 E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 56(4); 2022 > Article
-
Case Study
Clinically undetected plasmacytoid urothelial carcinoma of the urinary bladder with non-mass-forming metastases in multiple organs: an autopsy case -
Yuya Asano1,2
 , Kosuke Miyai2,3, Shinya Yoshimatsu4, Makoto Sasaki5, Katsunori Ikewaki5, Susumu Matsukuma2,4
, Kosuke Miyai2,3, Shinya Yoshimatsu4, Makoto Sasaki5, Katsunori Ikewaki5, Susumu Matsukuma2,4 -
Journal of Pathology and Translational Medicine 2022;56(4):217-224.
DOI: https://doi.org/10.4132/jptm.2022.03.15
Published online: May 3, 2022
1National Defense Medical College, Saitama, Japan
2Department of Pathology and Laboratory Medicine, National Defense Medical College, Saitama, Japan
3Department of Pathology, Japan Self-Defense Forces Central Hospital, Tokyo, Japan
4Department of Laboratory Medicine, National Defense Medical College Hospital, Saitama, Japan
5Department of Anti-Aging and Vascular Medicine, National Defense Medical College, Saitama, Japan
- Corresponding Author: Kosuke Miyai, MD, PhD, Department of Pathology, Japan Self-Defense Forces Central Hospital, 1-2-24 Ikejiri, Setagaya-ku, Tokyo 154-8532, Japan, Tel: +81-3-3411-0151, Fax: +81-4-2996-5193, E-mail: mykusu228@nifty.com
© 2022 The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
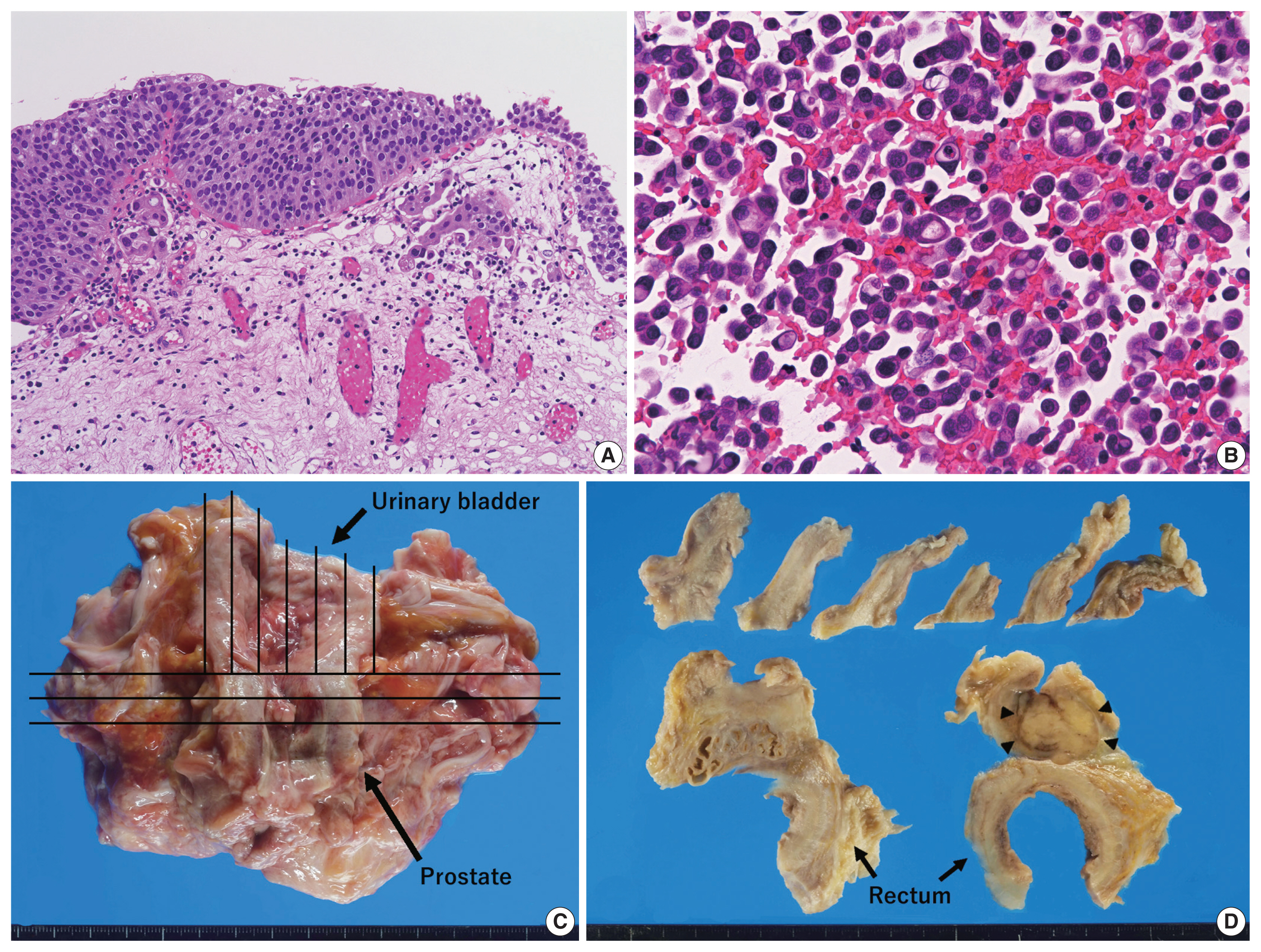

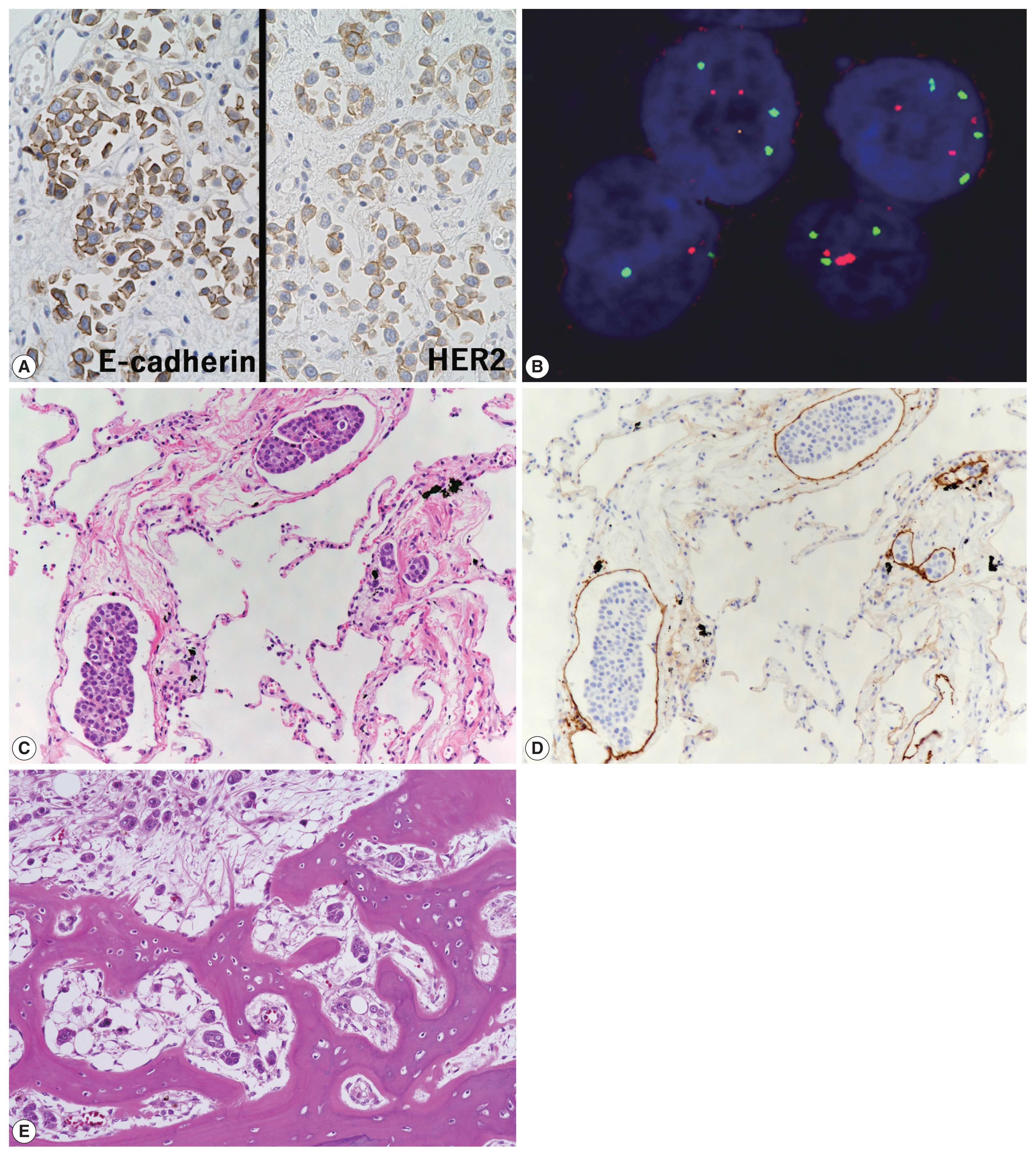
Figure & Data
References
Citations
- Plasmacytoid Urothelial Carcinoma with Initial Presentation as a Secondary
Prostatic Tumor: Diagnostic Pitfalls
and Literature Review
丰锦 李
Advances in Clinical Medicine.2026; 16(02): 1264. CrossRef - Severe Rectal Stenosis as the First Clinical Appearance of a Metastasis Originating from the Bladder: A Case Report and Literature Review
Claudiu Daha, Eugen Brătucu, Ioan Burlănescu, Virgiliu-Mihail Prunoiu, Hortensia-Alina Moisă, Ștefania Ariana Neicu, Laurențiu Simion
Life.2025; 15(5): 682. CrossRef - Carcinomatous Meningitis and Hydrocephalus in Plasmacytoid Urothelial Carcinoma of the Urinary Bladder With Extremely Elevated CA19-9 Levels
Fumiaki Henmi, Kayako Ukai, Atsuhito Nakayama, Yutaka Takazawa, Yoshikazu Uesaka
Cureus.2024;[Epub] CrossRef - Current Advances in the Management of Nonurothelial Subtypes of Bladder Cancer
Evangelia Vlachou, Burles Avner Johnson, Ezra Baraban, Rosa Nadal, Jean Hoffman-Censits
American Society of Clinical Oncology Educational Book.2024;[Epub] CrossRef - Plasmacytoid urothelial carcinoma: a multidisciplinary approach to the diagnosis and management
Marcus Zorovich, Jude Khatib, Aysha Mubeen, Katie Gardner, Nayana Patel
Abdominal Radiology.2024; 51(3): 1397. CrossRef - Divergent Histology in Bladder Cancer: What We Need to Know?
Shashank Agrawal, Arun Ramdas Menon, Ginil Kumar Pooleri
UroCancer Clinics of India.2024; 2(2): 100. CrossRef
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-
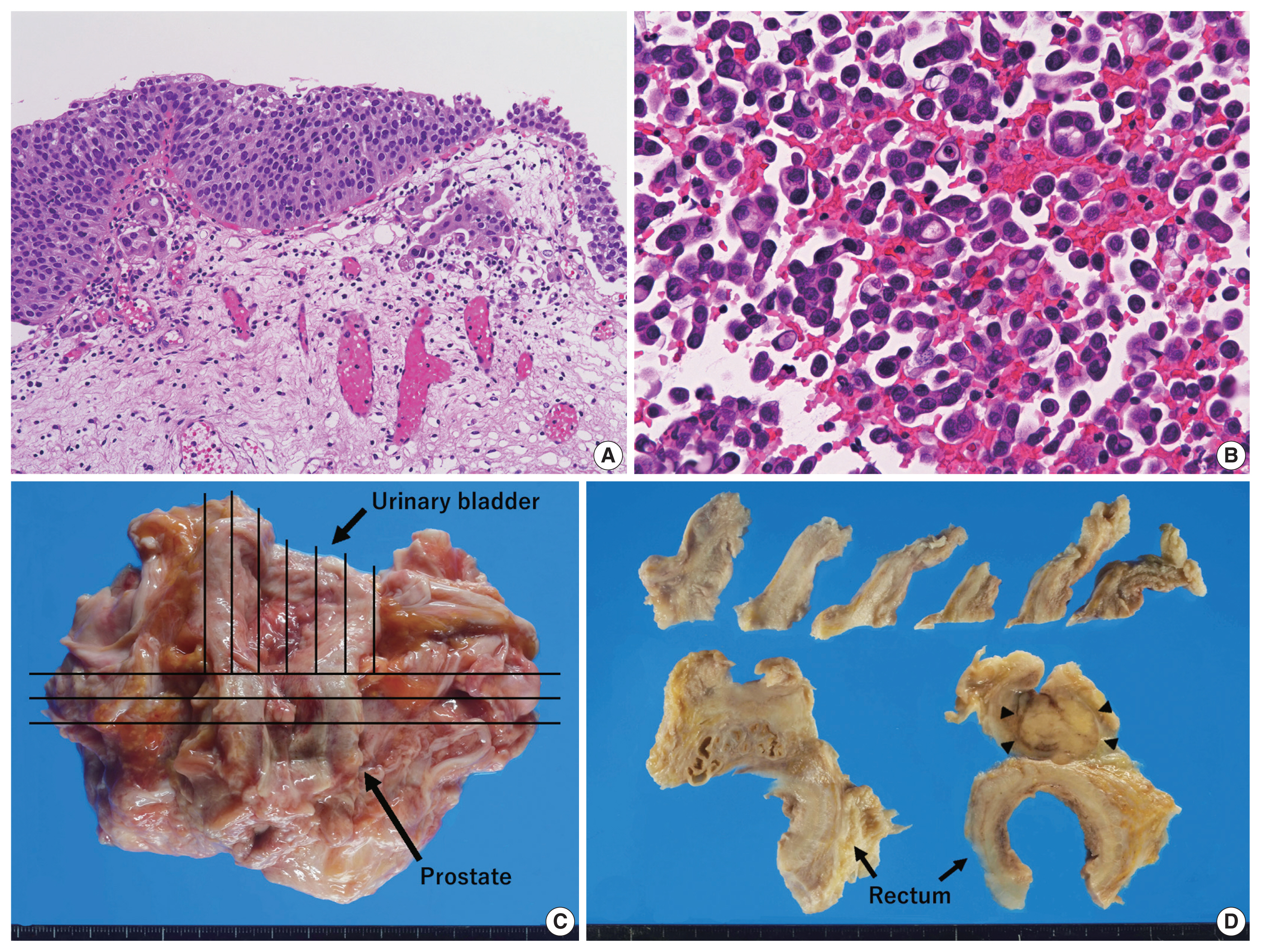
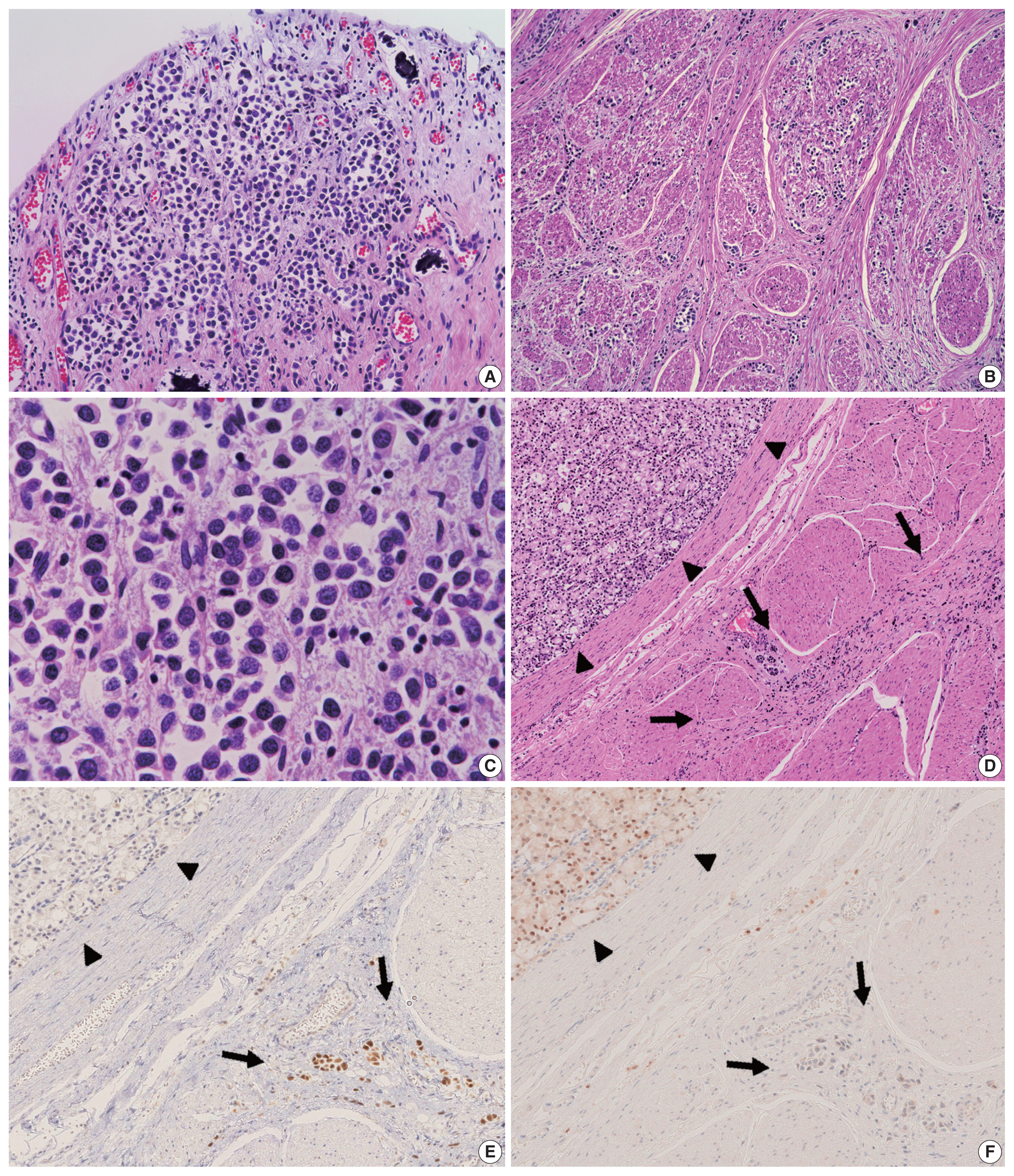



Fig. 1
Fig. 2
Fig. 3
| Protein | Clone | Manufacturer, catalog number | Host | Antigen retrieval | Dilution |
|---|---|---|---|---|---|
| β-catenin | Monoclonal, β-catenin-1 | Dako, Glostrup, Denmark, M3539 | Mouse | Boil, 95°C 30 min, EDTA pH = 9 | 1:200 |
| CK7 | Monoclonal, OV-TL 12/30 | Dako, M7018 | Mouse | Proteinase K, 37°C 15 min | 1:200 |
| CK20 | Monoclonal, Ks20.8 | Dako, M7019 | Mouse | Proteinase K, 37°C 15 min | 1:100 |
| D2-40 | Monoclonal, D2-40 | Dako, M3619 | Mouse | None | 1:50 |
| E-cadherin | Monoclonal, 4A2c7 | Invitrogen, Carlsbad, CA, USA, 18-0223 | Mouse | Boil, 95°C 30 min, EDTA pH = 9 | 1:100 |
| GATA3 | Monoclonal, L50-823 | Biocare Medical, Concord, CA, USA, 1-800-799-9499 | Mouse | Boil, 95°C 30 min, EDTA pH = 9 | 1:300 |
| HER2 | Polyclonal | Dako, K5204 (HercepTest II) | Rabbit | Boil, 95°C 40 min, specialized buffer | Ready-to-use |
| Nkx3.1 | Monoclonal, EP356 | Nichirei, Tokyo, Japan, 418281 | Rabbit | Autoclave, 121°C 10 min, EDTA pH = 9 | Ready-to-use |
| p63 | Monoclonal, 7JUL | Leica Biosystems, Newcastle Upon Tyne, UK, NCL-p63 | Mouse | Boil, 95°C 30 min, EDTA pH = 9 | 1:50 |
| PSA | Monoclonal, ER-PR8 | Dako, M0750 | Mouse | None | 1:100 |
| TTF-1 | Monoclonal, SPT24 | Novocastra, Newcastle Upon Tyne, UK, NCL-TTF-1 | Mouse | Boil, 95°C 30 min, EDTA pH = 9 | 1:200 |
| Case No. | Author | Age (yr)/Sex | Primary tumor size/Location | Operative procedure | Chemoradiotherapy | % PUC/Total UC | Immunohistochemical analysis | Direct invasion | Distant metastasis | Prognosis | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
| ||||||||||||||
| CK7 | CK20 | E-cad | GATA3 | HER2 | ||||||||||
| 1 | Simon et al. [ |
65/M | 7 cm per gross/bladder | TURBT and cysto-prostatectomy | MVAC (3 cycles), Atezolizumab | 100 | + | + | − | + | N/A | Rectal wall | Lungs, pleura, diaphragm, small/large intestine, gallbladder, thoracic and abdominal lymph nodes | DOD 9 mo |
| 2 | Kohada et al. [ |
75/F | N/A/bladder | TURBT | GC (2 cycles), Pembrolizumab | N/A | − | − | + | + | + | Uterus, retroperitoneum | None | DOD 4 mo |
| 3 | Ando et al. [ |
83/M | N/A/bladder | Nephro-ureterectomy | None | N/A | N/A | N/A | − | N/A | N/A | Rectal wall, prostate gland | Peritoneal dissemination and retroperitoneal lymphatic permeation | DOD 2 mo |
| 4 | Tanaka et al. [ |
85/M | 8 × 6 cm |
TURBT | None | N/A | + | + | − | N/A | N/A | Prostate gland | Liver, spleen, kidneys, adrenal glands, bone marrow | DOC (AMI) 37 days |
| 5 | Present case | 89/M | 10 × 7 cm |
TURBT | None | 100 | + | + | + | + | − | Rectal wall, seminal vesicle, paraprostatic tissue | Lungs, right kidney and ureter, left testis, pancreas, liver hilum, right adrenal gland, small/large intestine, pleural/peritoneal dissemination, retroperitoneal tissue, bone marrow, thoracic and abdominal lymph nodes | DOD 1 year and 5 mo |
EDTA, ethylenediaminetetraacetic acid; CK, cytokeratin; GATA3, GATA binding protein 3; HER2, human epidermal growth factor receptor 2; Nkx3.1, NK3 homeobox 1; PSA, prostate-specific antigen; TTF-1, thyroid transcription factor-1.
PUC, plasmacytoid urothelial carcinoma; UC, urothelial carcinoma; CK, cytokeratin; E-cad, E-cadherin; HER2, human epidermal growth factor receptor 2; M, male; TURBT, transurethral resection of bladder tumor; MVAC, methotrexate, vinblastine, doxorubicin and cisplatin; N/A, not available; DOD, death of disease; F, female; GC, gemcitabine and cisplatin; DOC, death of other cause; AMI, acute myocardial infarction. Period after TURBT; Period after para-duodenum tissue biopsy, by which carcinoma of unknown origin was firstly detected; At the time of autopsy.

