 E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 46(6); 2012 > Article
-
Original Article
Prognostic Relevance of the Expression of CA IX, GLUT-1, and VEGF in Ovarian Epithelial Cancers - Kyungbin Kim1, Won Young Park1, Jee Yeon Kim1,2, Mee Young Sol2,3, Dong Hun Shin2,3, Do Youn Park1,2, Chang Hun Lee1,2, Jeong Hee Lee3, Kyung Un Choi2,3,4
-
Korean Journal of Pathology 2012;46(6):532-540.
DOI: https://doi.org/10.4132/KoreanJPathol.2012.46.6.532
Published online: December 26, 2012
1Department of Pathology, Pusan National University Hospital, Pusan National University School of Medicine, Yangsan, Korea.
2Department of Pathology, Pusan National University School of Medicine, Yangsan, Korea.
3Department of Pathology, Pusan National University Yangsan Hospital, Pusan National University School of Medicine, Yangsan, Korea.
4Research Institute for Convergence of Biomedical Science and Technology, Pusan National University Yangsan Hospital, Pusan National University School of Medicine, Yangsan, Korea.
- Corresponding Author: Kyung Un Choi, M.D. Department of Pathology, Pusan National University Yangsan Hospital, Pusan National University School of Medicine, 20 Geumo-ro, Yangsan 626-787, Korea. Tel: +82-55-360-1862, Fax: +82-55-360-1865, kuchoi@pusan.ac.kr
© 2012 The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
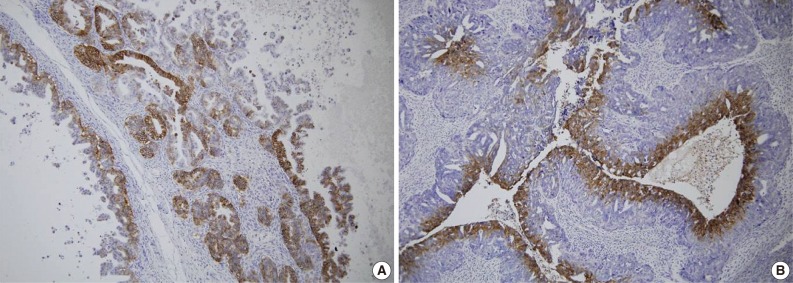
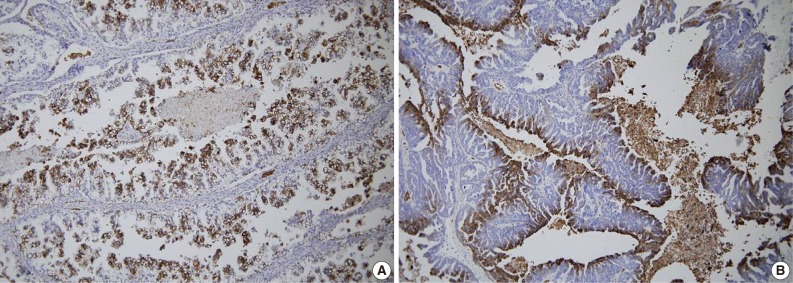
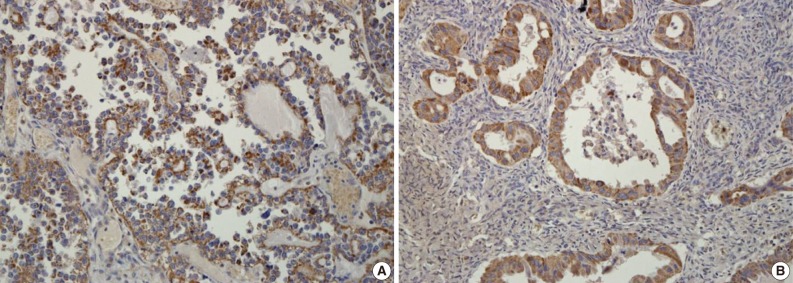
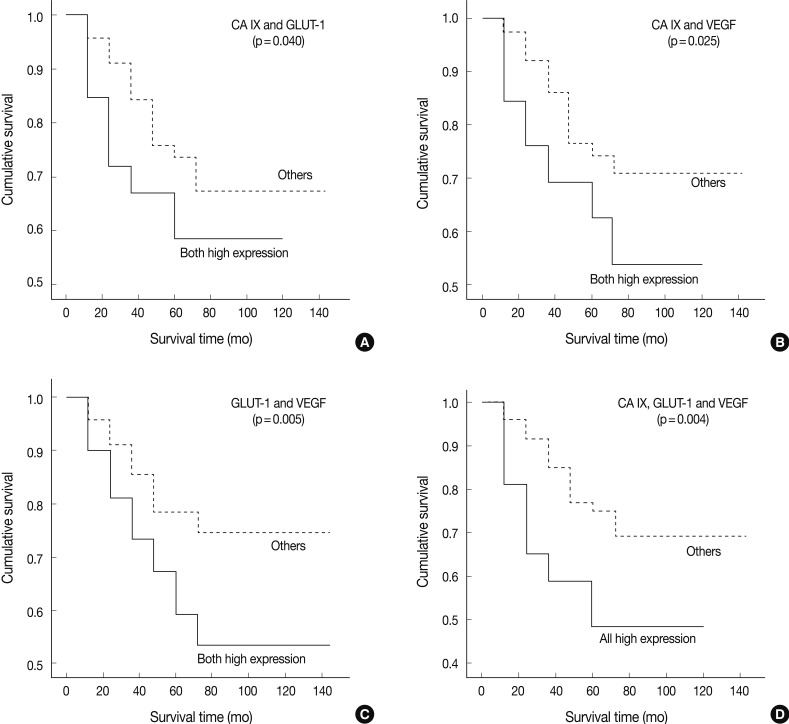
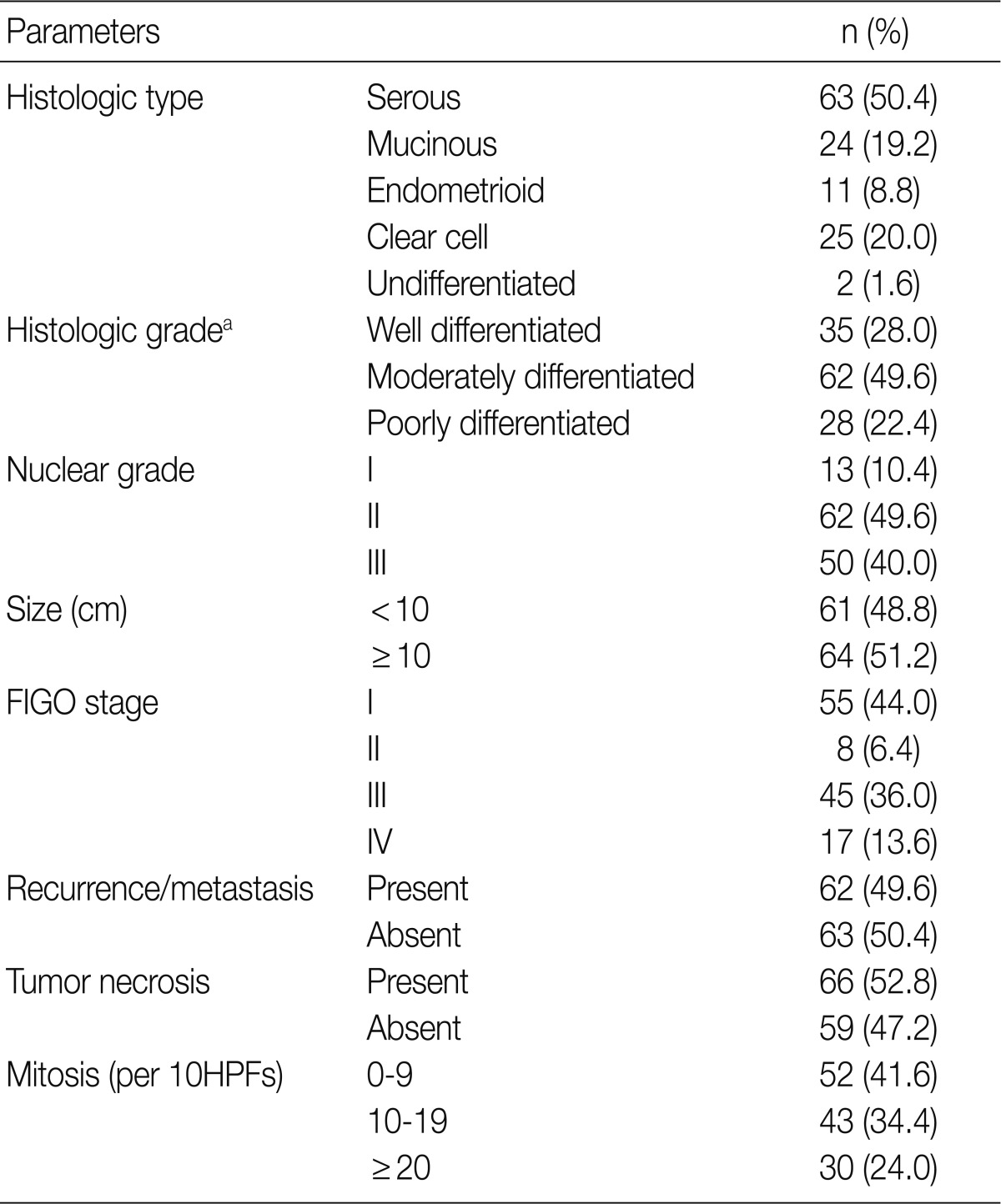
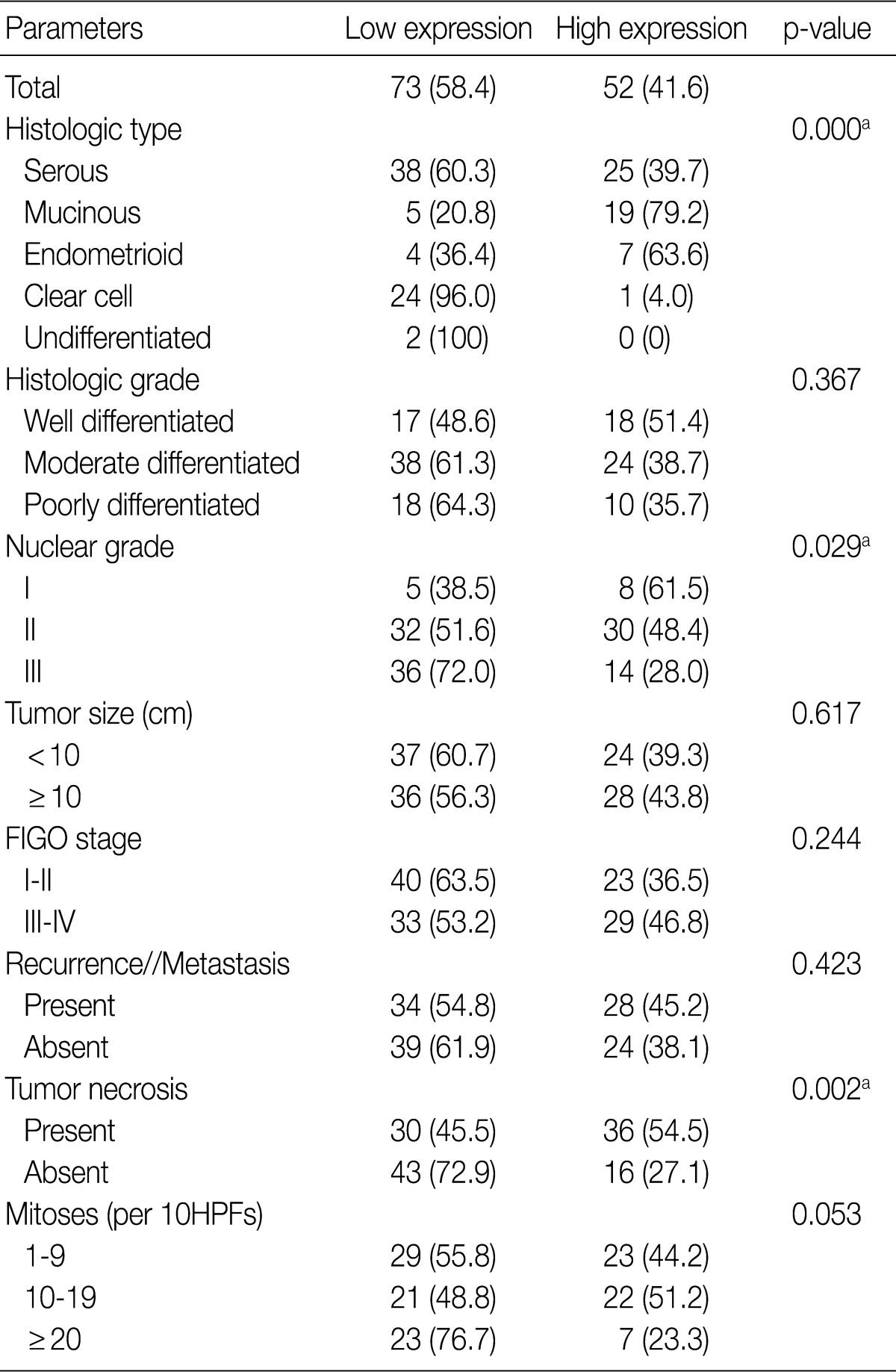
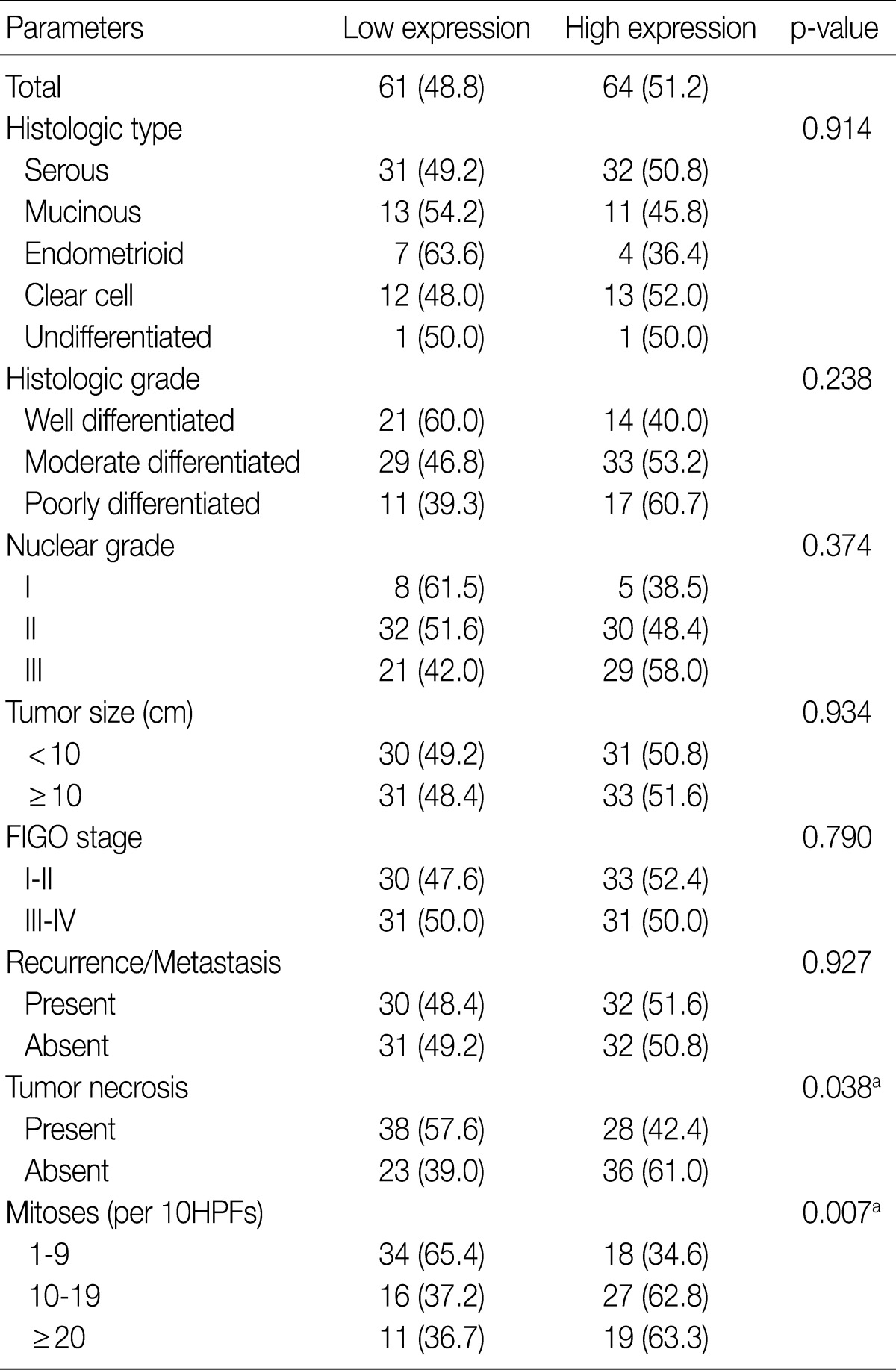
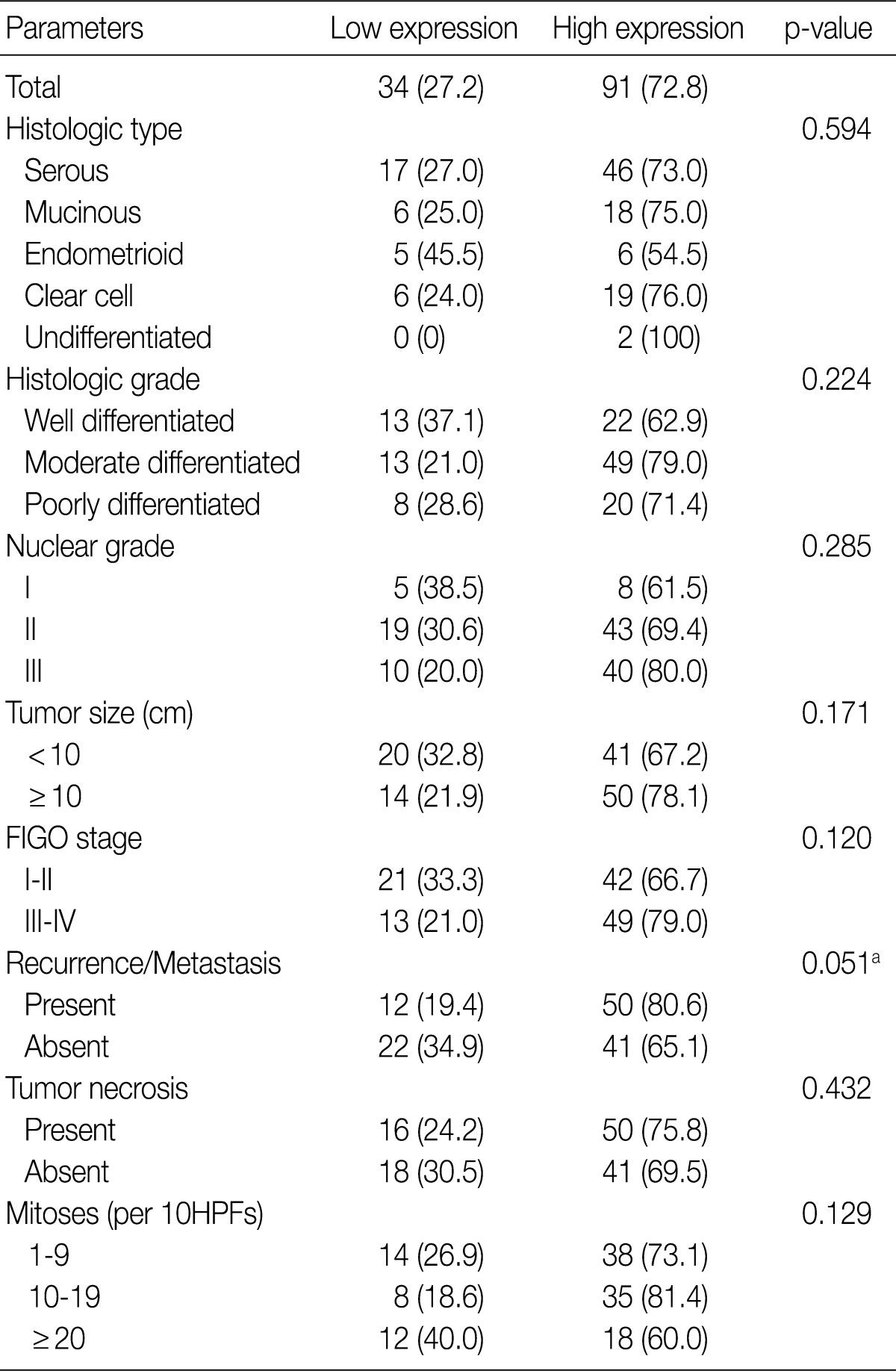
Figure & Data
References
Citations
- Glucose-transporter 1 (GLUT1) as a prognostic biomarker: evidence from 14,966 human tumors across 134 cancer types
Seyma Büyücek, Katharina Möller, Florian Viehweger, Ria Schlichter, Anne Menz, Andreas M Luebke, Viktor Reiswich, Martina Kluth, Claudia Hube-Magg, Andrea Hinsch, Florian Lutz, Sören Weidemann, Frank Jacobsen, Maximilian Lennartz, David Dum, Christian Ber
BMC Cancer.2026;[Epub] CrossRef - Role of Carbonic Anhydrase IX Expression in Triple-negative Breast Cancer
Hemali B Kotadiya, Nupur A Patel, Hemangini H Vora
Gujarat Cancer Society Research Journal.2026; 27(2): 31. CrossRef - Evaluation of the effect of Endogenous and Exogenous Antioxidants on Hypoxia Induced Breast Adenocarcinoma Cell Invasion and Migration:
In vitro
Subarnarekha Maitra, Poulami Sen, Dibya Sinha, Tathagata Roy
Research Journal of Pharmacy and Technology.2025; : 3153. CrossRef - Effect of Ultrasound Therapy at the ST11 on Sympathetic Nervous System Change: A Prospective Randomized Controlled Study
Shinwoo Kang, Dongho Keum
Journal of Korean Medicine Rehabilitation.2023; 33(4): 167. CrossRef - A systematic review verified by bioinformatic analysis based on TCGA reveals week prognosis power of CAIX in renal cancer
Zikuan Zhang, Bo Wu, Yuan Shao, Yongquan Chen, Dongwen Wang, Lucia Magnelli
PLOS ONE.2022; 17(12): e0278556. CrossRef - Effect of Acupuncture at the Field of the Auricular Branch of the Vagus Nerve on Autonomic Nervous System Change
Sunjoo An, Dongho Keum
Journal of Korean Medicine Rehabilitation.2021; 31(2): 81. CrossRef - Responses of Autonomic Nervous System and Gastrointestinal Function to Acupuncture at Abdominal Anterior Cutaneous Nerve : A Pilot Study
Seohyun Park, Hojun Kim, Dongho Keum
Journal of Korean Medicine.2019; 40(1): 99. CrossRef - Omega-3 polyunsaturated fatty acid docosahexaenoic acid and its role in exhaustive-exercise-induced changes in female rat ovulatory cycle
Abeer F. Mostafa, Shereen M. Samir, R.M. Nagib
Canadian Journal of Physiology and Pharmacology.2018; 96(4): 395. CrossRef - Clear cell carcinomas of the ovary and kidney: clarity through genomics
Jennifer X Ji, Yi Kan Wang, Dawn R Cochrane, David G Huntsman
The Journal of Pathology.2018; 244(5): 550. CrossRef - Prognostic Significance of Carbonic Anhydrase IX Expression in Cancer Patients: A Meta-Analysis
Simon J. A. van Kuijk, Ala Yaromina, Ruud Houben, Raymon Niemans, Philippe Lambin, Ludwig J. Dubois
Frontiers in Oncology.2016;[Epub] CrossRef - Review of Research Topics on Abdominal Examination
Jihye Kim, Jeong Hwan Park, Keun Ho Kim
Journal of Korean Medicine.2016; 37(3): 1. CrossRef - Expression of hypoxic markers and their prognostic significance in soft tissue sarcoma
JEUNG IL KIM, KYUNG UN CHOI, IN SOOK LEE, YOUNG JIN CHOI, WON TACK KIM, DONG HOON SHIN, KYUNGBIN KIM, JEONG HEE LEE, JEE YEON KIM, MEE YOUNG SOL
Oncology Letters.2015; 9(4): 1699. CrossRef - Evaluation of a Hypoxia Regulated Gene Panel in Ovarian Cancer
Amanda F. Baker, Scott W. Malm, Ritu Pandey, Cindy Laughren, Haiyan Cui, Denise Roe, Setsuko K. Chambers
Cancer Microenvironment.2015; 8(1): 45. CrossRef - Sulforaphane reduces molecular response to hypoxia in ovarian tumor cells independently of their resistance to chemotherapy
MICHAL PASTOREK, VERONIKA SIMKO, MARTINA TAKACOVA, MONIKA BARATHOVA, MARIA BARTOSOVA, LUBA HUNAKOVA, OLGA SEDLAKOVA, SONA HUDECOVA, OLGA KRIZANOVA, FRANCK DEQUIEDT, SILVIA PASTOREKOVA, JAN SEDLAK
International Journal of Oncology.2015; 47(1): 51. CrossRef - Overexpression of Glucose Transporter-1 (GLUT-1) Predicts Poor Prognosis in Epithelial Ovarian Cancer
Hanbyoul Cho, You Sun Lee, Julie Kim, Joon-Yong Chung, Jae-Hoon Kim
Cancer Investigation.2013; 31(9): 607. CrossRef - Towards Lipidomics of Low-Abundant Species for Exploring Tumor Heterogeneity Guided by High-Resolution Mass Spectrometry Imaging
Jonathan Cimino, David Calligaris, Johann Far, Delphine Debois, Silvia Blacher, Nor Sounni, Agnès Noel, Edwin De Pauw
International Journal of Molecular Sciences.2013; 14(12): 24560. CrossRef
 PubReader
PubReader Cite this Article
Cite this Article
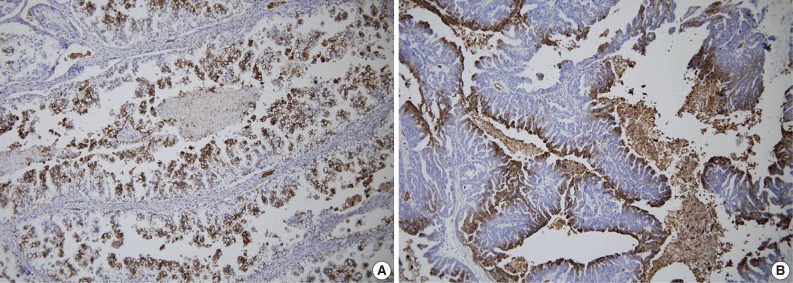
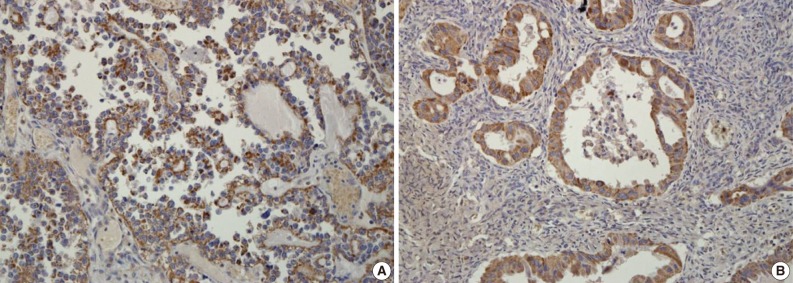
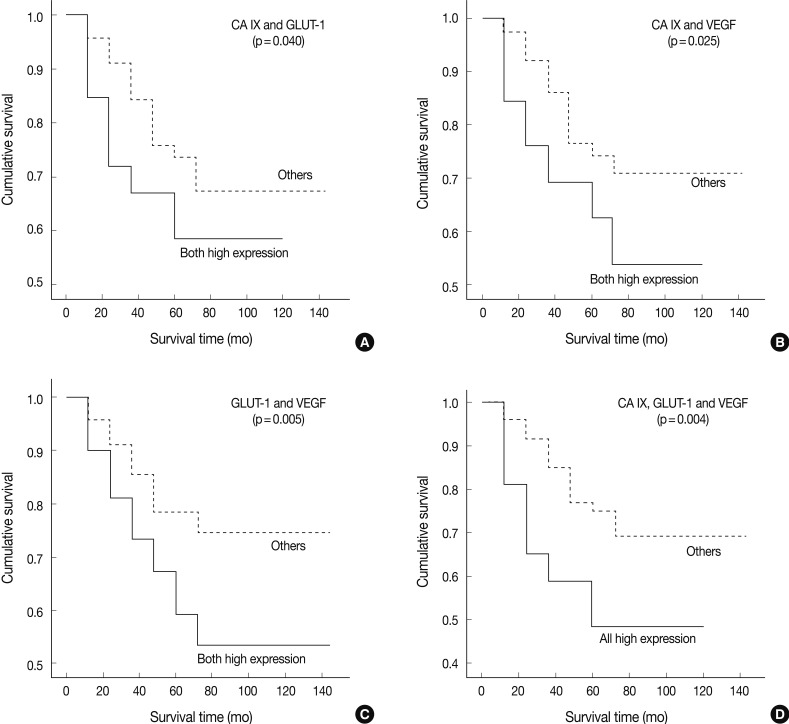




Fig. 1
Fig. 2
Fig. 3
Fig. 4
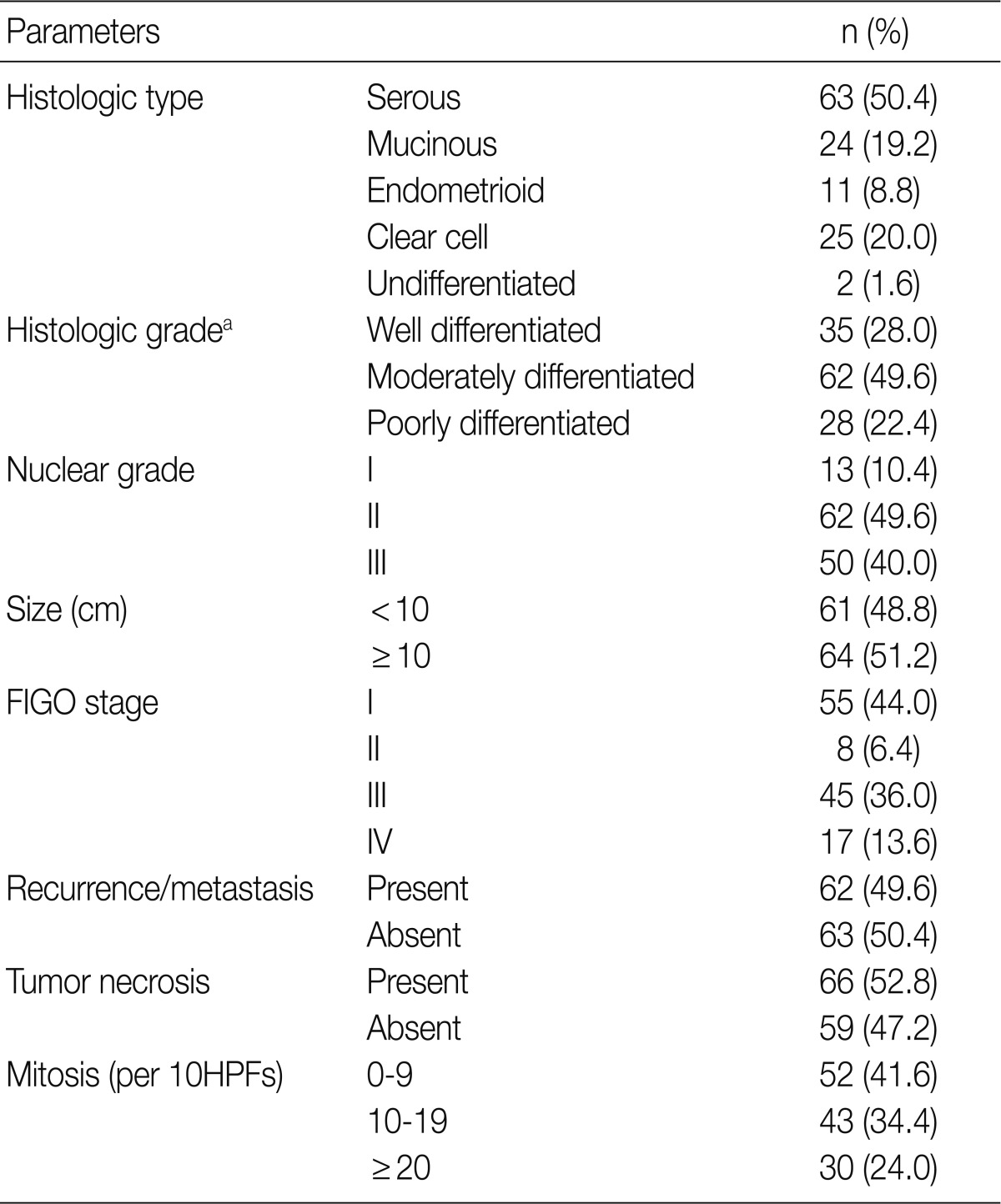
FIGO, Federation of Gynecology and Obstetrics; HPF, high power field. aSilverberg tumor grade system.
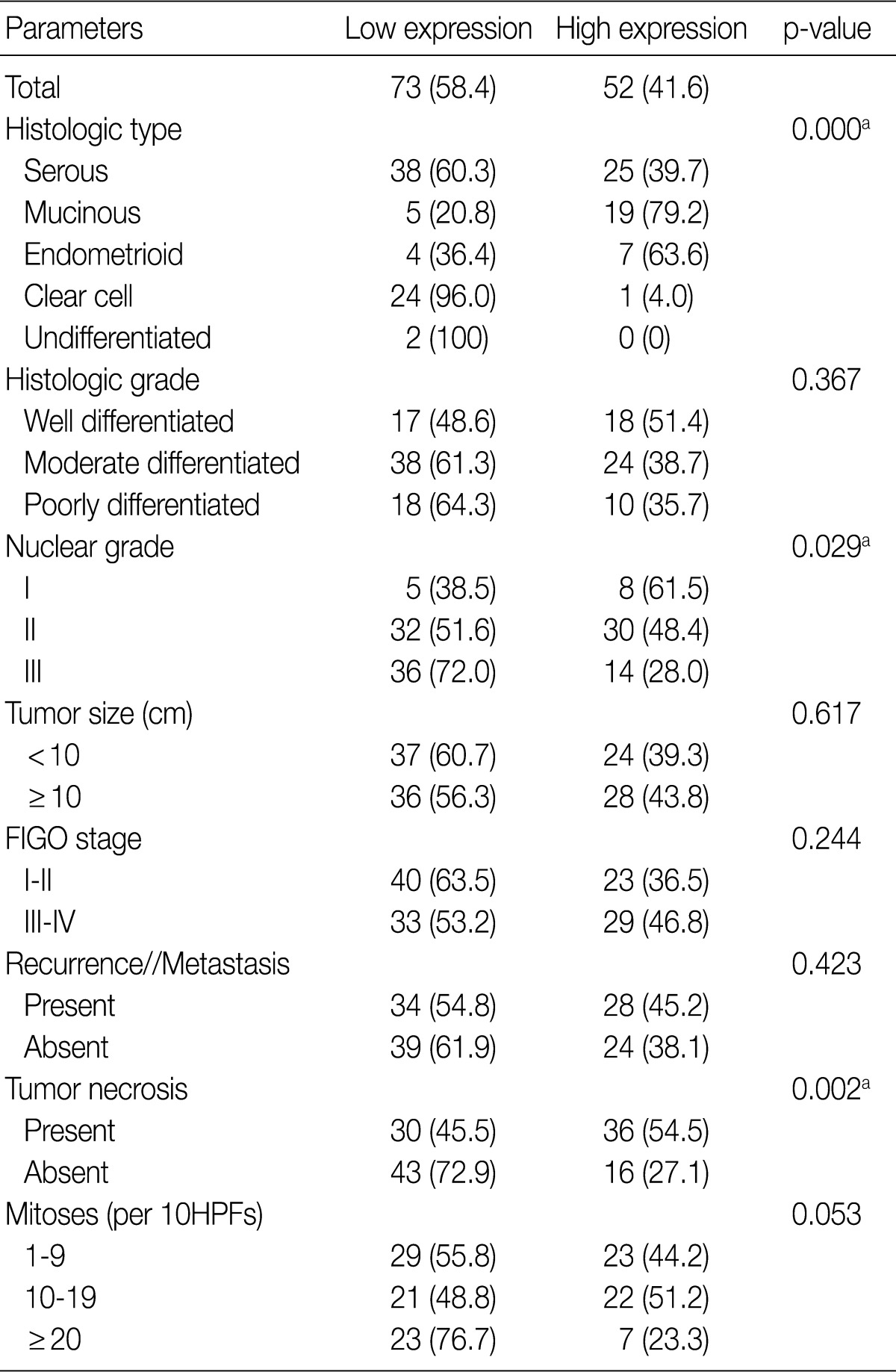
Values are presented as number (%). Low expression, less than 10% positive staining of tumor cells; high expression, more than 10% positive staining of tumor cells. CA IX, carbonic anhydrase IX; FIGO, Federation of Gynecology and Obstetrics; HPF, high power field. aStatistically significance (Pearson's chi-squared test).
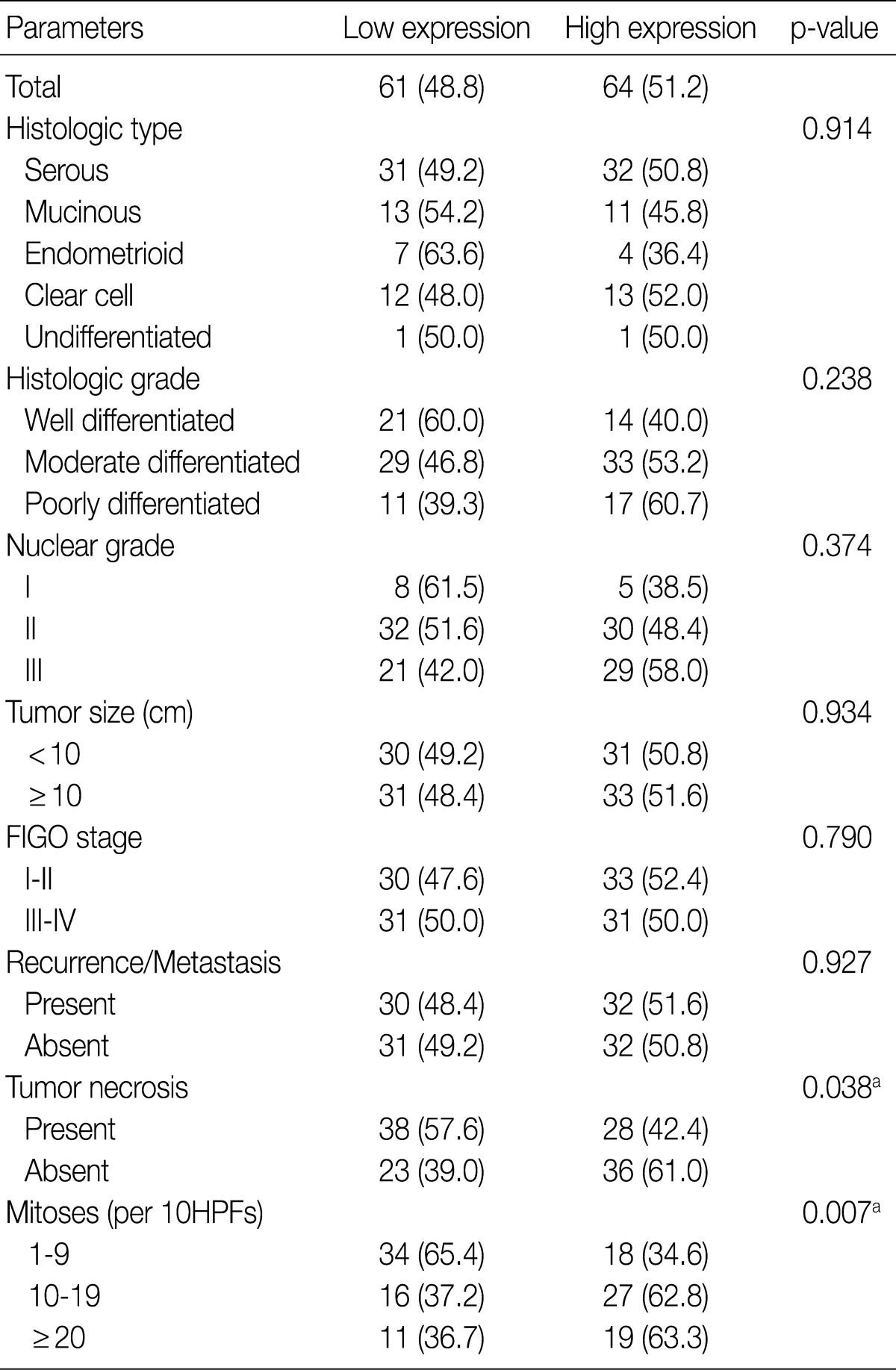
Values are presented as number (%). Low expression, less than 10% positive staining of tumor cells; high expression, more than 10% positive staining of tumor cells. GLUT-1, glucose transporter-1; FIGO, Federation of Gynecology and Obstetrics; HPF, high power field. aStatistically significance (Pearson's chi-squared test).
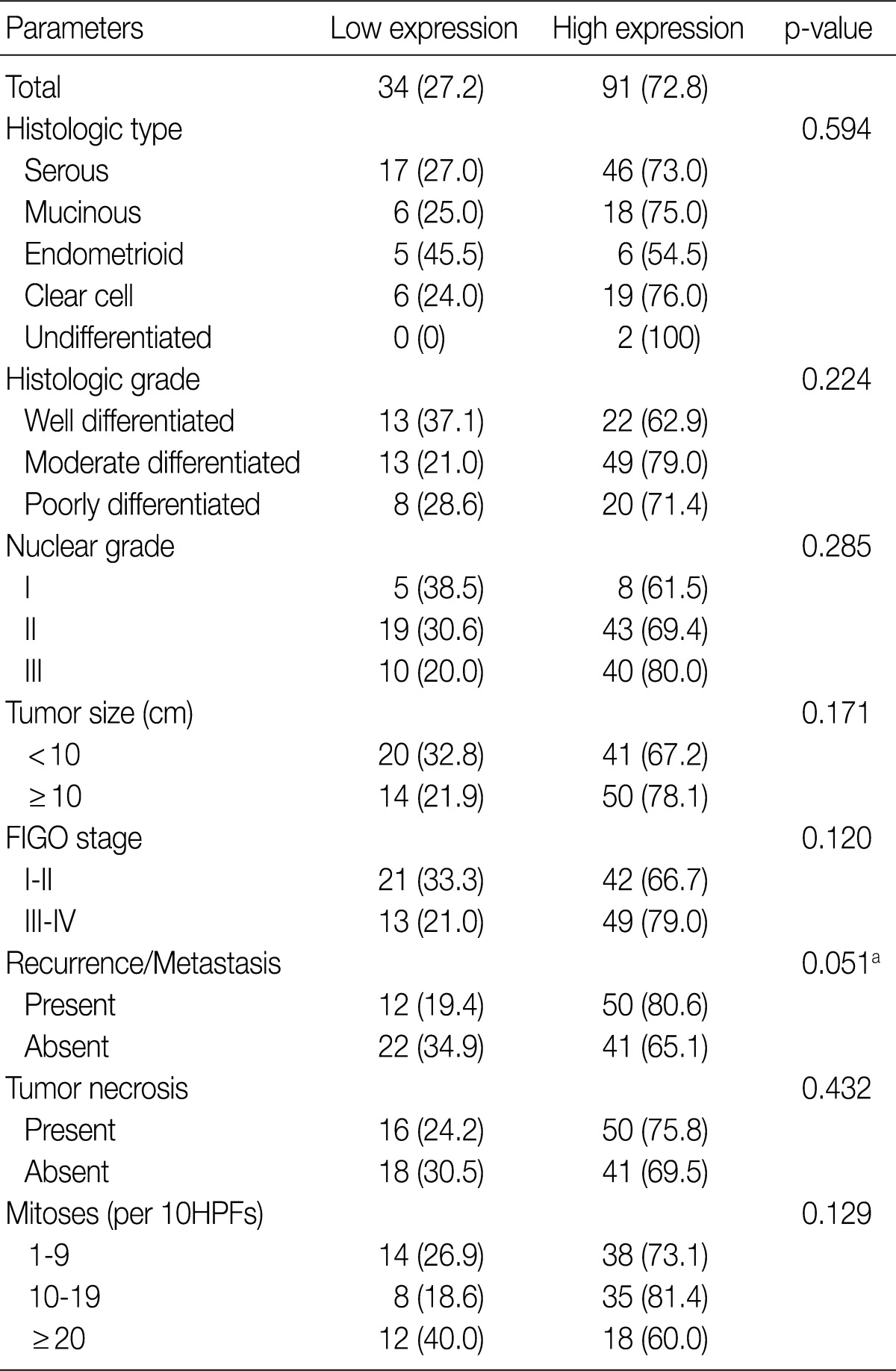
Low expression, less than 10% positive staining of tumor cells; high expression, more than 10% positive staining of tumor cells. VEGF, vascular endothelial growth factor; FIGO, Federation of Gynecology and Obstetrics; HPF, high power field. aStatistically significance (Pearson's chi-squared test).

