalence study of PD-L1 SP142 assay in metastatic triple-negative breast cancer. Appl Immunohistochem Mol Morphol 2021; 29: 258-64. ArticlePubMed
- 45. Al-Jussani GN, Dabbagh TZ, Al-Rimawi D, Sughayer MA. Expression of PD-L1 using SP142 CDx in triple negative breast cancer. Ann Diagn Pathol 2021; 51: 151703.ArticlePubMed
REFERENCES
Figure & Data
References
Citations
- Lipid metabolism involved in progression and drug resistance of breast cancer
Wenxiang Fu, Aijun Sun, Huijuan Dai
Genes & Diseases.2025; 12(4): 101376. CrossRef - Unveiling the impact of lipid metabolism on triple-negative breast cancer growth and treatment options
Xin-xian Cai, Zhe-zhong Zhang, Xiao-xiao Yang, Wen-rui Shen, Liu-wei Yuan, Xi Ding, Ying Yu, Wen-yu Cai
Frontiers in Oncology.2025;[Epub] CrossRef - Protein biomarkers for diagnosis of breast cancer
Emeka Eze Joshua Iweala, Doris Nnenna Amuji, Faith Chinasaokwu Nnaji
Scientific African.2024; 25: e02308. CrossRef - Microarray analysis points to LMNB1 and JUN as potential target genes for predicting metastasis promotion by etoposide in colorectal cancer
Jiafei Liu, Hongjie Yang, Peng Li, Yuanda Zhou, Zhichun Zhang, Qingsheng Zeng, Xipeng Zhang, Yi Sun
Scientific Reports.2024;[Epub] CrossRef - The signature of extracellular vesicles in hypoxic breast cancer and their therapeutic engineering
Baiheng Zhu, Kehao Xiang, Tanghua Li, Xin Li, Fujun Shi
Cell Communication and Signaling.2024;[Epub] CrossRef - NFYA promotes malignant behavior of triple-negative breast cancer in mice through the regulation of lipid metabolism
Nobuhiro Okada, Chihiro Ueki, Masahiro Shimazaki, Goki Tsujimoto, Susumu Kohno, Hayato Muranaka, Kiyotsugu Yoshikawa, Chiaki Takahashi
Communications Biology.2023;[Epub] CrossRef - Role of EGFR and FASN in breast cancer progression
Suchi Chaturvedi, Mainak Biswas, Sushabhan Sadhukhan, Avinash Sonawane
Journal of Cell Communication and Signaling.2023; 17(4): 1249. CrossRef - Bioinformatics Method Was Used to Analyze the Highly Expressed Gene FAM83A of Breast Cancer in Young Women
Yongzhe Tang, Hao Wang, Qi He, Yuanyuan Chen, Jie Wang, Fahd Abd Algalil
Applied Bionics and Biomechanics.2022; 2022: 1. CrossRef - NCAPH promotes proliferation as well as motility of breast cancer cells by activating the PI3K/AKT pathway
Ting Zhang, Peng Li, Wanying Guo, Qipeng Liu, Weiqiang Qiao, Miao Deng
Physiology International.2022;[Epub] CrossRef
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-
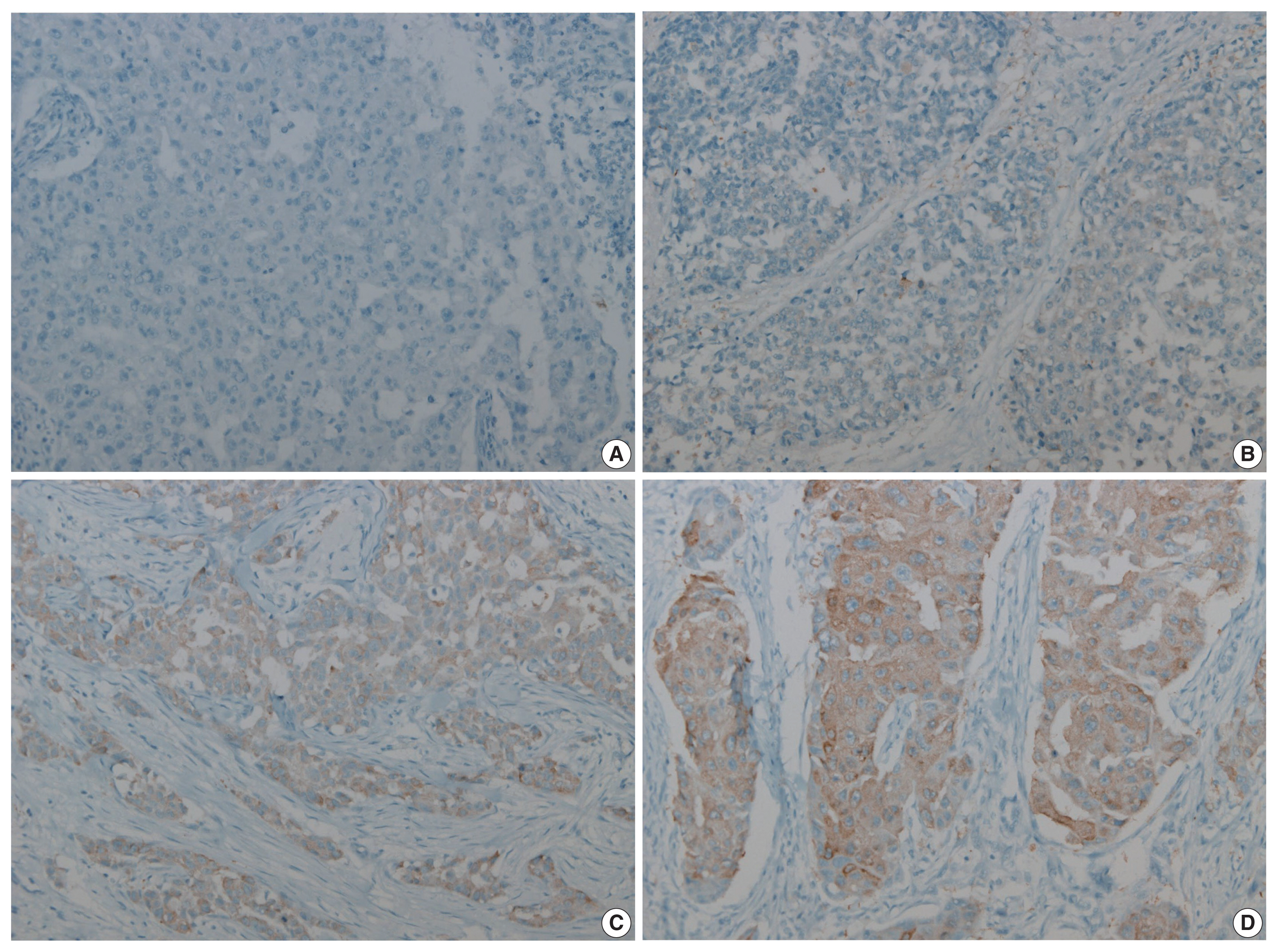
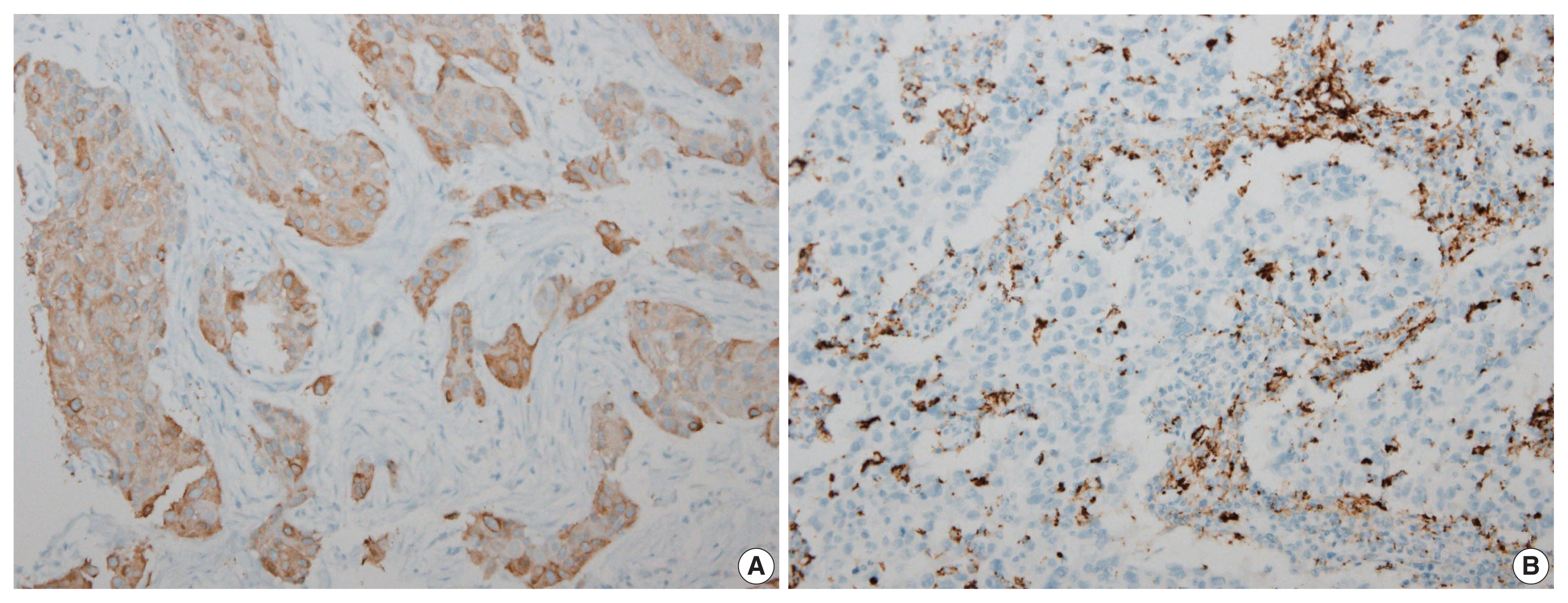


Fig. 1
Fig. 2
| Characteristics | No. of patients |
|---|---|
| Age (yr) | 51 (28–83) |
| Age (yr) | |
| ≤ 50 | 81 (48.8) |
| > 50 | 85 (51.2) |
| Histologic type | |
| IDC, NOS | 154 (92.8) |
| Carcinoma with medullary feature | 8 (4.8) |
| Pleomorphic carcinoma | 3 (1.8) |
| Metaplastic carcinoma | 1 (0.6) |
| T category | |
| 1 | 66 (39.8) |
| 2 | 88 (53.0) |
| 3 | 11 (6.6) |
| 4 | 1 (0.6) |
| N category | |
| 0 | 109 (65.7) |
| 1 | 40 (24.1) |
| 2 | 9 (5.4) |
| 3 | 4 (2.4) |
| NA | 4 (2.4) |
| Histologic grade | |
| 1 | 0 |
| 2 | 24 (14.5) |
| 3 | 142 (85.5) |
| AJCC stage | |
| 1 | 33 (19.9) |
| 2 | 110 (66.3) |
| 3 | 19 (11.4) |
| N/A | 4 (2.4) |
| Neoadjuvant CTx | |
| Yes | 10 (6.0) |
| No | 156 (94.0) |
| CTx | |
| Yes | 154 (92.8) |
| No | 12 (7.2) |
| RTx | |
| Yes | 140 (84.3) |
| No | 26 (15.7) |
| Recur | |
| Yes | 26 (15.7) |
| No | 140 (84.3) |
| Low (n = 126) | High (n = 40) | p-value | |
|---|---|---|---|
| Age (yr) | .018 | ||
| < 50 | 58 (46.0) | 27 (67.5) | |
| > 50 | 68 (54.0) | 13 (32.5) | |
| Histologic type | .319 | ||
| IDC, NOS | 116 (92.1) | 38 (95.0) | |
| Carcinoma with medullary feature | 7 (5.6) | 1 (2.5) | |
| Pleomorphic carcinoma | 3 (2.4) | 0 | |
| Metaplastic carcinoma | 0 | 1 (2.5) | |
| T category | .080 | ||
| 1 | 44 (66.7) | 22 (33.3) | |
| 2 | 73 (83.0) | 15 (17.0) | |
| 3 | 8 (72.7) | 3 (27.3) | |
| 4 | 1 (100) | 0 | |
| N category | .614 | ||
| 0 | 79 (72.5) | 30 (27.5) | |
| 1 | 33 (82.5) | 7 (17.5) | |
| 2 | 8 (88.9) | 1 (11.1) | |
| 3 | 2 (50.0) | 2 (50.0) | |
| AJCC stage | .075 | ||
| 1 | 18 (54.5) | 15 (45.5) | |
| 2 | 91 (82.7) | 19 (17.3) | |
| 3 | 13 (68.4) | 6 (31.6) | |
| N/A | 4 (100) | 0 | |
| Histologic grade | .097 | ||
| 2 | 15 (11.9) | 9 (22.5) | |
| 3 | 111 (88.1) | 31 (77.5) | |
| Neoadjuvant CTx | 10 (7.94) | 0 | .120 |
| CTx | 119 (94.4) | 35 (87.5) | .140 |
| RTx | 105 (83.3) | 35 (87.5) | .528 |
| Recur | 23 (18.3) | 3 (7.5) | .135 |
| Mann-Whitney U test | Ki-67 | p-value |
|---|---|---|
| Low FASN, median (range) | 60 (40–80) | .003 |
| High FASN, median (range) | 72.75 (55.13–87.7) | |
| Spearman’s correlation | ||
| FASN expression level | ρ = 0.257 | .001 |
Values are presented as median (interquartile range) or number (%). TNBC, triple-negative breast cancer; IDC, invasive ductal carcinoma; NOS, not otherwise specified; NA, not applicable; AJCC, American Joint Committee on Cancer; CTx, chemotherapy; RTx, radiation therapy.
FASN, fatty acid synthetase; IDC, invasive ductal carcinoma; NOS, not otherwise specified; N/A, not applicable; AJCC, American Joint Committee on Cancer; CTx, chemotherapy; RTx, radiation therapy. Linear by linear association; Fisher’s exact test.
FASN, fatty acid synthetase.

