 E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 56(3); 2022 > Article
-
Original Article
Frequency of PIK3CA mutations in different subsites of head and neck squamous cell carcinoma in southern Thailand -
Arunee Dechaphunkul1
 , Phatcharaporn Thongwatchara1, Paramee Thongsuksai2, Tanadech Dechaphunkul3, Sarayut Lucien Geater4
, Phatcharaporn Thongwatchara1, Paramee Thongsuksai2, Tanadech Dechaphunkul3, Sarayut Lucien Geater4 -
Journal of Pathology and Translational Medicine 2022;56(3):126-133.
DOI: https://doi.org/10.4132/jptm.2022.01.04
Published online: February 28, 2022
1Holistic Center for Cancer Study and Care (HOCC-PSU), Medical Oncology Unit, Department of Internal Medicine, Faculty of Medicine, Prince of Songkla University, Songkhla, Thailand
2Department of Pathology, Faculty of Medicine, Prince of Songkla University, Songkhla, Thailand
3Department of Otorhinolaryngology Head and Neck Surgery, Faculty of Medicine, Prince of Songkla University, Songkhla, Thailand
4Division of Respiratory and Respiratory Critical Care Medicine, Department of Internal Medicine, Faculty of Medicine, Prince of Songkla University, Songkhla, Thailand
- Corresponding Author: Arunee Dechaphunkul, MD, Holistic Center for Cancer Study and Care (HOCC-PSU), Medical Oncology Unit, Department of Internal Medicine, Faculty of Medicine, Prince of Songkla University, Songkhla 90110, Thailand, Tel: +6674-455856, Fax: +6674-451469, E-mail: dr.arunee@gmail.com
© 2022 The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
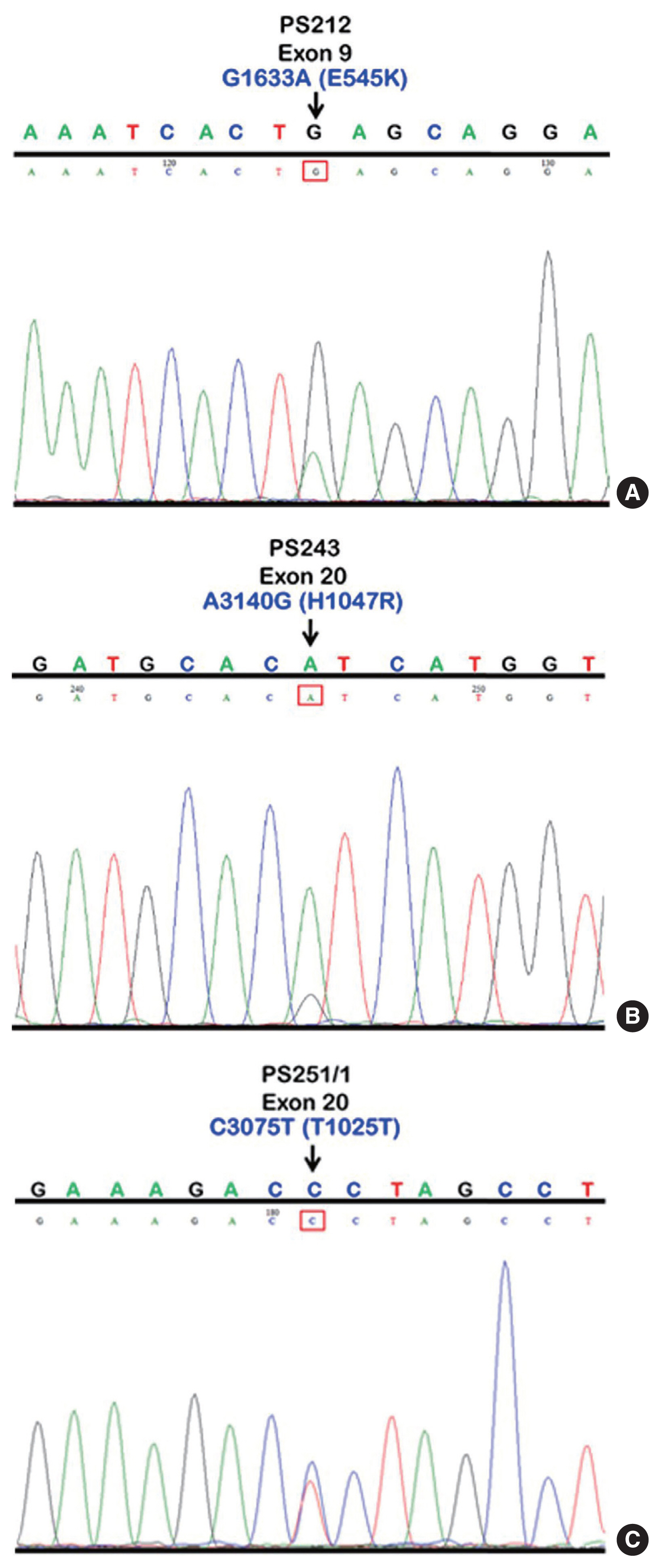
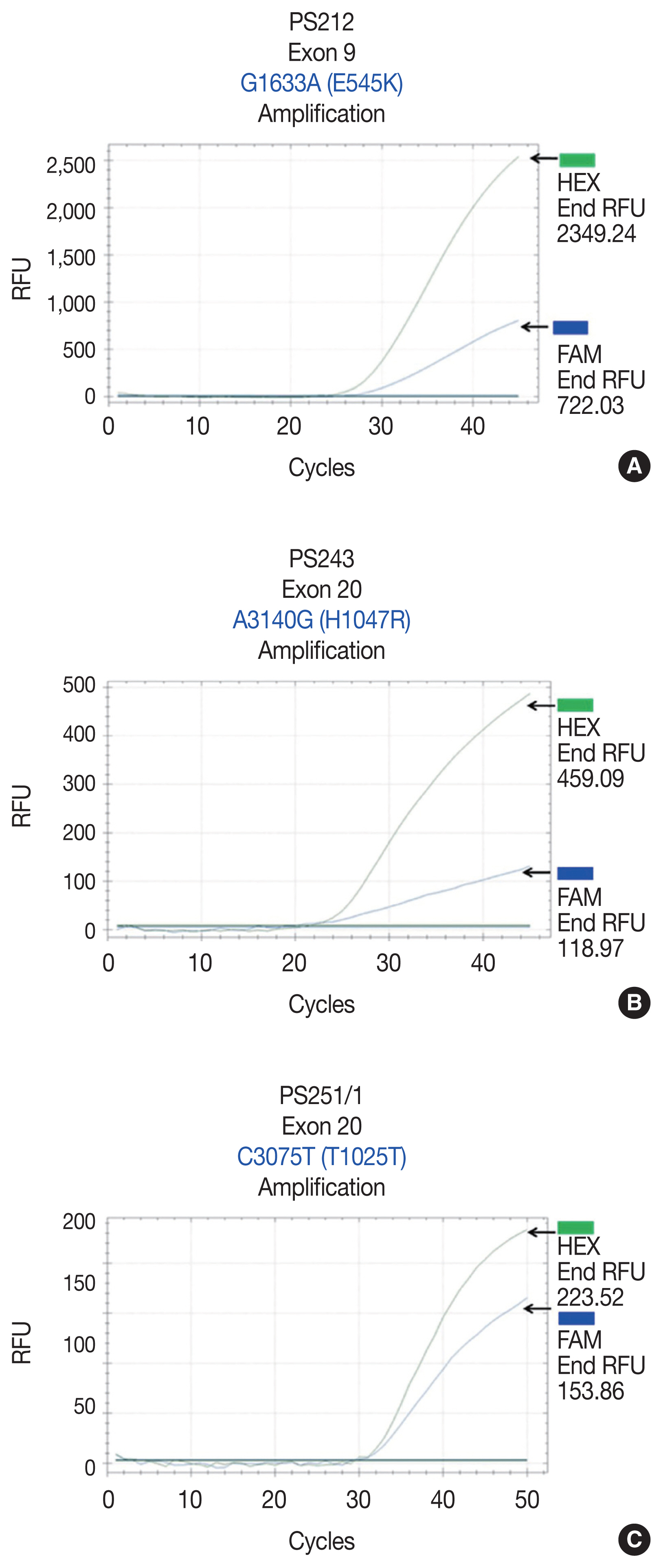
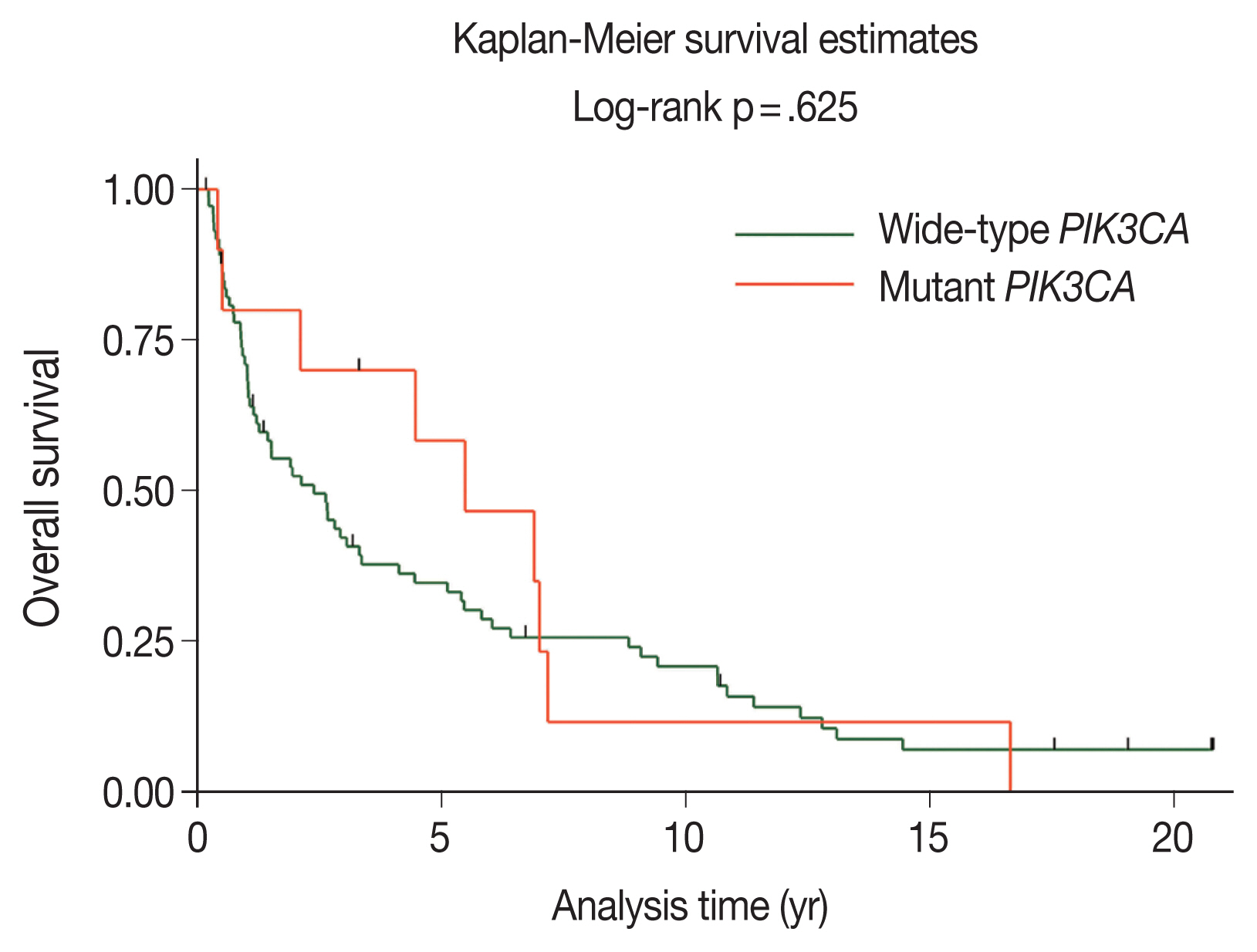
Figure & Data
References
Citations
- Comprehensive Genomic Profiling of Sinonasal Carcinomas: Identification of Common Mutations and Potential Targets for Therapy
Gabriel Bitar, Beau Hsia, Saif Alshaka, Bastien A. Valencia, Jeeho Kim, Mariko Sato, John Crawford, Michael L. Levy, Sean Polster, Vijay A. Patel
Journal of Neurological Surgery Part B: Skull Base.2025;[Epub] CrossRef - Anti-breast cancer effects of Pterocarpus soyauxii Taub aqueous extract and its compounds by integrating ADMET, network pharmacology, molecular docking, dynamic simulation, CLC-Pred and pdCSM-Cancer/PPI approaches, and in vitro validation
Owona Pascal Emmanuel, Mengue Ngadena Yolande Sandrine, Bilanda Danielle Claude, Ayissi Mbomo Rigobert-Espoir, Oluwafemi Adeleke Ojo, Ella Armand Fils, Bidingha A Goufani Ronald, Bindzi Georges Michel, Dzeufiet Djomeni Paul Désiré, Tariq Aziz, Abdulhakeem
Journal of Ethnopharmacology.2025; 353: 120407. CrossRef - A retrospective study of laryngeal squamous cell carcinoma and the significance of the PIK3CA mutation for survival
Akinobu Kubota, Nobuyuki Bandoh, Takashi Goto, Michihisa Kono, Ryosuke Sato, Shiori Suzuki, Shota Sakaue, Ryuhei Takeda, Shuto Hayashi, Misaki Hayashi, Daisuke Araki, Shogo Baba, Yasutaka Kato, Miki Takahara, Hiroshi Nishihara, Hajime Kamada
Molecular and Clinical Oncology.2025; 23(4): 1. CrossRef - An empirical review on the resistance mechanisms of epidermal growth factor receptor inhibitors and predictive molecular biomarkers in colorectal cancer
Sankha Bhattacharya
Critical Reviews in Oncology/Hematology.2023; 183: 103916. CrossRef
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-
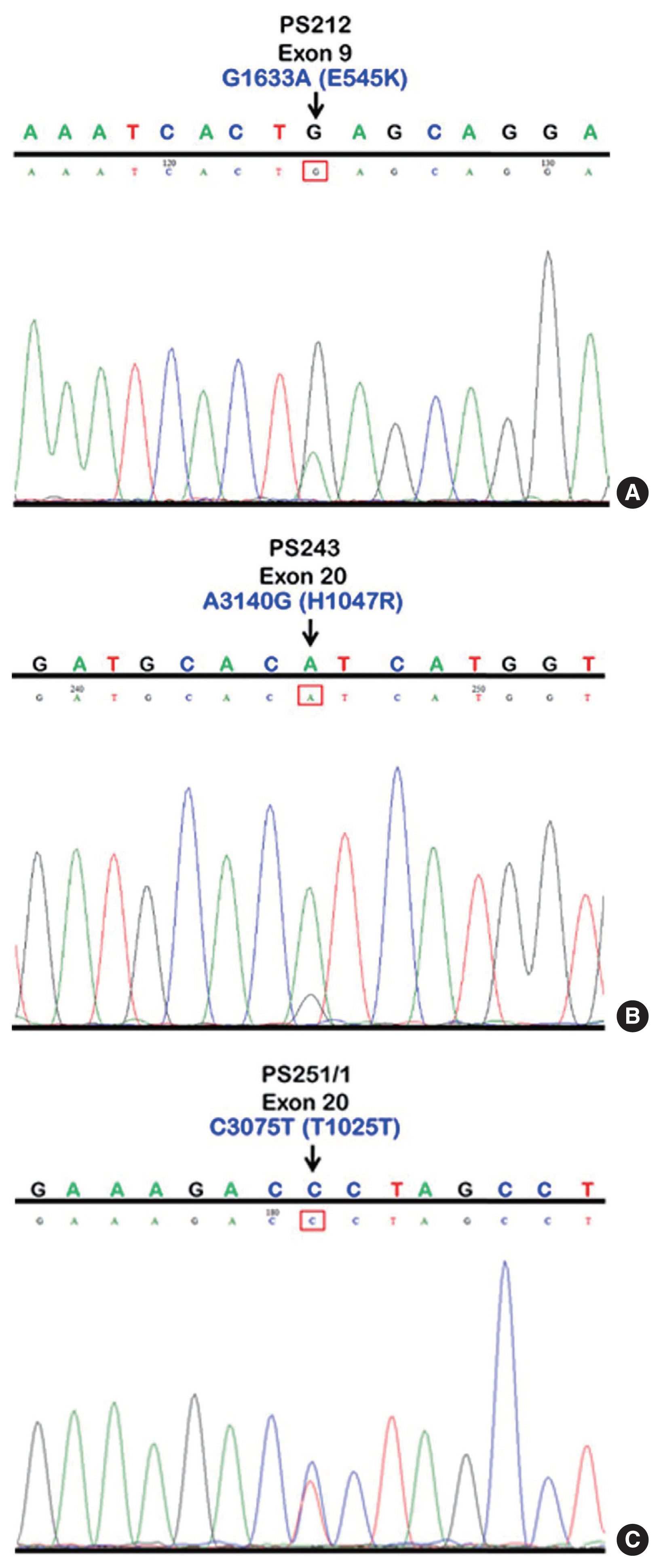
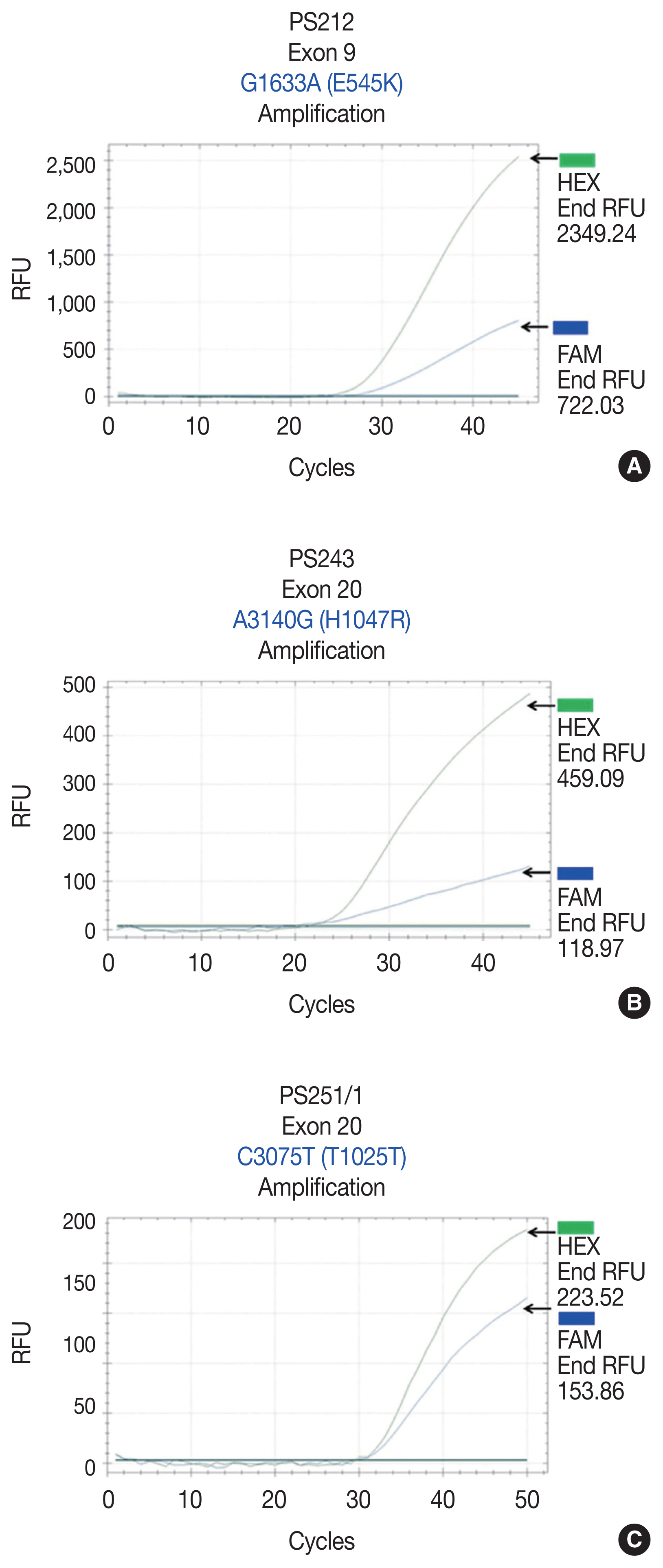
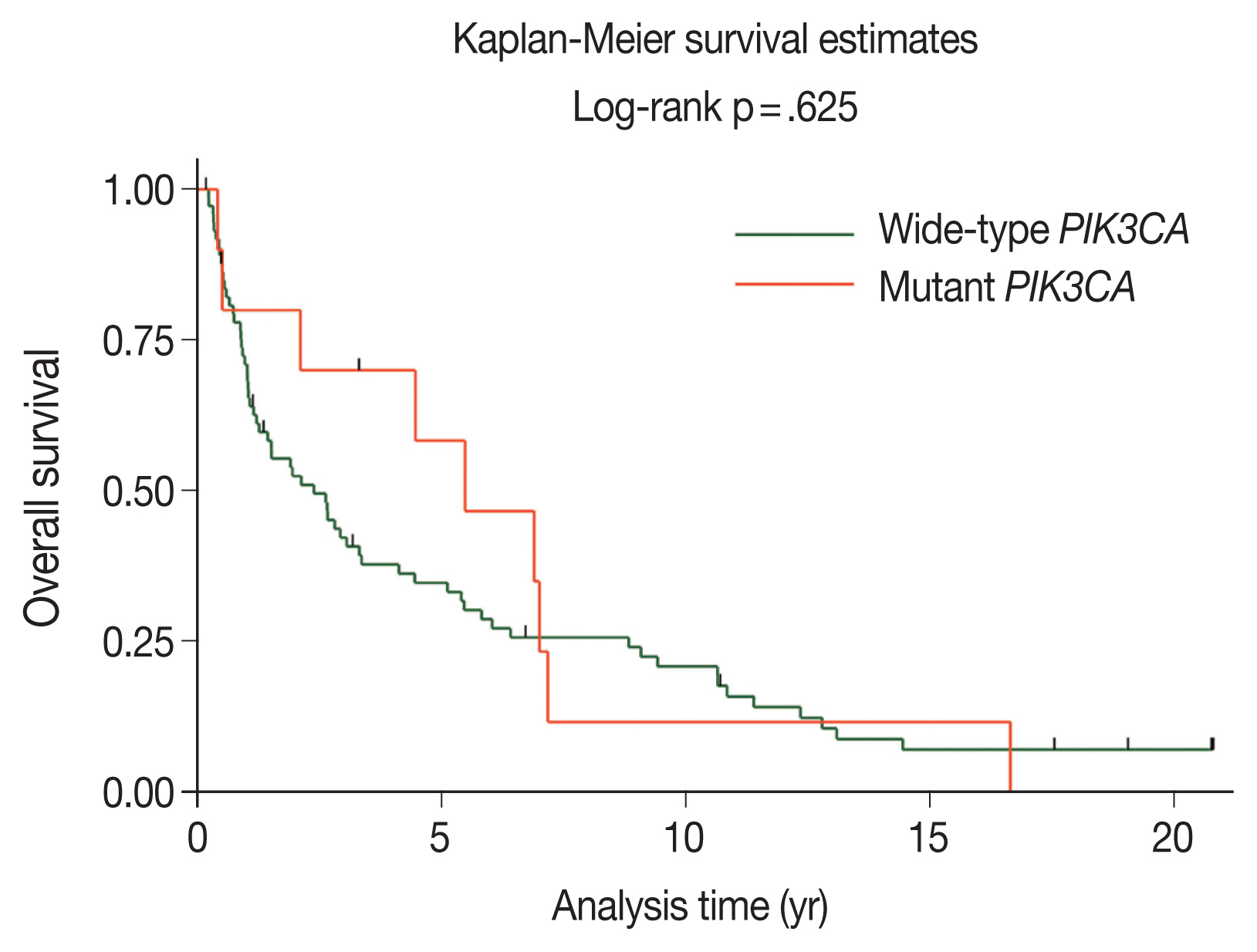



Fig. 1
Fig. 2
Fig. 3
| Probe name | Type | Sequence |
|---|---|---|
| PIK3CA exon 9 G>A | Wild-type probe | 5′-(HEX) CTCTCTGAAATCACTGAGCAGGAGAA (BHQ-1)-3′ |
| PIK3CA exon 9 G>A | Mutated probe | 5′-(FAM) CTCTCTGAAATCACTAAGCAGGAGAA (BHQ-1)-3′ |
| PIK3CA exon 20 A>G | Wild-type probe | Anti-sense 5′ (HEX) AGCCACCATGATGTGCATCATTC (BHQ-1)-3′ |
| PIK3CA exon 20 A>G | Mutated probe | Anti-sense 5′ (FAM) AGCCACCATGACGTGCATCATTC (BHQ-1)-3′ |
| PIK3CA exon 20 C>T | Wild-type probe | 5′-(HEX) ACATTCGAAAGACCCTAGCCTTAGAT (BHQ-1)-3′ |
| PIK3CA exon 20 C>T | Mutated probe | 5′-(FAM) ACATTCGAAAGACTCTAGCCTTAGAT (BHQ-1)-3′ |
| Variable | Total (n = 84) | Wild-type PIK3CA (n = 74) | Mutant PIK3CA (n = 10) | p-value |
|---|---|---|---|---|
| Age (yr) | .100 | |||
| Median ± SD | 68 ± 12.6 | 68 ± 12.8 | 70 ± 9.7 | |
| Sex | .307 | |||
| Male | 49 (58.3) | 45 (60.8) | 4 (40.0) | |
| Female | 35 (41.7) | 29 (39.2) | 6 (60.0) | |
| Smoking | .324 | |||
| Yes | 47 (56.0) | 43 (58.1) | 4 (40.0) | |
| No | 37 (44.0) | 31 (41.9) | 6 (60.0) | |
| Alcohol drinking | .182 | |||
| Yes | 44 (52.4) | 41 (55.4) | 3 (30.0) | |
| No | 40 (47.6) | 33 (44.6) | 7 (70.0) | |
| Tumor location | .380 | |||
| Oral cavity | 57 (67.9) | 51 (68.9) | 6 (60.0) | |
| Tongue | 14 (16.7) | 13 (17.6) | 1 (10.0) | |
| Gums | 13 (15.4) | 12 (16.2) | 1 (10.0) | |
| Buccal mucosa | 11 (13.1) | 10 (13.5) | 1 (10.0) | |
| Floor of mouth | 6 (7.1) | 5 (6.7) | 1 (10.0) | |
| Lip | 5 (6.0) | 3 (4.1) | 2 (20.0) | |
| Hard palate | 4 (4.8) | 4 (5.4) | 0 | |
| Retromolar area | 2 (2.4) | 2 (2.7) | 0 | |
| Oral cavity (unspecified) | 2 (2.4) | 2 (2.7) | 0 | |
| Oropharynx | 6 (7.1) | 6 (8.1) | 0 | |
| Base of tongue | 6 (7.1) | 6 (8.1) | 0 | |
| Hypopharynx | 21 (25.0) | 17 (23.0) | 4 (40.0) | |
| Pyriform sinus | 21 (25.0) | 17 (23.0) | 4 (40.0) | |
| Clinical stage | .628 | |||
| I | 16 (19.0) | 14 (18.9) | 2 (20.0) | |
| II | 17 (20.3) | 13 (17.6) | 4 (40.0) | |
| III | 19 (22.6) | 18 (24.3) | 1 (10.0) | |
| IVa | 29 (34.5) | 26 (35.1) | 3 (30.0) | |
| IVb | 1 (1.2) | 1 (1.4) | 0 | |
| IVc | 2 (2.4) | 2 (2.7) | 0 | |
| Treatment | .337 | |||
| Surgery | 23 (27.4) | 18 (24.3) | 5 (50.0) | |
| Surgery followed by RT | 42 (50.0) | 38 (51.4) | 4 (40.0) | |
| RT | 13 (15.5) | 12 (16.2) | 1 (10.0) | |
| Best supportive care | 6 (7.1) | 6 (8.1) | 0 |
| Subsites of HNSCC | PIK3CA mutation | Overall PIK3CA mutations | |
|---|---|---|---|
|
| |||
| Exon 9 | Exon 20 | ||
| Oral cavity | 0/63 (0) | 6/63 (9.5) | 6/63 (9.5) |
| Oropharynx | 0/10 (0) | 0/10 (0) | 0/10 (0) |
| Hypopharynx | 2/23 (8.7) | 2/23 (8.7) | 4/23 (17.4) |
| Sample No. | Age at diagnosis (yr) | Sex | Tumor location | Exon | Nucleotide | Codon change | Amino acid change | Type of mutation |
|---|---|---|---|---|---|---|---|---|
| PS212 | 76 | Male | Pyriform sinus | 9 | G1633A | GAG to AAG | E545K | Missense |
| PS220 | 62 | Female | Pyriform sinus | 9 | G1633A | GAG to AAG | E545K | Missense |
| PS243 | 72 | Male | Pyriform sinus | 20 | A3140G | CAT to CGT | H1047R | Missense |
| PS251/1 | 63 | Male | Pyriform sinus | 20 | C3075T | ACC to ACT | T1025T | Silent |
| OR183 | 58 | Female | Buccal mucosa | 20 | C3075T | ACC to ACT | T1025T | Silent |
| OR214 | 90 | Female | Tongue | 20 | C3075T | ACC to ACT | T1025T | Silent |
| OR378 | 79 | Female | Gums | 20 | C3075T | ACC to ACT | T1025T | Silent |
| OR391 | 69 | Male | Floor of mouth | 20 | C3075T | ACC to ACT | T1025T | Silent |
| OR205 | 79 | Female | Lip | 20 | A3140G | CAT to CGT | H1047R | Missense |
| OR209 | 66 | Female | Lip | 20 | A3140G | CAT to CGT | H1047R | Missense |
| Authors (year) | Location of HNSCC | PIK3CA mutations (%) | Type of mutation | Exons |
|---|---|---|---|---|
| Qiu et al. (2006) [ |
HNSCC | 11 (4/38) | Point mutation | 4, 9, and 20 |
| Kozaki et al. (2006) [ |
Oral cavity | 9 (11/122) | Point mutation | 9 and 20 |
| Qiu et al. (2008) [ |
Pharynx | 21 (5/24) | Point mutation | 9 and 20 |
| Murugan et al. (2008) [ |
HNSCC | 13 (7/54) | Point mutations, frameshift | 9 and 20 |
| Kommineni et al. (2015) [ |
HNSCC | 60.46 | Point mutation | 9 and 20 |
| Wu et al. (2017) [ |
Hypopharynx | 13.6 | Point mutation | 9 and 20 |
| Beaty et al. (2020) [ |
Oropharynx | 21 (16/77) | Point mutation | 9 and 13 |
| Lui et al. (2013) [ |
HNSCC | 12.6 (19/151) | Point mutation | 9, 20, and novel mutations |
Values are presented as number (%) unless otherwise indicated.
Values are presented as number (%).

