E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 60(4); 2026 > Article
-
Case study
SDH-deficient renal cell carcinoma with intracytoplasmic mucinous material: a case report and literature review -
Ryosuke Yoshioka1
 , Kosuke Miyai1,2, Kimi Kato3, Keiichi Ito4, Kimiya Sato1,5, Susumu Matsukuma1,2
, Kosuke Miyai1,2, Kimi Kato3, Keiichi Ito4, Kimiya Sato1,5, Susumu Matsukuma1,2 -
Journal of Pathology and Translational Medicine 2026;60(4):456-461.
DOI: https://doi.org/10.4132/jptm.2026.04.23
Published online: July 15, 2026
1Department of Laboratory Medicine, National Defense Medical College Hospital, National Defense Medical College, Saitama, Japan
2Department of Pathology and Laboratory Medicine, National Defense Medical College, Saitama, Japan
3Department of Pathology, Japan Self-Defense Forces Central Hospital, Tokyo, Japan
4Department of Urology, National Defense Medical College, Saitama, Japan
5Department of Basic Pathology, National Defense Medical College, Saitama, Japan
- Corresponding Author Kosuke Miyai, MD, PhD Department of Laboratory Medicine, National Defense Medical College Hospital, 3-2 Namiki, Tokorozawa, Saitama 359-8513, Japan Tel: +81-4-2995-1211, Fax: +81-4-2996-5193, E-mail: mykusu228@nifty.com
© The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 64 Views
- 3 Download
Abstract
- Succinate dehydrogenase (SDH)–deficient renal cell carcinoma (RCC) is a rare, molecularly defined neoplasm. We report a 45-year-old man with a right renal mass treated by nephrectomy. Grossly, a 38-mm gray-white-to-brown solid cystic tumor was observed in the lower pole of the kidney. Microscopically, the tumor consisted of sheets and nested proliferation of eosinophilic cells with low-grade nuclei and bubbly or flocculent cytoplasm. No sarcomatoid or rhabdoid features were observed. Abundant extracellular and focal intracytoplasmic mucinous material was observed in the tumor, which was positive for Alcian blue and mucicarmine staining, but negative for periodic acid–Schiff staining. Immunohistochemistry showed complete loss of succinate dehydrogenase subunit B in tumor cells. These findings supported the diagnosis of RCC consistent with SDH-deficient RCC. This case expands the morphological spectrum of SDH-deficient RCC and highlights the diagnostic pitfalls of renal tumors with mucinous material.
- Succinate dehydrogenase (SDH)–deficient renal cell carcinoma (RCC) is a molecularly defined RCC, comprising less than 0.2% of all RCCs and typically affecting younger individuals, with a median age of approximately 35 years at diagnosis. The SDH complex, composed of four subunits (SDHA, SDHB, SDHC, and SDHD), is a mitochondrial enzyme integral to both the Krebs cycle and electron transport chain. Germline mutations in any of these subunits can lead to destabilization of the SDH complex, resulting in the loss of SDHB protein expression—a diagnostic hallmark of SDH-deficient tumors [1].
- SDH-deficient RCC is histologically characterized by nests or sheets of uniform eosinophilic cells with indistinct borders, low-grade nuclei, and cytoplasmic vacuoles or inclusions containing pale eosinophilic or flocculent material [1]. Although most tumors exhibit indolent morphology, recent studies have highlighted a broader histological spectrum, including high-grade transformation, sarcomatoid or rhabdoid features, and overlapping morphology with fumarate hydratase (FH)–deficient RCC and transcription factor EB (TFEB)–rearranged RCC [2-5].
- To date, mucinous material has not been recognized as a common morphological feature of SDH-deficient RCC, and reports describing this phenomenon remain limited [2,6]. Herein, we report a case of RCC consistent with SDH-deficient RCC showing focal intracytoplasmic mucinous material. This case expands the recognized morphological heterogeneity of this rare tumor subtype. Awareness of this atypical presentation is essential to avoid misclassification—particularly in the differential diagnosis of mucin-producing renal neoplasms and metastatic carcinomas—and to prompt appropriate ancillary testing, including SDHB immunohistochemistry and genetic evaluation.
INTRODUCTION
- A 45-year-old Japanese man with no notable medical history, including a history of malignancy or hereditary syndromes, was incidentally diagnosed with a right renal mass during a routine health screening. The patient's mother had died of colon cancer, and the histopathological subtype was unknown. Abdominal imaging revealed a 40-mm mass in the lower pole of the right kidney. Contrast-enhanced X-ray computed tomography showed early enhancement with washout, and magnetic resonance imaging revealed a partially cystic lesion with high signal intensity on T2- and diffusion-weighted imaging. Preoperatively, no clear evidence of extrarenal invasion or metastasis was observed. A laparoscopic right nephrectomy was performed for the clinical diagnosis of RCC.
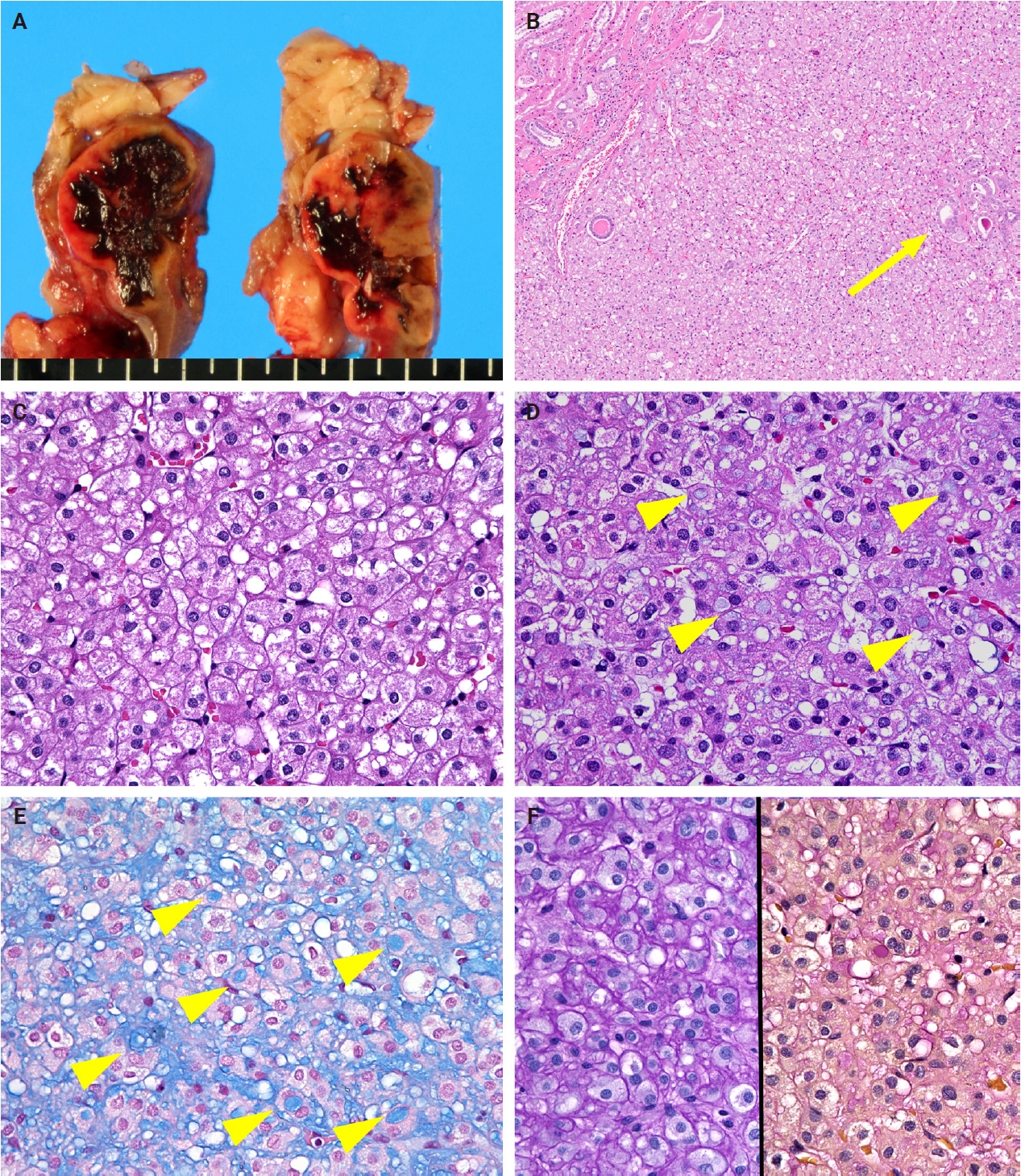
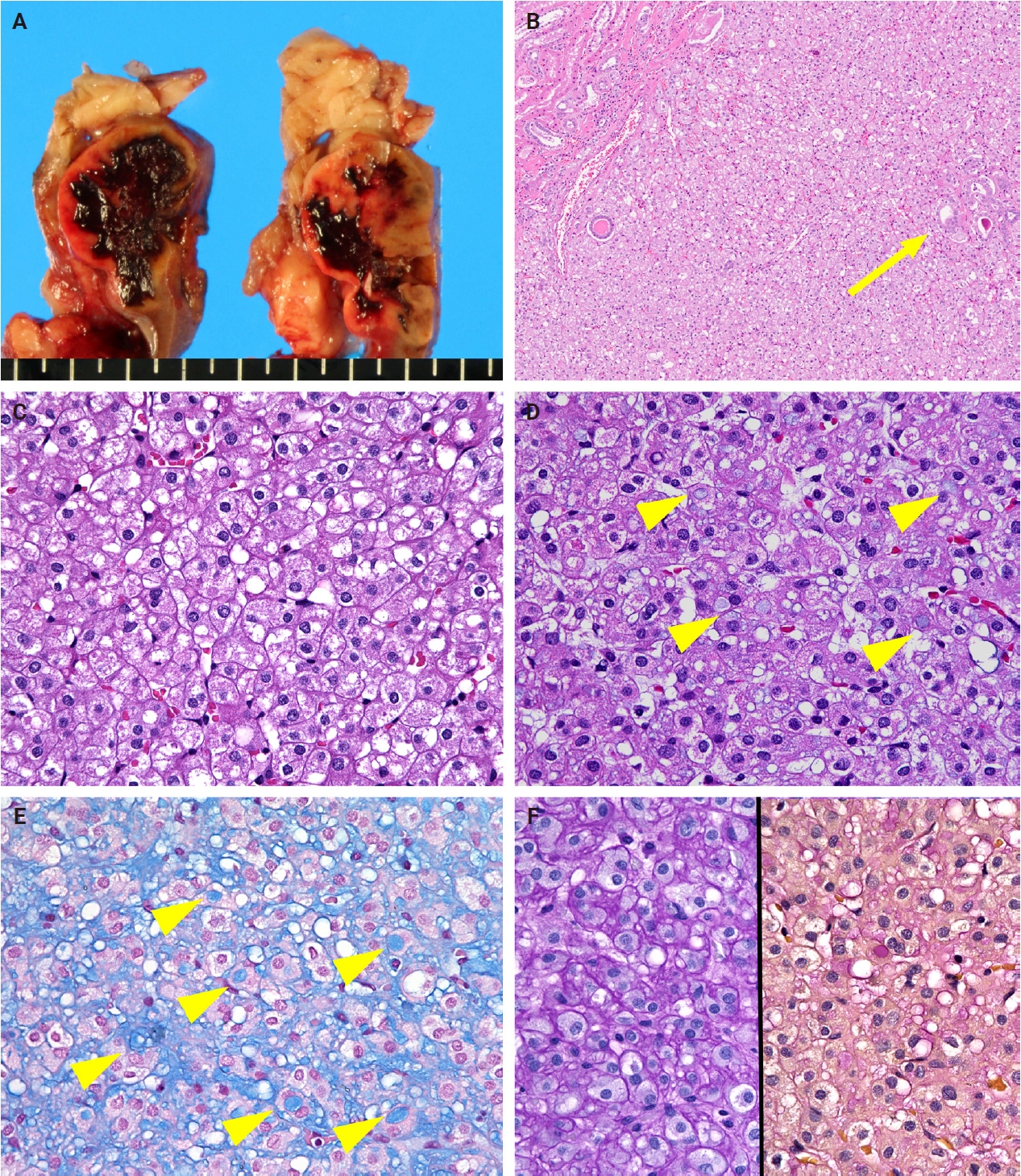
- The resected specimen showed a well-circumscribed, gray-white-to-dark-brown, solid, hemorrhagic, and cystic tumor measuring 38 × 30 × 25 mm in the renal parenchyma (Fig. 1A). Microscopically, the tumor displayed predominantly sheet-like and nested growth patterns with focal cystic areas. At the tumor periphery, no distinct fibrous capsule was observed, and entrapped non-neoplastic renal tubules were noted (Fig. 1B). The tumor cells had bland, round-to-oval nuclei, corresponding to World Health Organization/International Society of Urological Pathology nuclear grade 1, and an eosinophilic cytoplasm with frequent bubbly or pale flocculent features (Fig. 1C). The cell borders were indistinct. Although cystic degeneration and hemorrhage were present, no evidence of coagulative tumor necrosis was observed. No high-grade features, such as sarcomatoid or rhabdoid changes, nuclear pleomorphism, or increased mitotic activity, were identified. Notably, the mucinous material was distributed in a patchy pattern throughout the tumor, predominantly in the intercellular stroma; however, focal and distinct intracytoplasmic accumulation was also observed (Fig. 1D). The intracytoplasmic mucinous material was positive for Alcian blue (pH 2.5) (Fig. 1E) and mucicarmine staining, but negative for periodic acid–Schiff (PAS) staining (Fig. 1F). The mucinous material distributed in the intercellular stroma was also positive for Alcian blue, but negative for mucicarmine staining.
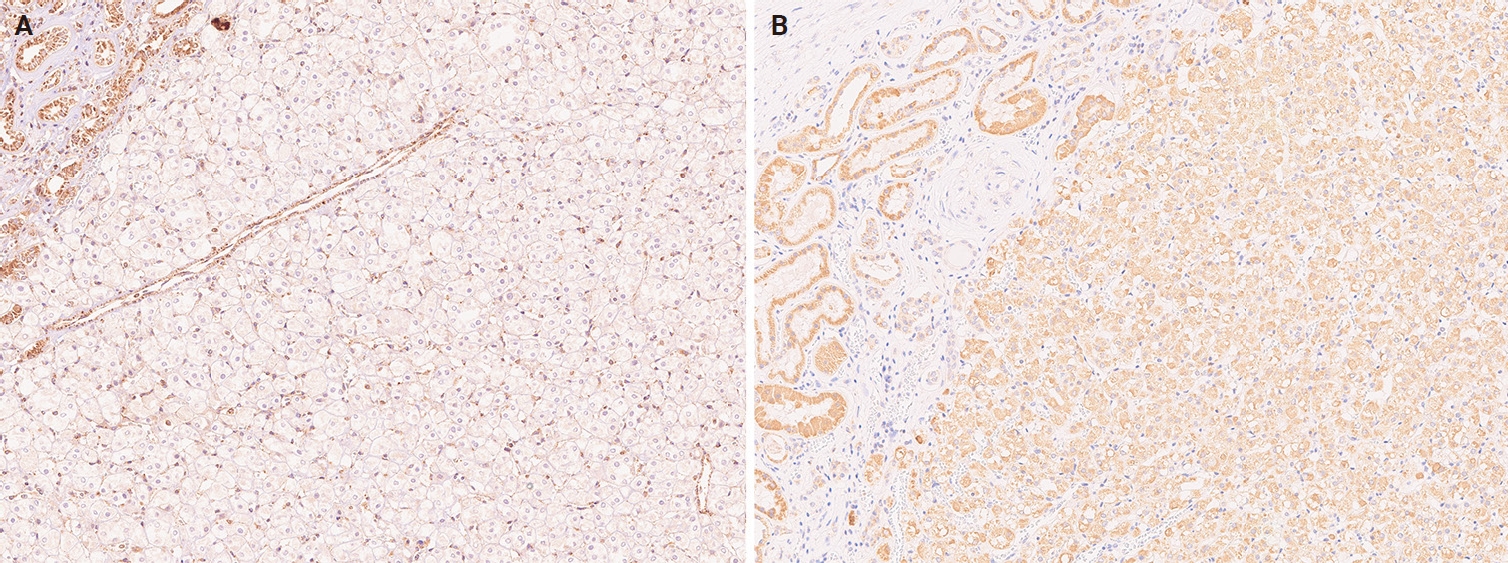
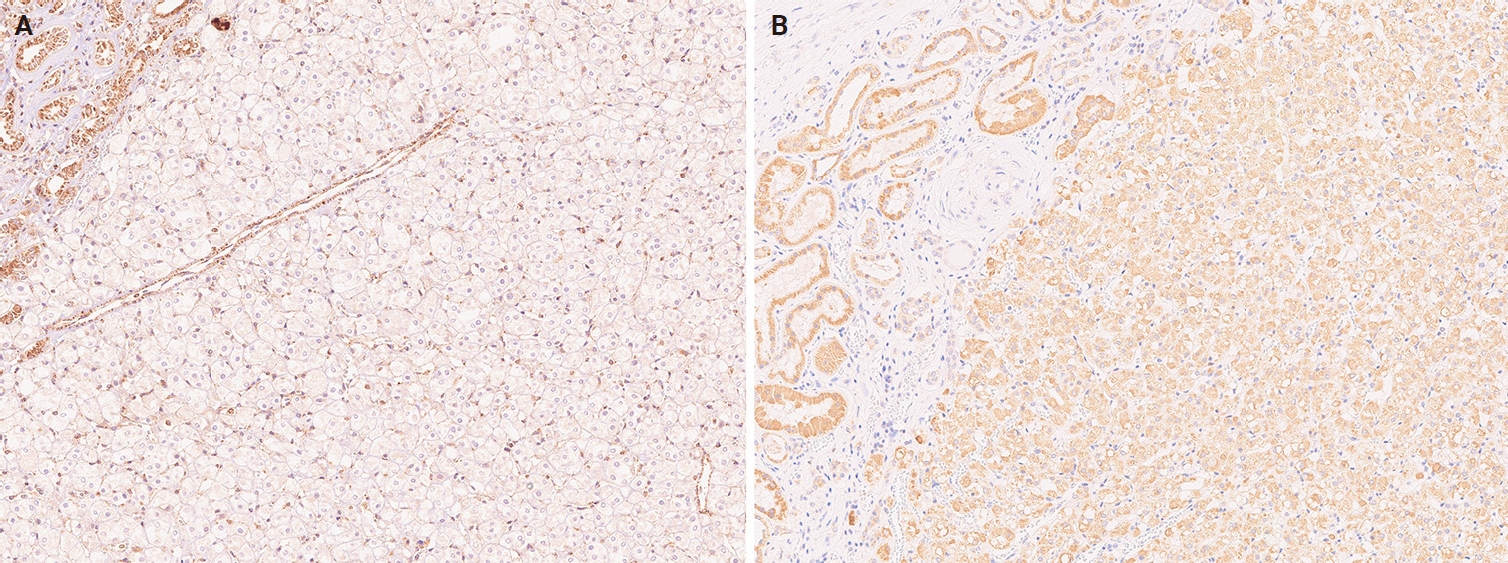
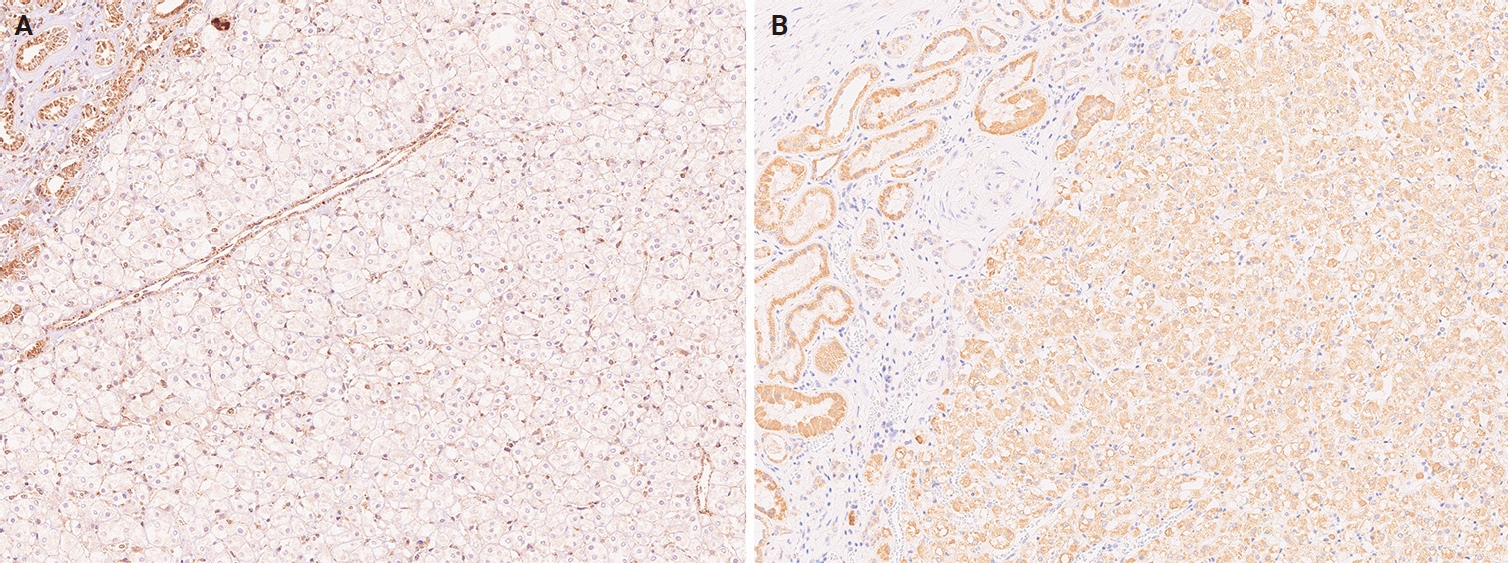
- Immunohistochemically, the tumor cells were positive for PAX8 and focally positive for cytokeratin (CK) AE1/AE3, alpha-methylacyl-CoA racemase, CD117, and vimentin, and negative for CK7, CD10, RCC markers, human melanoma black 45, and anaplastic lymphoma kinase (ALK). Transcription factor E3 (TFE3) showed cytoplasmic staining only without nuclear expression, and TFEB showed only weak staining without evidence of overexpression. SDHB immunostaining showed a complete loss of cytoplasmic expression in the tumor cells, with strong granular positivity in the adjacent non-neoplastic renal tubules, serving as an internal positive control (Fig. 2A). SDHA expression was retained in the tumor cells (Fig. 2B). Genetic testing for pathogenic germline variants in the SDH genes (SDHA, SDHB, SDHC, and SDHD) was not performed because the patient did not provide consent.
- Based on the morphologic and immunohistochemical findings, the tumor was considered consistent with SDH-deficient RCC with focal intracytoplasmic mucinous material. The tumor was confined to the kidney, with no invasion into the renal sinus or perinephric fat. Lymphovascular invasion of tumor cells was not identified, and the surgical margins were negative. The pathologic T category was pT1a. The patient remains alive and well, with no evidence of recurrence or metastasis at 49 months postoperatively.
CASE REPORT
- RCC encompasses diverse subtypes, defined by distinct morphologies, immunophenotypes, and molecular alterations. SDH-deficient RCC is a rare subtype that typically arises in younger individuals and is characterized by loss of SDHB protein expression [1]. In the present case, the unilateral renal mass displayed morphologic features compatible with SDH-deficient RCC, including an eosinophilic cytoplasm with a bubbly or flocculent appearance, low-grade nuclei, and a heterogeneous architecture composed of sheet-like and microcystic patterns. Notably, Alcian blue-positive mucinous material was found extracellularly and focally within the cytoplasm, which is an uncommon feature of SDH-deficient RCC.
- Recently, the morphological spectrum of SDH-deficient RCC has expanded. In addition to the classical bland histology, some tumors exhibit overlapping features with FH-deficient RCC or TFEB-rearranged RCC or display high-grade transformations such as sarcomatoid or rhabdoid differentiation. These variant morphologies may correlate with more aggressive clinical behavior [2-5]. Only two cases of mucinous material deposition in SDH-deficient RCC have been reported to date. Ajmal et al. described the presence of extracellular mucinous material in a high-grade tumor with sarcomatoid and rhabdoid features. That study noted only a small amount of extracellular mucinous material, and no histological images were provided. Additionally, no information was provided about the distribution pattern of mucinous material deposition or the results of the histochemical staining used to determine its nature [2]. Hu et al. [6] reported intracellular and intraluminal mucinous material deposition in SDHA-deficient RCC. That study described single tumor cells containing intracellular mucinous material and small- to medium-sized, round, dilated, and twisted glandular ducts around the tumor nodule. Histologic images showed gray-blue mucinous material filling the lumina of the tumor glands. However, no information was provided regarding the results of histochemical staining [6]. In contrast, our case demonstrated Alcian blue-positive, PAS-negative mucinous material predominantly located in the intercellular spaces, with focal intracytoplasmic deposition, indicating the presence of acidic mucopolysaccharides. Furthermore, mucicarmine staining was weakly and focally positive, which supports this interpretation. To the best of our knowledge, this case represents one of the few reported cases in which the mucinous material was characterized histochemically. This finding expands the known morphological spectrum of this tumor type and underscores the importance of recognizing the deposition of mucinous material in SDH-deficient RCC. Further accumulation of cases with detailed histochemical evaluation is required to clarify the nature and distribution of mucinous material.
- The differential diagnosis in the present case includes other renal neoplasms with eosinophilic cytoplasm and mucinous material. Among renal tumors, mucinous tubular and spindle cell carcinoma (MTSC) is an important consideration because it characteristically shows mucinous stroma. However, the present tumor lacked the spindle cell component and well-formed tubular structures that are characteristic of MTSC, and was also negative for CK7 and CD10, which is inconsistent with MTSC. ALK-rearranged RCC may also show extracellular and intracellular mucinous material, sometimes with signet-ring-like change [7]. However, the present tumor was negative for ALK and lacked other characteristic features, such as inflammatory cell infiltration and papillary or cribriform architecture. TFE3/TFEB-rearranged RCC was also considered, given its known morphologic variability and occasional overlapping eosinophilic features. However, the present tumor showed no obvious histologic findings including biphasic clear/eosinophilic cell population and basement membrane-like material, or convincing TFE3/TFEB overexpression; therefore, a TFE3/TFEB-associated translocation renal cell carcinoma was not supported. In addition, PAX8 positivity supported renal epithelial origin, arguing against non-renal SDH-deficient neoplasms such as paraganglioma. Taken together, the morphologic and immunohistochemical findings supported a diagnosis of RCC consistent with SDH-deficient RCC.
- Loss of SDHB expression is a diagnostic hallmark of SDH-deficient tumors, irrespective of the subunit affected. Dysfunction of any SDH subunit (SDHA, SDHB, SDHC, or SDHD) disrupts the complex, causing the SDHB protein to become unstable and undetectable. Therefore, SDHB immunohistochemistry serves as a reliable diagnostic marker of SDH deficiency [8]. In the present case, the combination of complete loss of SDHB expression and retained SDHA expression was diagnostically important and strongly supported SDH-deficient RCC. At the same time, this immunophenotype does not identify the specific underlying SDH gene alteration. Among SDH-deficient RCCs, SDHB-deficient RCC is predominant, whereas SDHA-, SDHC-, and SDHD-deficient RCCs are less common. Despite limited data, tumors with SDHA alterations tend to show unusual morphologies, including high-grade nuclear atypia, papillary, cribriform, sarcomatoid, and rhabdoid morphologies [1,6]. Interestingly, the only previously documented case of intracytoplasmic mucinous material accumulation in SDH-deficient RCC was also associated with SDHA deficiency [6]. In contrast, the retained SDHA expression in the present case argues against SDHA-deficient RCC with loss of SDHA protein expression. However, because molecular genetic testing was not performed, the precise SDH subunit alteration could not be determined. Further accumulation of genetically characterized cases will be necessary to clarify whether specific SDH subunit alterations are associated with distinct morphologic features or clinical behavior.
- Germline alterations in SDH subunit genes underlie SDH-deficient tumor syndrome, which encompasses pheochromocytoma/paraganglioma, SDH-deficient gastrointestinal stromal tumors, and pituitary neuroendocrine neoplasms. Although immunohistochemical SDHB loss in tumor cells is an effective marker of SDH deficiency, it cannot differentiate between mutated SDH subunits (except that concurrent loss of SDHB and SDHA suggests SDHA deficiency) [8]. A major limitation of the present case is the absence of molecular genetic testing. Although the morphologic findings and immunophenotype, particularly SDHB loss with retained SDHA expression, strongly support SDH-deficient RCC, the specific underlying genetic alteration could not be identified. However, genetic testing is generally recommended because identifying the specific SDH subunit allows for the customization of surveillance [9]. Each subunit is associated with a different set of tumors and different penetrance, and the result enables targeted cascade testing in relatives. Importantly, genotyping also distinguishes SDHB-, SDHC-, and SDHD-mutated tumors that are indistinguishable by immunohistochemistry, thereby facilitating clinicopathological correlations, including comparisons of morphological variation and clinical course across subtypes. Even when genetic testing is not performed, long-term surveillance for other SDH-deficient neoplasms should be considered [9].
- In summary, we report one of the few documented cases of RCC consistent with SDH-deficient RCC showing histochemically characterized extracellular and focal intracytoplasmic mucinous material. This case further expands the morphological spectrum of SDH-deficient RCC. SDH-deficient RCC should be considered in the differential diagnosis of renal tumors with mucinous material, although such cases are likely rare. Further case accumulation with genetic analysis of the SDH subunit genes is warranted to clarify the correlation between specific SDH subunit mutations and distinct histological features.
DISCUSSION
Ethics Statement
This single case report was exempted from Institutional Review Board review and subsequent informed consent by the National Defense Medical College, Tokorozawa, Japan (Registration number, 5156; decision date, March 10, 2025).
Availability of Data and Material
Data sharing not applicable to this article as no datasets were generated or analyzed during the study.
Code Availability
Not applicable.
Author Contributions
Conceptualization: RY, KK, KM. Data curation: RY, KK, KM. Formal analysis: KM. Investigation: RY, KK, KM. Methodology: KM. Project administration: KM. Resources: KI. Supervision: KM, KI, KS, SM. Validation: KS, SM. Visualization: RY, KM. Writing—original draft: RY, KM. Writing—review & editing: KK, KS, SM. Approval of final manuscript: all authors.
Conflicts of Interest
The authors declare that they have no potential conflicts of interest.
Funding Statement
No funding to declare.
Acknowledgments
We thank Ms. Ruu Hokari (National Defense Medical College) for her excellent technical assistance.
- 1. WHO Classification of Tumours Editorial Board. WHO classification of tumours: urinary and male genital tumours. 5th ed. Lyon: International Agency for Research on Cancer, 2022; 31-130.
- 2. Ajmal N, Lallas CD, McCue P, Li L. Succinate dehydrogenase deficient renal cell carcinoma with sarcomatoid and rhabdoid features: a diagnostic dilemma. Int J Surg Pathol 2024; 32: 1508-13. ArticlePubMedPDF
- 3. Santa F, Dabaghian A, Posfai B, et al. Morphological diversity in SDH-deficient renal carcinomas: a three-case exploration of variant features and dedifferentiation. Virchows Arch 2024; 485: 1167-73. ArticlePubMedPDF
- 4. Fuchs TL, Maclean F, Turchini J, et al. Expanding the clinicopathological spectrum of succinate dehydrogenase-deficient renal cell carcinoma with a focus on variant morphologies: a study of 62 new tumors in 59 patients. Mod Pathol 2022; 35: 836-49. ArticlePubMedPDF
- 5. Gill AJ, Hes O, Papathomas T, et al. Succinate dehydrogenase (SDH)-deficient renal carcinoma: a morphologically distinct entity: a clinicopathologic series of 36 tumors from 27 patients. Am J Surg Pathol 2014; 38: 1588-602. ArticlePubMedPMC
- 6. Hu M, Wang XT, Xiao XX, Rao Q, Fan LF, Yue JQ. Renal cell carcinoma with succinate dehydrogenase A mutation: a case report and literature review. Oncol Lett 2024; 29: 84.ArticlePubMedPMC
- 7. Kuroda N, Trpkov K, Gao Y, et al. ALK-rearranged renal cell carcinoma (ALK-RCC): a multi-institutional study of twelve cases with identification of novel partner genes CLIP1, KIF5B and KIAA1217. Mod Pathol 2020; 33: 2564-79. ArticlePubMedPDF
- 8. Gill AJ, Matias-Guiu X, Mete O, et al. SDH-deficient tumour syndrome: hereditary phaeochromocytoma-paraganglioma syndromes (SDHA, SDHB, SDHC, SDHD, SDHAF2). In: Rubin MA, editor. WHO classification of tumours: urinary and male genital tumours. 5th ed [Internet]. Lyon: International Agency for Research on Cancer, 2022 [cited 2025 Nov 28]. Available from: https://tumourclassification.iarc.who.int/chaptercontent/67/196.
- 9. Gill AJ. Succinate dehydrogenase (SDH)-deficient neoplasia. Histopathology 2018; 72: 106-16. ArticlePubMedPDF
REFERENCES
Figure & Data
References
Citations
-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-
- Related articles
-
- Cytological characteristics of Müllerian adenosarcoma of the uterine corpus: a case report and literature review
- Composite chronic lymphocytic leukemia and mantle cell lymphoma involving the bone marrow: a case report and literature review
- Concurrent intestinal plasmablastic lymphoma and diffuse large B-cell lymphoma with a clonal relationship: a case report and literature review
- Intravascular NK/T-cell lymphoma: a case report and literature review
- Metastatic choroidal melanoma in the breast: a case report and review of the literature