 E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 57(6); 2023 > Article
-
Case Study
Intravascular NK/T-cell lymphoma: a case report and literature review -
Ji Min Na1
 , Wookjae Jung2, Minhye Kim2, Yun-Hong Cheon3, Jong Sil Lee4, Dae Hyun Song4, Jung Wook Yang4
, Wookjae Jung2, Minhye Kim2, Yun-Hong Cheon3, Jong Sil Lee4, Dae Hyun Song4, Jung Wook Yang4 -
Journal of Pathology and Translational Medicine 2023;57(6):332-336.
DOI: https://doi.org/10.4132/jptm.2023.10.30
Published online: November 14, 2023
1Department of Pathology, Samsung Medical Center, Seoul, Korea
2Department of Pathology, Gyeongsang National University Hospital, Jinju, Korea
3Division of Rheumatology, Department of Internal Medicine, Gyeongsang National University Hospital, Jinju, Korea
4Department of Pathology, Gyeonsang National University Hospital, Gyeongsang National University College of Medicine, Jinju, Korea
- Corresponding Author: Jung Wook Yang, MD, PhD, Department of Pathology, Gyeongsang National University Hospital, Gyeongsang National University College of Medicine, 15 Jinju-dearo 816beon-gil, Jinju 52727, Korea Tel: +82-55-772-8065, Fax: +82-55-759-7952, E-mail: woogi1982@gnu.ac.kr
© 2023 The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
- Intravascular lymphoma is characterized by an exclusively intravascular distribution of tumor cells. Intravascular natural killer/T-cell lymphoma (IVNKTL) is extremely rare, highly aggressive, commonly Epstein-Barr virus (EBV)–positive, and predominantly affects the skin and central nervous system. Here we report a case of IVNKTL diagnosed in a 67-year-old female, presenting with persistent intermittent fever and skin rashes throughout the body. Incisional biopsy of an erythematous lesion on the chest exhibited aggregation of medium to large-sized atypical lymphoid cells confined to the lumen of small vessels that were positive for CD3, granzyme B, and CD56 on immunohistochemistry and EBV-encoded RNA in situ hybridization. EBV DNA was also detected in serum after diagnosis. With a review of 26 cases of IVNKTL to date, we suggest that active biopsy based on EBV DNA detection may facilitate early diagnosis of IVNKTL.
- A 67-year-old woman with a history of asthma (adequately treated) was admitted with an intermittent night fever (39°C) lasting 1 month and general weakness that persisted after antibiotic treatment at a local hospital. Other vital signs were stable and there were no symptoms or signs other than fever, erythematous skin rash on the chest, and general weakness. Laboratory tests revealed slightly low white blood cell count, 3,090/mm3 (4000–10,000/mm3), and increased aspartate transaminase level of 99 U/L (0–37 U/L), alanine transaminase level of 42 U/L (0– 41 U/L), and lactate dehydrogenase level of 2,600 U/L (135– 225 U/L). Peripheral blood smear findings were normal. Immunological tests for antinuclear antibodies and rheumatoid factors were negative. Blood, cerebrospinal fluid (CSF), and urine cul-tures also yielded negative results. Chest computed tomography (CT) revealed a focal consolidative lesion in the right lower lobe and bronchial wall thickening in both lungs. Slightly enlarged lymph nodes were found in the mediastinum and both hilar regions. Positron emission tomography showed multiple focal hot uptake lesions in bones, suggesting the differential diagnosis of multiple myeloma. However, a bone marrow biopsy and protein electrophoresis revealed no evidence of multiple myeloma or other malignancies. Abdominal and brain CT showed no remarkable findings. There was no history or evidence of hemophagocytic syndrome. The origin of the fever remained unclear. Given the recurrent fever, skin rash, and lymphadenopathy, adult-onset Still disease was suspected, and high-dose prednisolone was prescribed. After treatment, the fever subsided, but the skin rash showed little improvement. The patient developed a fever again, accompanied by multiple erythematous skin lesions all over her body. Her mental status decreased, and she underwent episodes of seizure. Brain CT and magnetic resonance imaging scans showed no specific findings. An incisional skin biopsy of the anterior chest was performed.
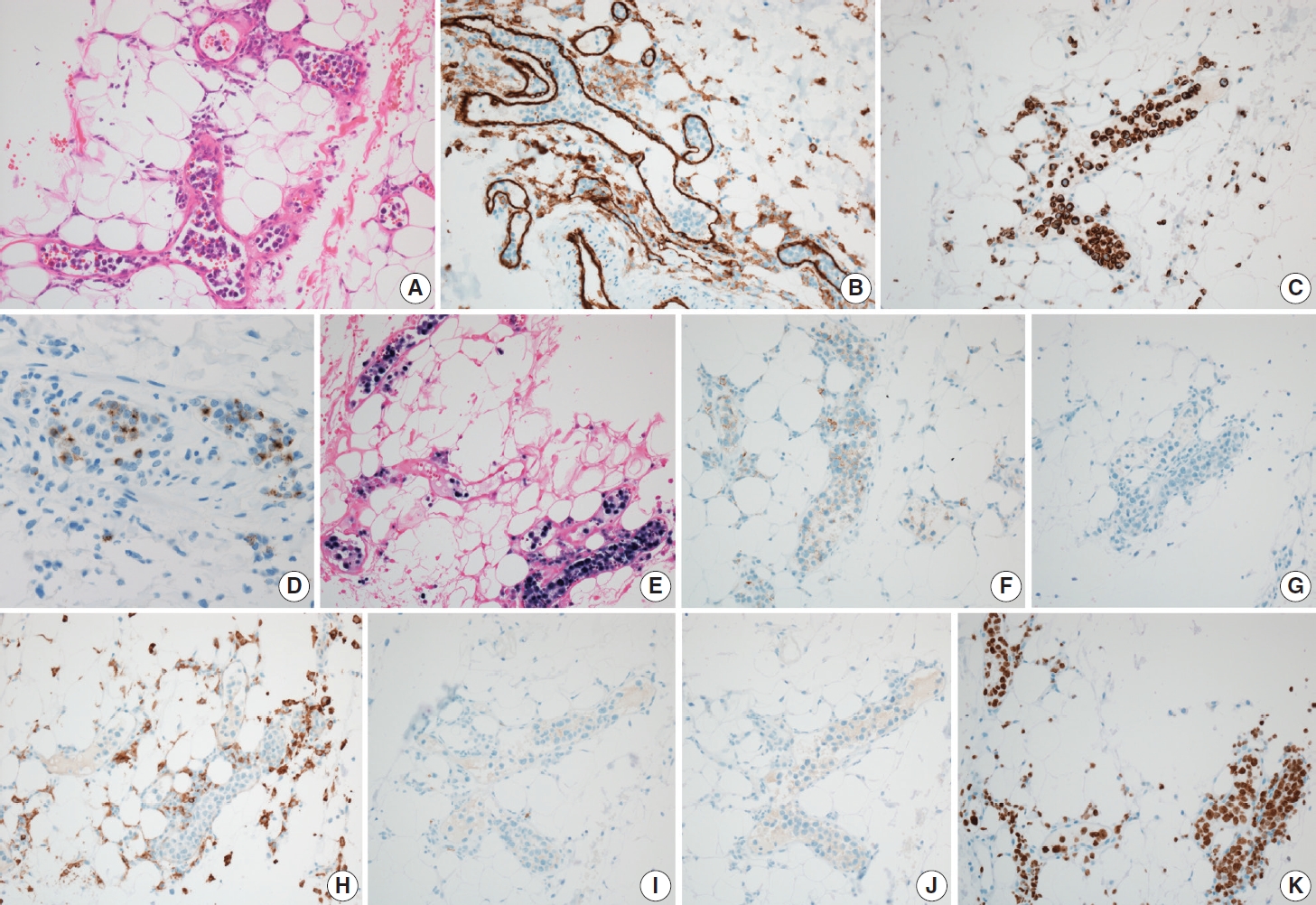
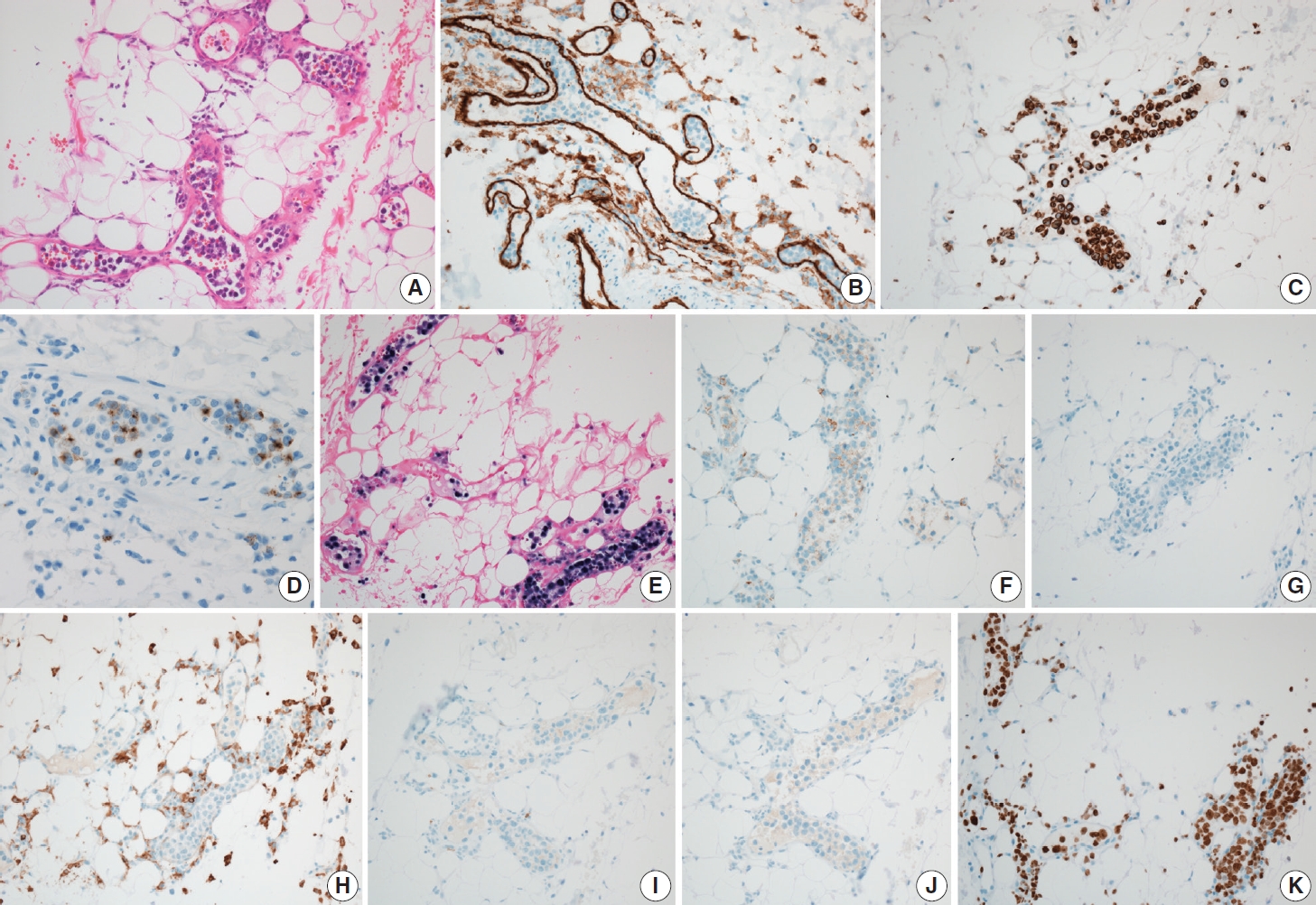
- Microscopic examination of skin specimen revealed mildly dilated capillaries in the dermis and superficial subcutaneous fat. Atypical lymphoid cells were confined to the lumen of the small blood vessels. The intravascular atypical cells were medium to large in size compared to normal lymphocytes and were poorly cohesive. The atypical cells had large, irregular nuclei and scanty cytoplasm (Fig. 1A). Occasional mitoses were observed. Immunohistochemistry (IHC) for CD31 highlighted the vasculature, and the intravascular presence of atypical cells was confirmed (Fig. 1B). Atypical cells were positive for CD3 (Fig. 1C), granzyme B (Fig. 1D), and EBV-encoded RNA (EBER) in situ hybridization (Fig. 1E). CD56 was weakly positive in the atypical cells (Fig. 1F). CD20, CD4, CD8, and CD30 expression were negative (Fig. 1G–J), and the Ki-67 proliferation index was >90% (Fig. 1K). A T-cell receptor (TCR) gene rearrangement test did not show monoclonal T-cell proliferation. In conclusion, the patient was diagnosed with cutaneous intravascular EBV-positive NK/T-cell lymphoma. After diagnosis, polymerase chain reaction (PCR) detected EBV DNA (445,000 copies/mL) in serum. The patient’s clinical condition deteriorated with acute respiratory failure, and her mental status did not improve. She and her family opted for hospice care and no further pathological examination was done, but the progression of symptoms suggested that multiorgan failure and brain involvement had occurred. The patient expired 18 days after diagnosis.
CASE REPORT
- IVNKTL is an extremely rare, highly aggressive lymphoma that predominantly involves the skin and central nervous system. Histological diagnosis is essential. Twenty-seven cases of IVNKTL, including the present case, with sufficient immunohistochemical and clonality data, have been reported (Table 1). The patients included 13 men and 14 women aged 18–87 years. The clinical presentation varied, including skin rash, neurologic symptoms, fever, cytopenia, weight loss, and malaise. Most patients had skin lesions (23/27, 85.2%, skin lesion only in 11 patients). Central nervous system involvement was found in 10 patients (10/27, 37.0%). Most of tested cases showed EBER positivity (22/26, 84.6%). Seven cases with clonality data showed the presence of monoclonal proliferation (7/22, 31.8%).
- A skin biopsy is the easiest and most effective way to diagnose IVNKTL; however, it is challenging in patients without obvious skin lesions. Of the four patients without skin lesions, two presented with neurological symptoms and were diagnosed by brain biopsy (cases No. 23 and 26), and the other two were confirmed on autopsy (cases No. 3 and 25). Brain biopsy is more burdensome than skin biopsy. In each case, brain biopsy was performed after neurological symptoms worsened, and EBV DNA was detected in the CSF. The other two patients showed various symptoms and signs, including pancytopenia at presentation, and were diagnosed by bone marrow biopsy and autopsy. Autopsies of the last two patients revealed multiorgan involvement of IVNKTL, including the brain, kidneys, and bone marrow.
- Bone marrow involvement was uncommon (4/19, 21.1%) and seemed to be associated with poor prognosis. In the case reported by Gebauer et al. [13] (case no. 14), bone marrow biopsy revealed dense medullary infiltration of IVNKTL, constituting approximately 40% of the overall cellularity. However, bone marrow biopsies showed only subtle sinusoidal lymphomatous infiltration in the other two cases (cases Nos. 3 and 25). The remaining case exhibited no evidence of neoplastic infiltration in morphological and IHC analyses of the bone marrow biopsy, and only TCR gene rearrangement test of the bone marrow aspirate confirmed clonality (case No. 23). Although bone marrow involvement may be uncommon, it can also easily be missed. Meanwhile, patients with bone marrow involvement showed shorter survival (<1 month) after confirmation of bone marrow involvement. Bone marrow involvement may indicate rapid disease progression; however, further evaluation is needed.
- Most reports did not mention EBV DNA PCR testing (24/27, 88.9%). In three recent cases, EBV DNA PCR of pleural effusion, lung tissue (case No. 25), CSF (case No. 26), and blood (present case) was positive. Serum EBV DNA load has been suggested as a biomarker in EBV-associated cancers such as nasopharyngeal carcinoma, Burkitt lymphoma, and EBV-positive Hodgkin lymphoma [24]. IVNKTL may also present with a high serum EBV DNA load. Since procedures for histopathological examination (e.g., brain biopsy) are invasive, detection of serum EBV DNA could provide a supportive basis for conducting further work-up for diagnosis, especially in patients without apparent skin lesions.
- In conclusion, we reported a case of IVNKTL in which serum EBV DNA was detected. An active skin biopsy or other invasive biopsy based on EBV DNA detection may facilitate early diagnosis of IVNKTL.
DISCUSSION
Ethics Statement
This study was approved by the Institutional Review Board of Gyeongsang National University Hospital, and the need for informed consent was waived (IRB No. GNUH 2023-07-033).
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
Code Availability
Not applicable.
Author contributions
Conceptualization: JWY. Data Curation: JMN, WJ, JWY. Investigation: JMN, WJ, JWY. Resources: MK, YHC, JSL. Supervision: YHC, JWY. Visualization: JMN, JWY. Writing—original draft preparation: JMN, JWY. Writing—review & editing: JMN, DHS, JWY. Approval of final manuscript: all authors.
Conflicts of Interest
The authors declare that they have no potential conflicts of interest.
Funding Statement
No funding to declare.
Acknowledgments
| Case | Age (yr)/Sex | Biopsy sites | Skin lesion | CNS inv. | Cytopenia | Bone marrow inv. | EBV DNA | EBER | TCR | Survival |
|---|---|---|---|---|---|---|---|---|---|---|
| Santucci et al. (2003) [4] | 54/M | Skin | + | #NAME? | Leuko- | NA | NA | + | NA | Died 17 mo after dx. |
| Wu et al. (2005) [5] | 41/M | Skin | + | – | – | – | NA | + | Germline | Alive 12 mo after dx. |
| Wu et al. (2005) [5] | 47/F | Skin | + | + | Pan- | + (on IHC) | NA | – | Germline | Died 15 days after dx. |
| Kuo et al. (2006) [6] | 71/F | Skin | + | – | – | – | NA | + | Germline | Alive 5 mo after dx. |
| Song et al. (2007) [7] | 40/F | Skin | + | + | – | – | NA | + | Germline | Alive 7 mo after dx. |
| Nakamichi et al. (2008) [8] | 23/F | Skin | + | – | – | – | NA | + | Germline | Died 9 mo after dx |
| Cerroni et al. (2008) [9] | 67/F | Skin | + | + | – | NA | NA | NA | Clonal (TCRg) | Died 7 days after dx. |
| Cerroni et al. (2008) [9] | 63/M | Skin | + | – | Leuko- | NA | NA | + | Germline | Died 6 mo after dx. |
| Thrombo- | ||||||||||
| Cerroni et al. (2008) [9] | 64/M | Skin | + | NA | – | – | NA | – | Germline | Died 7 mo after dx. |
| Cerroni et al. (2008) [9] | 87/M | Skin | + | – | – | NA | NA | + | Clonal (TCRg) | Died 15 days after dx. |
| Gleason et al. (2008) [10] | 62/M | Skin | + | – | – | – | NA | – | Clonal (TCRg) | Alive 8 mo after dx. |
| Liao (2011) [11] | 42/F | Skin | + | – | – | – | NA | + | NA | Alive 14 mo after dx. |
| Yanning et al. (2013) [12] | 84/F | Skin | + | NA | – | NA | NA | + | Germline | Alive 4 mo after dx. |
| Gbauer et al. (2014) [13] | 72/M | Skin | + | + (6 mo after dx.) | Pan– (6 mo after dx.) | + (40%, 6 mo after dx.) | NA | + | Germline | Died 7 mo after dx. |
| Jang et al. (2014) [14] | 23/F | Skin | + | – | – | – | NA | + | Germline | Died 18 mo after dx. |
| Liu et al. (2014) [15] | 38/F | Skin | + | – (7 mo after dx.) | – | – | NA | + | NA | Died 13 mo after dx. |
| Wang et al. (2015) [16] | 45/M | Skin | + | NA | – | NA | NA | + | Germline | Died 15 days after dx. |
| Wang et al. (2015) [16] | 32/F | Skin | + | – | – | NA | NA | + | Germline | Died 4 mo after dx. |
| Wang et al. (2015) [16] | 18/F | Skin | + | – | – | – | NA | + | Germline | Alive 3 yr after dx. |
| Bi et al. (2015) [17] | 29/M | Skin | + | – | – | – | NA | + | Germline | Died 3 mo after dx. |
| Alhumidi (2015) [18] | 48/F | Skin | + | – | – | – | NA | + | NA | Alive 18 mo after dx. |
| Okonkwo and Jaffe (2017) [19] | 51/M | Skin | + | + | – | NA | NA | + | Clonal (TCRg) | NA |
| Sharma et al. (2017) [20] | 62/F | Brain | – | + | – | + (on TCR) | NA | – | Clonal | Died 7 days after dx. |
| Alegria-Landra et al. (2017) [21] | 81/M | Skin | + | – | – | – | NA | + | Clonal (TCRb & g) | Died 15 days after dx. |
| Zanelli et al. (2018) [22] | 54/M | Autopsy | – | + | Pan- | + (10%) | + (PE & lung) | + | Clonal | Died 18 days after presentation |
| Meisoner et al. (2022) [23] | 53/M | Brain | – | + | – | – | + (CFS) | + | NA | Alive 8 yr after SCT |
| Present case | 67/F | Skin | + | + (sx. only) | Leuko- | – | + (blood) | + | Germline | Died 18 days after dx. |
NK, natural killer; CNS, central nervous system; inv., involvement; EBV, Epstein-Barr virus; EBER, Epstein-Barr virus-encoded small RNA; TCR, T-cell receptor gene rearrangement; M, male; F, female; dx., diagnosis; NA, not available; IHC, immunohistochemistry; PE, pleural effusion; SCT, stem cell transplantation; sx., symptom.
- 1. WHO classification of tumours of haematopoietic and lymphoid tissues. Revised 4th ed. Lyon: International Agency for Research in Cancer, 2017; 317-406.
- 2. Alaggio R, Amador C, Anagnostopoulos I, et al. The 5th edition of the World Health Organization classification of haematolymphoid tumours: lymphoid neoplasms. Leukemia 2022; 36: 1720-48. PubMedPMC
- 3. Zanelli M, Parente P, Sanguedolce F, et al. Intravascular NK/T-cell lymphoma: what we know about this diagnostically challenging, aggressive disease. Cancers (Basel) 2022; 14: 5458.ArticlePubMedPMC
- 4. Santucci M, Pimpinelli N, Massi D, et al. Cytotoxic/natural killer cell cutaneous lymphomas. Report of EORTC Cutaneous Lymphoma Task Force Workshop. Cancer 2003; 97: 610-27. ArticlePubMedPDF
- 5. Wu H, Said JW, Ames ED, et al. First reported cases of intravascular large cell lymphoma of the NK cell type: clinical, histologic, immunophenotypic, and molecular features. Am J Clin Pathol 2005; 123: 603-11. ArticlePubMed
- 6. Kuo TT, Chen MJ, Kuo MC. Cutaneous intravascular NK-cell lymphoma: report of a rare variant associated with Epstein-Barr virus. Am J Surg Pathol 2006; 30: 1197-201. ArticlePubMed
- 7. Song DE, Lee MW, Ryu MH, Kang DW, Kim SJ, Huh J. Intravascular large cell lymphoma of the natural killer cell type. J Clin Oncol 2007; 25: 1279-82. ArticlePubMed
- 8. Nakamichi N, Fukuhara S, Aozasa K, Morii E. NK-cell intravascular lymphomatosis: a mini-review. Eur J Haematol 2008; 81: 1-7. ArticlePubMed
- 9. Cerroni L, Massone C, Kutzner H, Mentzel T, Umbert P, Kerl H. Intravascular large T-cell or NK-cell lymphoma: a rare variant of intravascular large cell lymphoma with frequent cytotoxic phenotype and association with Epstein-Barr virus infection. Am J Surg Pathol 2008; 32: 891-8. PubMed
- 10. Gleason BC, Brinster NK, Granter SR, Pinkus GS, Lindeman NI, Miller DM. Intravascular cytotoxic T-cell lymphoma: a case report and review of the literature. J Am Acad Dermatol 2008; 58: 290-4. ArticlePubMed
- 11. Liao JB, Hsieh PP, Hwang YC, Lin SL, Wu CS. Cutaneous intravascular natural killer-cell lymphoma: a rare case and review of the literature. Acta Derm Venereol 2011; 91: 472-3. ArticlePubMed
- 12. Yanning X, Chen H, Si H, Liu Y, Min Z. Cutaneous intravascular NK-cell lymphoma. Eur J Dermatol 2013; 23: 252-3. ArticlePubMed
- 13. Gebauer N, Nissen EJ, Driesch P, Feller AC, Merz H. Intravascular natural killer cell lymphoma mimicking mycosis fungoides: a case report and review of the literature. Am J Dermatopathol 2014; 36: e100-4. PubMed
- 14. Jang YH, Lee SJ, Choi YH, et al. Intravascular cytotoxic T-cell lymphoma in a young immunocompetent woman. Ann Dermatol 2014; 26: 496-500. ArticlePubMedPMC
- 15. Liu Y, Zhang W, An J, Li H, Liu S. Cutaneous intravascular natural killer-cell lymphoma: a case report and review of the literature. Am J Clin Pathol 2014; 142: 243-7. PubMed
- 16. Wang L, Chen S, Ma H, et al. Intravascular NK/T-cell lymphoma: a report of five cases with cutaneous manifestation from China. J Cutan Pathol 2015; 42: 610-7. ArticlePubMed
- 17. Bi Y, Huo Z, Liang Z, et al. Intravascular NK-cell lymphoma: a case report and review of the literature. Diagn Pathol 2015; 10: 84.ArticlePubMedPMCPDF
- 18. Alhumidi A. Cutaneous intravascular NK/T-cell lymphoma mimic panniculitis clinically, case report and literature brief review. Diagn Pathol 2015; 10: 107.ArticlePubMedPMCPDF
- 19. Okonkwo L, Jaffe ES. Intravascular large cell lymphoma of NK/Tcell type, EBV positive. Blood 2017; 130: 837.ArticlePubMedPMCPDF
- 20. Sharma TL, Yeaney GA, Soltanzadeh P, Li Y, Cotta CV. Intravascular T-cell lymphoma: a rare, poorly characterized entity with cytotoxic phenotype. Neuropathology 2017; 37: 365-70. ArticlePubMedPDF
- 21. Alegria-Landa V, Manzarbeitia F, Salvatierra Calderon MG, Requena L, Rodriguez-Pinilla SM. Cutaneous intravascular natural killer/T cell lymphoma with peculiar immunophenotype. Histopathology 2017; 71: 994-1002. ArticlePubMedPDF
- 22. Zanelli M, Mengoli MC, Del Sordo R, et al. Intravascular NK/T-cell lymphoma, Epstein-Barr virus positive with multiorgan involvement: a clinical dilemma. BMC Cancer 2018; 18: 1115.ArticlePubMedPMCPDF
- 23. Meissner J, Schmitt M, Andrulis M, et al. Cure of intravascular NK/T-cell lymphoma of the central nervous system by allogeneic hematopoietic cell transplantation. Bone Marrow Transplant 2022; 57: 1451-4. ArticlePubMedPMCPDF
- 24. Patel PD, Alghareeb R, Hussain A, Maheshwari MV, Khalid N. The association of Epstein-Barr virus with cancer. Cureus 2022; 14: e26314.ArticlePubMedPMC
REFERENCES
Figure & Data
References
Citations
- Mimicry in the vasculature: a review of diagnostic clues in cutaneous intravascular lymphoid proliferations
MA Faraz, S Tu Zahra, F Ocampo-Gonzalez, SC Shalin, Aadil Ahmed
Diagnostic Histopathology.2026; 32(3): 155. CrossRef - Intravascular Lymphoma Associated with the Female Genital Tract—Diagnostic Considerations, Therapeutic Approaches, and Outcomes
Aleksandar Ristic, Marija Rovcanin, Ana Tomic, Aleksandar Rakic, Nebojsa Zecevic, Svetlana Jankovic
Diseases.2026; 14(3): 109. CrossRef - Adequacy of Single Random Skin Biopsy With Subcutaneous Sampling for the Diagnosis of Intravascular Lymphoma
Phitsinee Purngpiputtrakul, Panitta Sitthinamsuwan, Sanya Sukpanichnant, Penvadee Pattanaprichakul, Manasmon Chairatchaneeboon, Yingyong Chinthammitr, Pochamana Phisalprapa
Journal of Cutaneous Pathology.2026; 53(8): 731. CrossRef - Intravascular Lymphoma: A Unique Pattern Underlying a Protean Disease
Mario Della Mura, Joana Sorino, Filippo Emanuele Angiuli, Gerardo Cazzato, Francesco Gaudio, Giuseppe Ingravallo
Cancers.2025; 17(14): 2355. CrossRef - Cutaneous Intravascular Hematolymphoid Entities: A Review
Emily Hatheway Marshall, Bethany Brumbaugh, Allison Holt, Steven T. Chen, Mai P. Hoang
Diagnostics.2024; 14(7): 679. CrossRef - CD30- and CD56-positive atypical intravascular lymphocytes of the uterine cervix, mimicking intravascular lymphoma: A case report and review of the literature
Daisuke Yamashita, Munemichi Otani, Hayato Maruoka, Takuya Aoki, Shigeo Hara
Journal of Clinical and Experimental Hematopathology.2024; 64(4): 328. CrossRef
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-
- Related articles
-
- SDH-deficient renal cell carcinoma with intracytoplasmic mucinous material: a case report and literature review
- Clinicopathological characteristics of digestive system angioleiomyomas: case report and literature review
- Cytological characteristics of Müllerian adenosarcoma of the uterine corpus: a case report and literature review
- Composite chronic lymphocytic leukemia and mantle cell lymphoma involving the bone marrow: a case report and literature review
- Concurrent intestinal plasmablastic lymphoma and diffuse large B-cell lymphoma with a clonal relationship: a case report and literature review

Fig. 1.
| Case | Age (yr)/Sex | Biopsy sites | Skin lesion | CNS inv. | Cytopenia | Bone marrow inv. | EBV DNA | EBER | TCR | Survival |
|---|---|---|---|---|---|---|---|---|---|---|
| Santucci et al. (2003) [4] | 54/M | Skin | + | #NAME? | Leuko- | NA | NA | + | NA | Died 17 mo after dx. |
| Wu et al. (2005) [5] | 41/M | Skin | + | – | – | – | NA | + | Germline | Alive 12 mo after dx. |
| Wu et al. (2005) [5] | 47/F | Skin | + | + | Pan- | + (on IHC) | NA | – | Germline | Died 15 days after dx. |
| Kuo et al. (2006) [6] | 71/F | Skin | + | – | – | – | NA | + | Germline | Alive 5 mo after dx. |
| Song et al. (2007) [7] | 40/F | Skin | + | + | – | – | NA | + | Germline | Alive 7 mo after dx. |
| Nakamichi et al. (2008) [8] | 23/F | Skin | + | – | – | – | NA | + | Germline | Died 9 mo after dx |
| Cerroni et al. (2008) [9] | 67/F | Skin | + | + | – | NA | NA | NA | Clonal (TCRg) | Died 7 days after dx. |
| Cerroni et al. (2008) [9] | 63/M | Skin | + | – | Leuko- | NA | NA | + | Germline | Died 6 mo after dx. |
| Thrombo- | ||||||||||
| Cerroni et al. (2008) [9] | 64/M | Skin | + | NA | – | – | NA | – | Germline | Died 7 mo after dx. |
| Cerroni et al. (2008) [9] | 87/M | Skin | + | – | – | NA | NA | + | Clonal (TCRg) | Died 15 days after dx. |
| Gleason et al. (2008) [10] | 62/M | Skin | + | – | – | – | NA | – | Clonal (TCRg) | Alive 8 mo after dx. |
| Liao (2011) [11] | 42/F | Skin | + | – | – | – | NA | + | NA | Alive 14 mo after dx. |
| Yanning et al. (2013) [12] | 84/F | Skin | + | NA | – | NA | NA | + | Germline | Alive 4 mo after dx. |
| Gbauer et al. (2014) [13] | 72/M | Skin | + | + (6 mo after dx.) | Pan– (6 mo after dx.) | + (40%, 6 mo after dx.) | NA | + | Germline | Died 7 mo after dx. |
| Jang et al. (2014) [14] | 23/F | Skin | + | – | – | – | NA | + | Germline | Died 18 mo after dx. |
| Liu et al. (2014) [15] | 38/F | Skin | + | – (7 mo after dx.) | – | – | NA | + | NA | Died 13 mo after dx. |
| Wang et al. (2015) [16] | 45/M | Skin | + | NA | – | NA | NA | + | Germline | Died 15 days after dx. |
| Wang et al. (2015) [16] | 32/F | Skin | + | – | – | NA | NA | + | Germline | Died 4 mo after dx. |
| Wang et al. (2015) [16] | 18/F | Skin | + | – | – | – | NA | + | Germline | Alive 3 yr after dx. |
| Bi et al. (2015) [17] | 29/M | Skin | + | – | – | – | NA | + | Germline | Died 3 mo after dx. |
| Alhumidi (2015) [18] | 48/F | Skin | + | – | – | – | NA | + | NA | Alive 18 mo after dx. |
| Okonkwo and Jaffe (2017) [19] | 51/M | Skin | + | + | – | NA | NA | + | Clonal (TCRg) | NA |
| Sharma et al. (2017) [20] | 62/F | Brain | – | + | – | + (on TCR) | NA | – | Clonal | Died 7 days after dx. |
| Alegria-Landra et al. (2017) [21] | 81/M | Skin | + | – | – | – | NA | + | Clonal (TCRb & g) | Died 15 days after dx. |
| Zanelli et al. (2018) [22] | 54/M | Autopsy | – | + | Pan- | + (10%) | + (PE & lung) | + | Clonal | Died 18 days after presentation |
| Meisoner et al. (2022) [23] | 53/M | Brain | – | + | – | – | + (CFS) | + | NA | Alive 8 yr after SCT |
| Present case | 67/F | Skin | + | + (sx. only) | Leuko- | – | + (blood) | + | Germline | Died 18 days after dx. |
NK, natural killer; CNS, central nervous system; inv., involvement; EBV, Epstein-Barr virus; EBER, Epstein-Barr virus-encoded small RNA; TCR, T-cell receptor gene rearrangement; M, male; F, female; dx., diagnosis; NA, not available; IHC, immunohistochemistry; PE, pleural effusion; SCT, stem cell transplantation; sx., symptom.

