 E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 54(1); 2020 > Article
-
Original Article
Clinicopathologic characteristics of HER2-positive pure mucinous carcinoma of the breast -
Yunjeong Jang1
 , Hera Jung1, Han-Na Kim1, Youjeong Seo1, Emad Alsharif2, Seok Jin Nam3, Seok Won Kim3, Jeong Eon Lee3, Yeon Hee Park4, Eun Yoon Cho1, Soo Youn Cho1
, Hera Jung1, Han-Na Kim1, Youjeong Seo1, Emad Alsharif2, Seok Jin Nam3, Seok Won Kim3, Jeong Eon Lee3, Yeon Hee Park4, Eun Yoon Cho1, Soo Youn Cho1 -
Journal of Pathology and Translational Medicine 2020;54(1):95-102.
DOI: https://doi.org/10.4132/jptm.2019.10.24
Published online: November 13, 2019
1Department of Pathology and Translational Genomics, Samsung Medical Center, Sungkyunkwan University College of Medicine, Seoul, Korea
2Division of Breast and Endocrine Surgery, Specialized Surgical Unit, King Abdullah Medical City, Makkah, Saudi Arabia
3Division of Breast Surgery, Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
4Division of Hematology-Oncology, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
-
Corresponding Author: Soo Youn Cho, MD, PhD, Department of Pathology and Translational Genomics, Samsung Medical Center, Sungkyunkwan University School of Medicine, 81 Irwon-ro, Gangnam-gu, Seoul 06351, Korea Tel: +82-2-3410-2817, Fax: +82-2-3410-0025, E-mail: sooyoun.cho@samsung.com
Corresponding Author: Eun Yoon Cho, MD, PhD, Department of Pathology and Translational Genomics, Samsung Medical Center, Sungkyunkwan University School of Medicine, 81 Irwon-ro, Gangnam-gu, Seoul 06351, Korea Tel: +82-2-3410-2796, Fax: +82-2-3410-0025, E-mail: eunyoon.cho@samsung.com
© 2020 The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
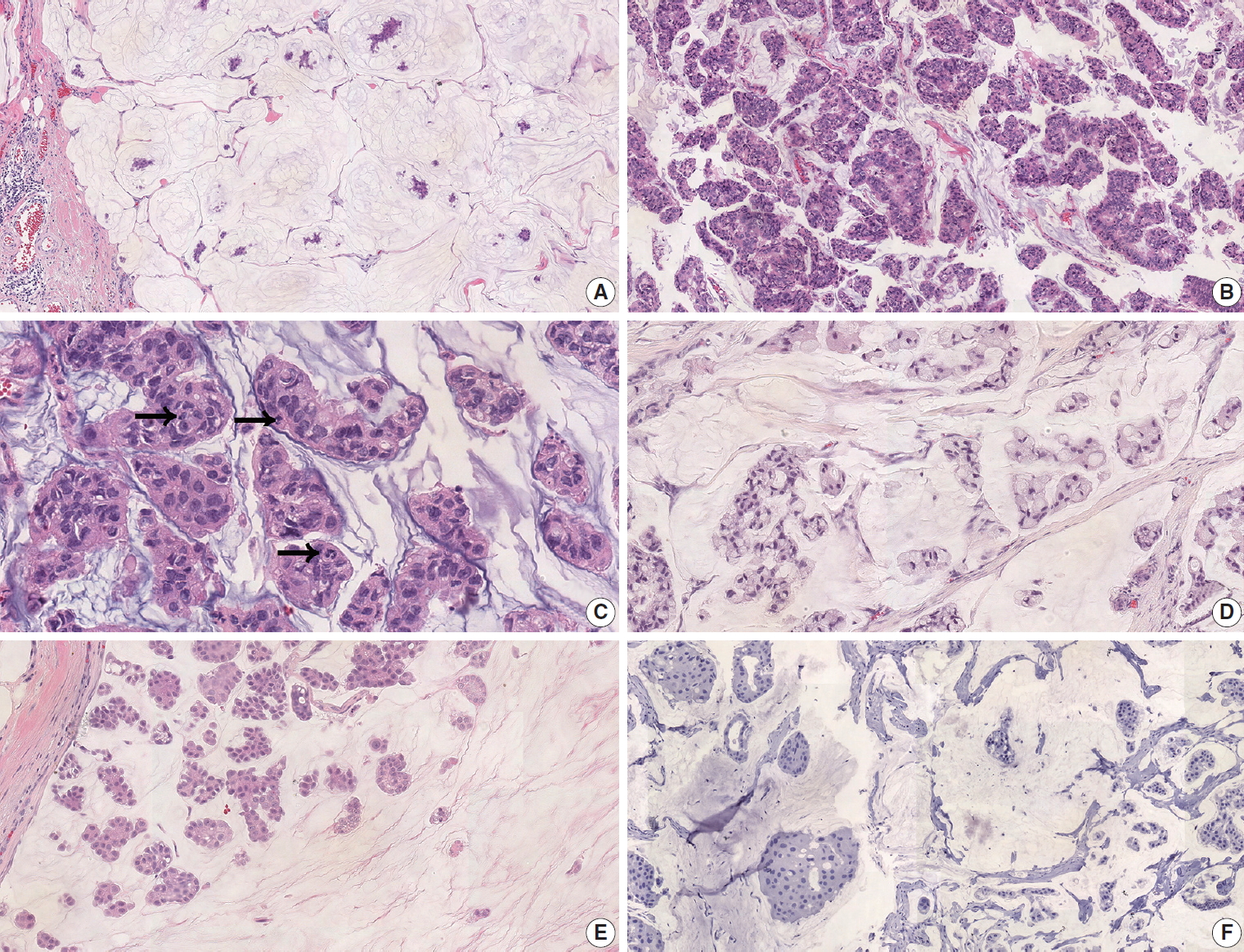
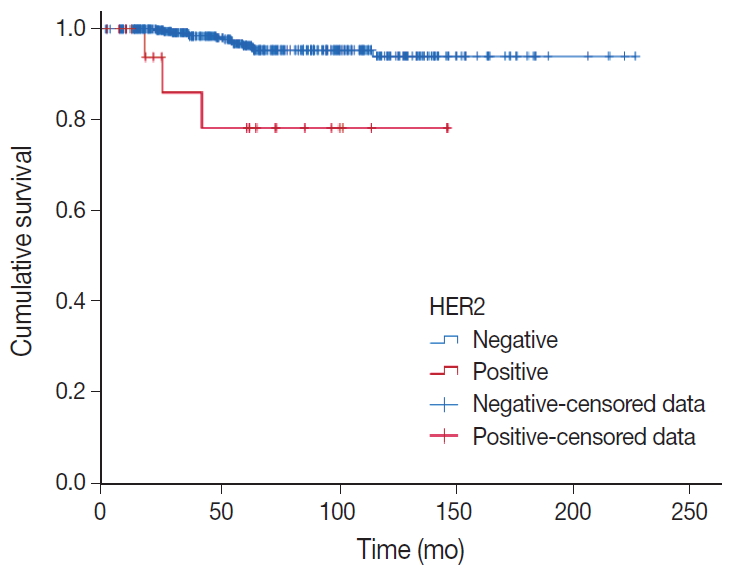
Figure & Data
References
Citations
- Mucin‐producing breast lesions: a practical approach to diagnosis
Sunayana Misra, Mihir Gudi, Kimberly H Allison, Edi Brogi, Cecily Quinn, Hannah Y Wen, Puay Hoon Tan
Histopathology.2026; 88(5): 939. CrossRef - Signet-ring cell cytomorphology in breast cancer: Unveiling the overlooked
Shitong Su, Zijian Liu, Bifeng Yao, Qiuyang Jing, Ruijie Liu, Kuansong Wang
Critical Reviews in Oncology/Hematology.2026; 220: 105170. CrossRef - Predictive factors and prognostic significance of HER2-low early breast cancer with long-term follow-up
Yuka Niwa, Mitsuo Terada, Yumi Wanifuchi-Endo, Takashi Fujita, Tomoko Asano, Hidetoshi Kawaguchi, Kazuki Nozawa, Nana Matsumoto, Ayaka Isogai, Hikaru Kawahara, Marie Mizumoto, Tatsuya Toyama
Surgical Oncology.2026; 64: 102360. CrossRef - Mucinous carcinoma of the breast: morphological spectrum, diagnostic pitfalls and classification challenges
Emad A Rakha, Bara Wazwaz, Stephen B Fox
Journal of Clinical Pathology.2026; : jcp-2026-210712. CrossRef - Clinicopathological characteristics of mucinous breast cancer: a retrospective analysis of a 6-years study from national cancer center in Vietnam
Thi Huyen Phung, Thanh Tung Pham, Huu Thang Nguyen, Dinh Thach Nguyen, Thanh Long Nguyen, Thi Hoai Hoang
Breast Cancer Research and Treatment.2025; 209(3): 667. CrossRef - Poor response of HER2-positive mucinous carcinomas of breast to neoadjuvant HER2-targeted therapy: A study of four cases
Min Han, Daniel Schmolze, Javier A. Arias-Stella, Christina H. Wei, Joanne Mortimer, Fang Fan
Annals of Diagnostic Pathology.2025; 74: 152396. CrossRef - Comprehensive Immunohistochemical Analysis of Mesonephric Marker Expression in Low-grade Endometrial Endometrioid Carcinoma
Yurimi Lee, Sangjoon Choi, Hyun-Soo Kim
International Journal of Gynecological Pathology.2024; 43(3): 221. CrossRef - Clinicopathological features and prognosis of mucinous breast carcinoma with a micropapillary structure
Beibei Yang, Menglu Shen, Bo Sun, Jing Zhao, Meng Wang
Thoracic Cancer.2024; 15(36): 2530. CrossRef - Pure Mucinous Carcinoma of the Breast: Radiologic-Pathologic Correlation
Cherie M Kuzmiak, Benjamin C Calhoun
Journal of Breast Imaging.2023;[Epub] CrossRef - Role of circ-FOXO3 and miR-23a in radiosensitivity of breast cancer
Elahe Abdollahi, Hossein Mozdarani, Behrooz Z. Alizadeh
Breast Cancer.2023; 30(5): 714. CrossRef - On Ultrasonographic Features of Mucinous Carcinoma with Micropapillary Pattern
Wei-Sen Yang, Yang Li, Ya Gao
Breast Cancer: Targets and Therapy.2023; Volume 15: 473. CrossRef - Spectrum of Mucin-containing Lesions of the Breast: Multimodality Imaging Review with Pathologic Correlation
Janice N. Thai, Melinda F. Lerwill, Shinn-Huey S. Chou
RadioGraphics.2023;[Epub] CrossRef - Mesonephric-like Adenocarcinoma of the Ovary: Clinicopathological and Molecular Characteristics
Hyun Hee Koh, Eunhyang Park, Hyun-Soo Kim
Diagnostics.2022; 12(2): 326. CrossRef - Alveolar Soft Part Sarcoma of the Uterus: Clinicopathological and Molecular Characteristics
Yurimi Lee, Kiyong Na, Ha Young Woo, Hyun-Soo Kim
Diagnostics.2022; 12(5): 1102. CrossRef - Metastasis of the Mucionous adenocarcinoma of breast to the mandibular gingiva: Rare case report
Ivana Mijatov, Aleksandra Fejsa Levakov, Aleksandar Spasić, Jelena Nikolić, Saša Mijatov
Medicine.2022; 101(38): e30732. CrossRef - Endometrioid Carcinomas of the Ovaries and Endometrium Involving Endocervical Polyps: Comprehensive Clinicopathological Analyses
Jihee Sohn, Yurimi Lee, Hyun-Soo Kim
Diagnostics.2022; 12(10): 2339. CrossRef - Serous Carcinoma of the Endometrium with Mesonephric-Like Differentiation Initially Misdiagnosed as Uterine Mesonephric-Like Adenocarcinoma: A Case Report with Emphasis on the Immunostaining and the Identification of Splice Site TP53 Mutation
Sangjoon Choi, Yoon Yang Jung, Hyun-Soo Kim
Diagnostics.2021; 11(4): 717. CrossRef - HER2 positive mucinous carcinoma of breast with micropapillary features: Report of a case and review of literature
Dinesh Chandra Doval, Rupal Tripathi, Sunil Pasricha, Pankaj Goyal, Chaturbhuj Agrawal, Anurag Mehta
Human Pathology: Case Reports.2021; 25: 200531. CrossRef - Carcinoma mucosecretor de mama HER2-positivo, un caso clínico
A.M. González Aranda, E. Martínez Gómez, A. Santana Costa, F. Arnanz Velasco, M.H. González de Diego, A. Zapico Goñi
Clínica e Investigación en Ginecología y Obstetricia.2021; 48(4): 100685. CrossRef - Clinicopathologic features of unexpectedly HER2 positive breast carcinomas: An institutional experience
Carissa LaBoy, Kalliopi P. Siziopikou, Lauren Rosen, Luis Z. Blanco, Jennifer L. Pincus
Pathology - Research and Practice.2021; 222: 153441. CrossRef - Mesonephric-like Differentiation of Endometrial Endometrioid Carcinoma: Clinicopathological and Molecular Characteristics Distinct from Those of Uterine Mesonephric-like Adenocarcinoma
Sujin Park, Go Eun Bae, Jiyoung Kim, Hyun-Soo Kim
Diagnostics.2021; 11(8): 1450. CrossRef - Mesonephric-like Adenocarcinoma of the Uterine Corpus: Comprehensive Immunohistochemical Analyses Using Markers for Mesonephric, Endometrioid and Serous Tumors
Hyunjin Kim, Kiyong Na, Go Eun Bae, Hyun-Soo Kim
Diagnostics.2021; 11(11): 2042. CrossRef
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-
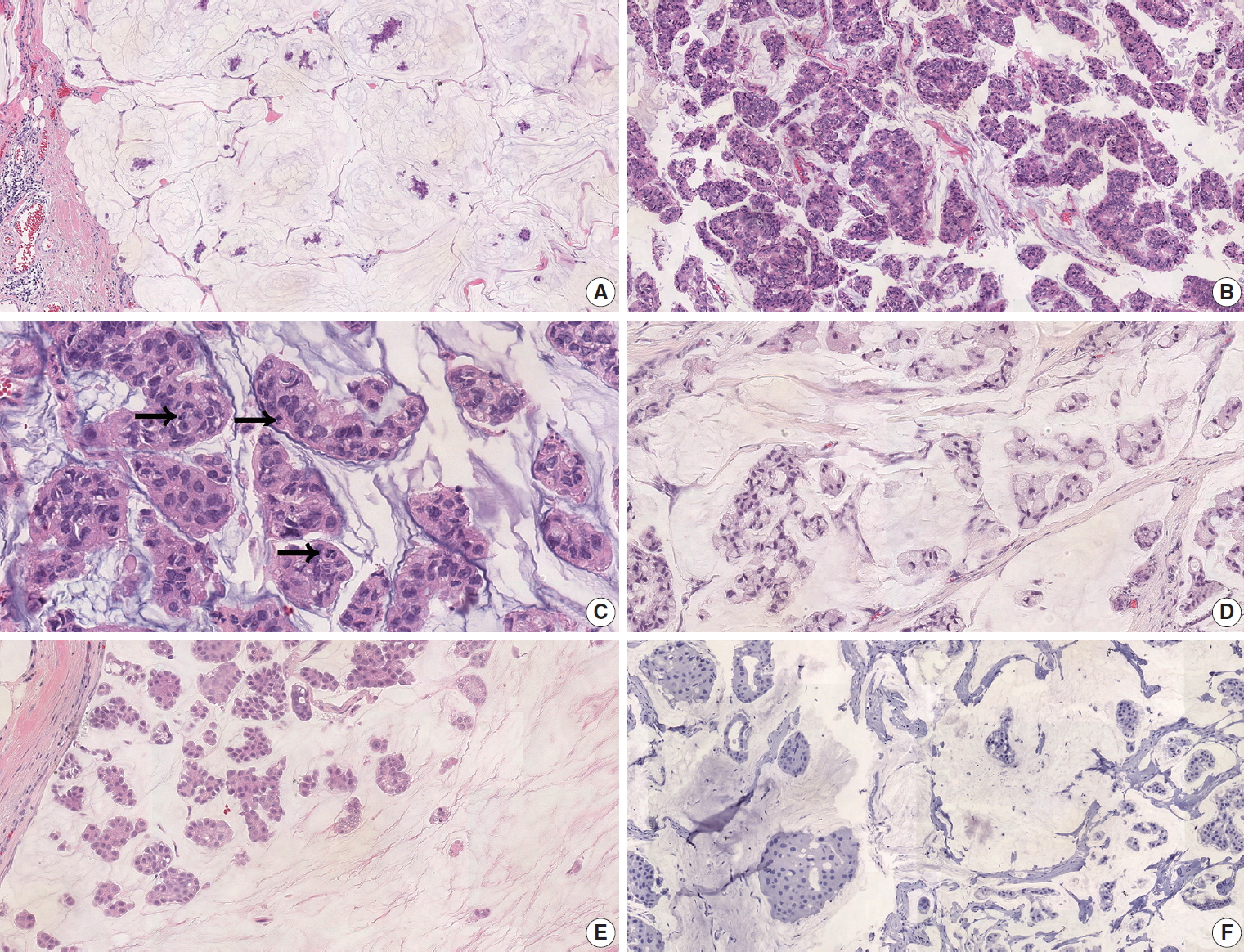
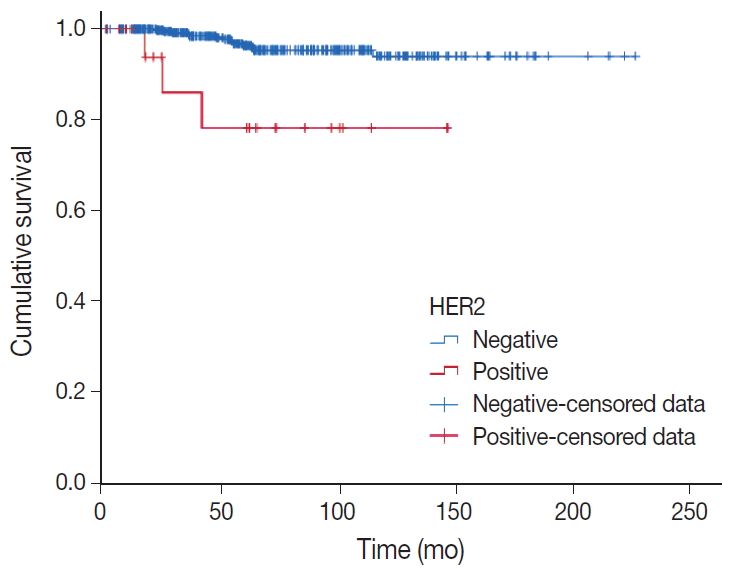


Fig. 1.
Fig. 2.
| Case | Age (yr) | Sex | Procedure | Mass size (mm) | T category | No. of positive LNs | N category | Nuclear | Histologic grade | ER | PR | Type A/B | Structure | Recurrence | Follow-up | Trastuzumab | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 60 | F | T | A | 30.0 | 2 | 0 | 0 | 3 | III | - | - | B | SRC | NED | ND | |
| 2 | 41 | F | B | S | 15.0 | 1 | 0 | 0 | 3 | III | + | + | B | None | NED | ND | |
| 3 | 43 | F | T | S | 3.0 | 1 | 0 | 0 | 2 | II | + | + | A | None | NED | ND | |
| 4 | 28 | F | B | S | 15.0 | 1 | 0 | 0 | 3 | III | + | + | B | SRC | NED | ND | |
| 5 | 60 | F | T | A | 70.0 | 3 | 1 | 1 | 3 | III | - | - | A | MP/SRC | NED | ND | |
| 6 | 43 | F | B | S | 4.0 | 1 | 0 | 0 | 2 | II | - | + | A | None | NED | ND | |
| 7 | 53 | F | T | S | 4.5 | 1 | 0 | 0 | 2 | II | + | - | B | SRC | NED | ND | |
| 8 | 46 | F | T | A | 65/60 |
3 | 5 | 2 | 2 | II | - | - | A | MP/SRC | Local recurrence | DOD | ND |
| 9 | 39 | F | T | A | 38.0 | 2 | 0 | 0 | 2 | II | + | + | NA | None | Metastasis to lung and brain | DOC | ND |
| 10 | 55 | F | B | S | 15.0 | 1 | 0 | 0 | 3 | III | + | + | A | MP | NED | NA | |
| 11 | 37 | F | B | S | 55/0 |
3 | NA |
NA |
2 | II | - | + | B | SRC | NED | Done |
|
| 12 | 46 | F | T | A | 85/70 |
3 | 7 | 2 | 3 | III | + | + | A | None | NED | Done |
|
| 13 | 48 | F | B | A | 90/80 |
3 | 1 | 1 | 2 | II | + | + | A | SRC | NED | Done |
|
| 14 | 63 | F | B | S | 16.0 | 1 | 0 | 0 | 3 | III | + | + | A | SRC | NED | Done | |
| 15 | 40 | F | B | A | 30/10 |
2 | 2 | 1 | NA | NA | + | + | NA | NA | NED | Done | |
| 16 | 38 | F | B | S | 12.0 | 1 | 0 | 0 | 2 | II | - | - | A | MP | NED | Done | |
| 17 | 32 | F | T | A | 16.0 | 1 | 0 | 0 | 3 | III | + | + | A | SRC | NED | Done | |
| 18 | 34 | F | B | S | 40.0 | 2 | 0 | 0 | 2 | II | - | - | A | SRC | NED | Done | |
| 19 | 41 | F | T | A | 41.0 | 2 | 2 | 1 | 3 | III | + | + | B | SRC | NED | Done | |
| 20 | 50 | F | B | S | 16.0 | 1 | 0 | 0 | 2 | II | + | + | A | SRC | NED | Done | |
| 21 | 54 | F | T | A | 16/19 |
1 | 22 | 3 | 3 | III | + | + | A | MP | Metastasis to skin and lung | DOC | Done |
| Variable | Total (n = 438) | HER2-negative PMC (n = 417) | HER2-positive PMC (n = 21) | p-value |
|---|---|---|---|---|
| Age (yr) | 49.92 | 50.15 | 45.29 | .073 |
| Sex | ||||
| Female | 431 | 410 | 21 | |
| Male | 7 | 7 | 0 | |
| Tumor size (mm) | 21.3 ± 14.41 | 20.73 ± 13.34 | 32.21 ± 26.55 | < .001 |
| T category | < .001 | |||
| T1 | 242 | 231 (55.5) | 11 (52.4) | |
| T2 | 174 | 169 (40.6) | 5 (23.8) | |
| T3 | 21 | 16 (3.8) | 5 (23.8) | |
| Lymph node status |
.009 | |||
| Negative | 378 | 365 (88.0) | 13 (65.0) | |
| Positive | 57 | 50 (12.0) | 7 (35.0) | |
| Nuclear grade |
< .001 | |||
| 1 | 200 | 200 (48.0) | 0 | |
| 2 | 217 | 207 (49.6) | 10 (50.0) | |
| 3 | 20 | 10 (2.4) | 10 (50.0) | |
| Histologic grade |
< .001 | |||
| I | 248 | 248 (59.5) | 0 | |
| II | 166 | 156 (37.4) | 10 (50.0) | |
| III | 23 | 13 (3.1) | 10 (50.0) | |
| ER | < .001 | |||
| Negative | 12 | 5 (1.2) | 7 (33.3) | |
| Positive | 424 | 410 (98.8) | 14 (66.7) | |
| PR | .005 | |||
| Negative | 36 | 30 (7.2) | 6 (28.6) | |
| Positive | 400 | 385 (92.8) | 15 (71.4) | |
| KI-67 |
.006 | |||
| < 20% | 244 | 236 (84.6) | 8 (53.3) | |
| ≥ 20% | 50 | 43 (15.4) | 7 (46.7) | |
| Type A/B |
.940 | |||
| A | 301 | 288 (69.2) | 13 (68.4) | |
| B | 134 | 128 (30.8) | 6 (31.6) | |
| EIC |
.011 | |||
| Negative | 328 | 318 (78.1) | 10 (50.0) | |
| Positive | 99 | 89 (21.9) | 10 (50.0) | |
| LVI |
.158 | |||
| Absent | 346 | 331 (87.8) | 15 (75.0) | |
| Present | 51 | 46 (12.2) | 5 (25.0) | |
| MP |
.012 | |||
| Absent | 207 | 192 (46.2) | 15 (75.0) | |
| Present | 229 | 224 (53.8) | 5 (25.0) | |
| SRC |
< .001 | |||
| Absent | 376 | 368 (88.5) | 8 (40.0) | |
| Present | 60 | 48 (11.5) | 12 (60.0) | |
| Operation | .182 | |||
| Excision | 7 | 7 (1.7) | 0 | |
| Conserving surgery | 299 | 288 (69.1) | 11 (52.4) | |
| Total mastectomy | 132 | 122 (29.3) | 10 (47.6) | |
| Lymph node dissection | .011 | |||
| Sentinel biopsy | 329 | 318 (76.8) | 11 (52.4) | |
| Axillary dissection | 106 | 96 (23.2) | 10 (47.6) | |
| Chemotherapy |
< .001 | |||
| No | 320 | 315 (76.1) | 5 (25.0) | |
| Yes | 114 | 99 (23.9) | 15 (75.0) | |
| Trastuzumab treatment |
||||
| No | 9 (45.0) | |||
| Yes | 11 (55.0) | |||
| Radiotherapy |
.199 | |||
| No | 119 | 111 (26.9) | 8 (40.0) | |
| Yes | 314 | 302 (73.1) | 12 (60.0) | |
| Hormone therapy |
.001 | |||
| No | 11 | 7 (1.7) | 4 (20.0) | |
| Yes | 420 | 404 (98.3) | 16 (80.0) |
| p-value |
||
|---|---|---|
| DFS | OS | |
| T category | .003 | .072 |
| Node metastasis | < .001 | .011 |
| Nuclear grade | .003 | .548 |
| Histologic grade | .021 | .494 |
| ER | .588 | .103 |
| PR | .296 | .755 |
| HER2 | .001 | .026 |
| Ki-67 (≥ 20%) | .395 | - |
| Type A/B | .127 | .877 |
| Structure (MP) | .761 | .085 |
| Structure (SRC) | .788 | .515 |
| EIC | .772 | .914 |
| LVI | < .001 | .127 |
| DFS |
OS |
|||
|---|---|---|---|---|
| Multivariate RR (95% CI) | p-value | Multivariate RR (95% CI) | p-value | |
| T category | ||||
| 1 | 1 | .535 | - | |
| 2 | 1.069 (0.275–4.156) | .924 | ||
| 3 | 2.892 (0.411–20.324) | .286 | ||
| Node metastasis | 4.818 (1.609–14.424) | .005 | 11.724 (1.059–129.775) | .045 |
| Nuclear grade | ||||
| 1 | 1 | .629 | - | |
| 2 | 2.532 (0.345–18.608) | .361 | ||
| 3 | 5.113 (0.046–565.687) | .497 | ||
| Histologic grade | ||||
| I | 1 | .977 | - | |
| II | 1.091 (0.207–5.742) | .918 | ||
| III | 0.731 (0.008–66.579) | .892 | ||
| HER2 | 7.822 (2.130–28.722) | .002 | 2.738 (0.189–39.568) | .460 |
| LVI | 2.355 (0.559–9.928) | .243 | - | |
HER2, human epidermal growth factor receptor 2; ER, estrogen receptor; PR, progesterone receptor; F, female; T, total mastectomy; A, axillary lymph node dissection; SRC, signet ring cells; NED, no evidence of disease; ND, not done; B, breast conserving surgery; S, sentinel lymph node biopsy; MP, micropapillary; DOD, died of disease; NA, not applicable; DOC, died of other cause. For cases with neoadjuvant chemotherapy, tumor size before/after treatment were recorded; In this patient, lymph node metastasis was suspected in radiologic images, but pathologic confirmation was not performed due to pathologic complete response; Used trastuzumab for neoadjuvant chemotherapy.
Values are presented as number (%) or mean ± standard deviation. HER2, human epidermal growth factor receptor 2; PMC, pure mucinous carcinoma; ER, estrogen receptor; PR, progesterone receptor; EIC, extensive intraductal component; LVI, lymphovascular invasion; MP, micropapillary pattern; SRC, signet ring cell pattern. There are some missing data.
DFS, disease-free survival; OS, overall survival; ER, estrogen receptor; PR, progesterone receptor; MP, micropapillary pattern; SRC, signet ring cell pattern; EIC, extensive intraductal component; LVI, lymphovascular invasion.
DFS, disease-free survival; OS, overall survival; RR, relative risk; CI, confidence interval; HER2, human epidermal growth factor receptor 2; LVI, lymphovascular invasion.

