 E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 47(2); 2013 > Article
-
Case Study
Extrapelvic Uterus-like Masses Presenting as Colonic Submucosal Tumor: A Case Study and Review of Literature - Ki Yong Na, Gou Young Kim, Kyu Yeoun Won, Hyun-Soo Kim1, Sang Won Kim2, Chi Hoon Lee3, Jae Myung Cha3
-
Korean Journal of Pathology 2013;47(2):177-181.
DOI: https://doi.org/10.4132/KoreanJPathol.2013.47.2.177
Published online: April 24, 2013
Department of Pathology, Kyung Hee University Hospital at Gangdong, Kyung Hee University School of Medicine, Seoul, Korea.
1Aerospace Medical Research Center, Aerospace Medical Center, Republic of Korea Air Force, Cheongwon, Korea.
2Department of Radiology, Kyung Hee University Hospital at Gangdong, Kyung Hee University School of Medicine, Seoul, Korea.
3Department of Internal Medicine, Kyung Hee University Hospital at Gangdong, Kyung Hee University School of Medicine, Seoul, Korea.
- Corresponding Author: Gou Young Kim, M.D. Department of Pathology, Kyung Hee University Hospital at Gangdong, Kyung Hee University School of Medicine, 892 Dongnam-ro, Gangdong-gu, Seoul 134-727, Korea. Tel: +82-2-440-7551, Fax: +82-2-440-7564, pathogen@medimail.co.kr
© 2013 The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.



Figure & Data
References
Citations
- Ultrasonographic Imaging Features of Accessory Cavitated Uterine Malformations and Application to Diagnosis
Ruijie Sun, Xinting Liu, Niya Wei, Xiaokun Li, Ying Zou, Yue Wang
Journal of Clinical Ultrasound.2025; 53(8): 1707. CrossRef - Clinical Diagnosis and Treatment Analysis of Accessory Cavity Uterine Malformation in Adolescents (with a Case Report and Literature Review)
义敏 项
Advances in Clinical Medicine.2025; 15(08): 1098. CrossRef - Accessory cavitated uterine malformation in a perimenopausal woman: Case report and literature review
Yuan Zhang, Hanxue Lv, Congjie Lin, Hua Liu
Journal of International Medical Research.2025;[Epub] CrossRef - Extrauterine adenomyoma: A case report and systematic review of the literature
Matteo Giorgi, Luca Labanca, Gabriele Centini, Lucia Lazzeri, Francesco Giuseppe Martire, Ester Sorrentino, Virginia Mancini, Diego Raimondo, Antonio Raffone, Daniele Neola, Anna Chiara Aru, Nassir Habib, Paolo Casadio, Renato Seracchioli, Errico Zupi
International Journal of Gynecology & Obstetrics.2024; 164(3): 869. CrossRef - Extrapelvic “Uterus Like Mass” Following Laparoscopic Morcellation Hysterectomy - a Consequence of Iatrogenic Implantation?
Neha Bakshi, Shashi Dhawan
International Journal of Surgical Pathology.2023; 31(5): 791. CrossRef - Extrauterine adenomyoma of the lesser omentum: A case report and review of the literature
Yanlin Chen, Liangyong Deng, Jingbo Zhao, Tianwen Luo, Zhong Zuo
Medicine.2022; 101(36): e30240. CrossRef - Pelvic Pain and Adnexal Mass: Be Aware of Accessory and Cavitated Uterine Mass
Pooya Iranpour, Sara Haseli, Pedram Keshavarz, Amirreza Dehghanian, Neda Khalili, Michael S. Firstenberg
Case Reports in Medicine.2021; 2021: 1. CrossRef - Endomyometriosis of the Rectum With Disseminated Peritoneal Leiomyomatosis 8 Years After Laparoscopic Myomectomy: A Case Report
Giorgio La Greca, Cristina Colarossi, Paolo Di Mattia, Cecilia Gozzo, Marco De Zuanni, Eliana Piombino, Lorenzo Memeo
Frontiers in Surgery.2021;[Epub] CrossRef - Imaging Manifestations of Accessory Cavitated Uterine Mass—A Rare Mullerian Anomaly
Tharani Putta, Reetu John, Betty Simon, Kirthi Sathyakumar, Anuradha Chandramohan, Anu Eapen
Indian Journal of Radiology and Imaging.2021; 31(03): 545. CrossRef - A rare case of ovarian adenomyoma mimicking primary invasive ovarian cancer with a contralateral serous borderline ovarian tumor: A case report and review of the literature
Viola Liberale, Alessandra Surace, Lorenzo Daniele, Luca Liban Mariani
Heliyon.2020; 6(7): e04406. CrossRef - Extrauterine adenomyoma located in the inguinal region: a case report of a 44-year-old woman
Winesh Ramphal, Chloé M L Peters, Luthy S M Alcalá, Dennis van Hamont, Paul D Gobardhan
Journal of Surgical Case Reports.2020;[Epub] CrossRef - Accessory and Cavitated Uterine Mass: Is It a Müllerian-Duct Anomaly?
Vani Malhotra, Sonia Dahiya, Smiti Nanda, Meenakshi Chauhan, Vandana Bhuria
Journal of Gynecologic Surgery.2020; 36(6): 350. CrossRef - Uterus-like mass in the right broad ligament
Lei Liu, Hui Yang, Shu-Peng Zhang
Medicine.2019; 98(38): e17246. CrossRef - Extrauterine adenomyoma: a review of the literature
P.G. Paul, Gunjan Gulati, Hemant Shintre, Sumina Mannur, George Paul, Santwan Mehta
European Journal of Obstetrics & Gynecology and Reproductive Biology.2018; 228: 130. CrossRef - Uterus-like mass
Jian He, Jie Xu, Hong-Yan Zhou
Medicine.2016; 95(39): e4961. CrossRef - Endometrioid Adenocarcinoma in an Extrauterine Adenomyoma
Michael A. Ulm, David B. Robins, Edwin M. Thorpe, Mark E. Reed
Obstetrics & Gynecology.2014; 124(2): 445. CrossRef - Endomyometriosis (“Uterus - like mass”) in an XY Male
Raul S. González, Cindy L. Vnencak-Jones, Chanjuan Shi, Oluwole Fadare
International Journal of Surgical Pathology.2014; 22(5): 421. CrossRef
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-
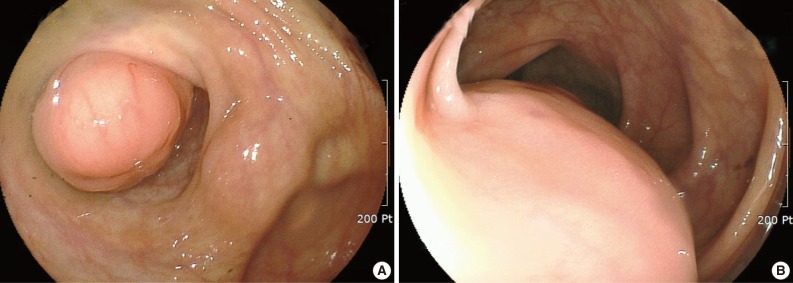

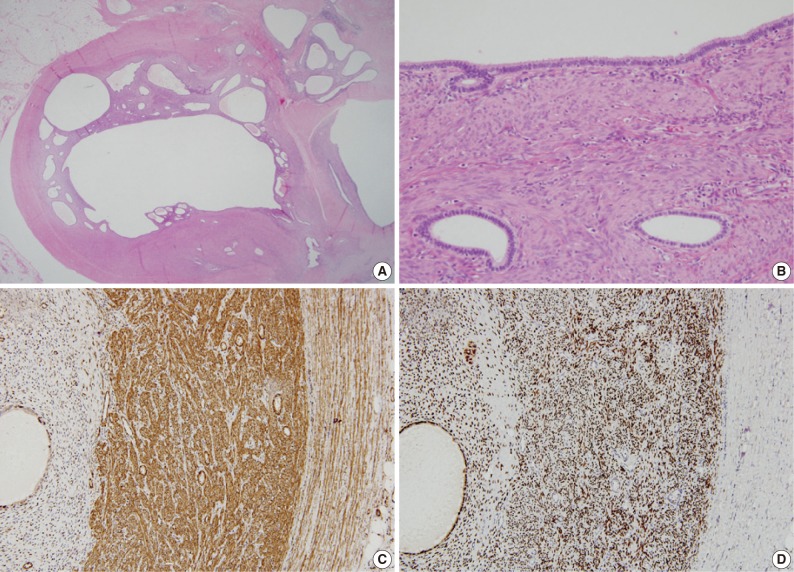



Fig. 1
Fig. 2
Fig. 3
| Authors | Age/sex | Location | Size (cm) | Clinical presentation | Treatment | Associated conditions |
|---|---|---|---|---|---|---|
| Cozzutto [1] | 32/F | Ovary | 6 | LAP | Mass excision | Unilateral renal agenesis, endometriosis |
| Pai et al. [2] | 38/F | Both ovaries |
4 and 3 | Incidental finding | BO | Invasive ductal carcinoma |
| 43/F | Ovary | 11.5 | Pelvic mass | Mass excision | None | |
| 39/F | Ovary | 13 | LAP, vaginal spot | TH + UO | Adenomyosis | |
| Tijani et al. [3] | 35/F | Uterus | 21 | LAP, dysmenorrhea | Mass excision | None |
| Matsuzaki et al. [4] | 29/F | Uterosacral ligament | 7.5 | LAP, dysmenorrhea | Mass excision | None |
| Carinelli et al. [5] | 46/F | Pelvic wall and mesentery |
Up to 10 | LAP, constipation | Partial colectomy | Endometriosis, leiomyomatous nodules |
| 39/F | Ovary and pelvic wall |
Up to 3.5 | LAP, dysmenorrhea | Mass excision | Endometriosis, leiomyomatous nodules | |
| Sharma et al. [6] | 33/F | Conus medullaris | 3 | Lower back mass | Mass excision | Spnia bifida, subcutaneous lipoma, tethered cord |
| 24/F | Conus medullaris | NA | Lower back pain | Mass excision | Tethered cord | |
| Rohlfing et al. [7] | 35/F | Obturator lymph node | 4.5 | Lymph node enlargement | TH + mass excision | Squamous cell carcinoma of cervix |
| Seki et al. [8] | 44/F | Inguinal soft tissue | 3.8 | LAP | Mass excision | Endometriosis |
| Redman et al. [9] | 50/F | Vagina | 8 | LAP, dysuria | Mass excision | Ureteral stricture |
| Peterson et al. [10] | 12/F | Ileum | 2.5 | Incidental finding | Segmental resection | Lower intestinal and urinary tract anomaly |
| Horie and Kato [11] | 59/F | Ileal mesentery | 14 | Abdominal mass | Mass excision | None |
| Shin et al. [12] | 31/F | Sigmoid mesocolon | 3 | LAP | Partial colectomy | None |
| Rougier et al. [13] | 18/F | Conus medullaris | 2.5 | Paresthesia | Mass excision | Spina bifida |
| Jung et al. [14] | 43/F | Uterus | 3 | Menorrhagia, dysmenorrhea | TH | Adenomyosis |
| 52/F | Uterus | 8 | Vulvar itching | TH+USO | Endometriosis | |
| Pai et al. [15] | 25/F | Broad ligament | 20 | Abdominal mass | Mass excision | None |
| Present case | 39/F | Cecum, colon, and mesocolon |
5 | LAP, anemia | Partial colectomy | Endometriosis |
F, female; LAP, low abdominal pain; TH, total hysterectomy; UO, unilateral oophorectomy; BSO, bilateral salpingo-oophorectomy; BO, bilateral oophorectomy; USO, unilateral salpingo-oophorectomy; NA, not available. Multiple uterus-like masses.

