 E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 47(6); 2013 > Article
-
Case Study
Cytomorphological Findings and Histological Correlation of Low-Grade Cribriform Cystadenocarcinoma of Salivary Gland in Fine-Needle Aspiration: A Case Study - Young Sin Ko, Ja Seung Koo
-
Korean Journal of Pathology 2013;47(6):592-595.
DOI: https://doi.org/10.4132/KoreanJPathol.2013.47.6.592
Published online: December 24, 2013
Department of Pathology, Yonsei University College of Medicine, Seoul, Korea.
- Corresponding Author: Ja Seung Koo, M.D. Department of Pathology, Yonsei University College of Medicine, 50 Yonsei-ro, Seodaemun-gu, Seoul 120-752, Korea. Tel: +82-2-2228-1772, Fax: +82-2-362-0860, kjs1976@yuhs.ac
• Received: November 20, 2012 • Revised: January 8, 2013 • Accepted: January 25, 2013
© 2013 The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
- Low-grade cribriform cystadenocarcinoma (LGCCC) of the salivary gland is a rare tumor. We report the cytologic features and histologic correlation of a patient with LGCCC. A 57-year-old man had a hardly palpable, nontender mass in the right cheek area followed over nine months. Radiologic analysis revealed a 1.2 cm multiseptated, cystic, solid nodule in an anterior superficial lobe of the right parotid gland. Fine-needle aspiration cytology revealed many irregular overlapping sheets or clusters of ductal epithelial cells forming solid, pseudopapillary, and cribriform architectures. Nuclei of the tumor cells revealed inconspicuous atypia with minimal size variation. On the basis of these findings, we confirmed a diagnosis of ductal epithelial proliferative lesion, favoring neoplasm, with uncertain malignant potential. Tumor excision was performed, revealing a tiny multicystic nodule (0.7 cm). Histopathologically, this tumor showed the characteristic morphology of LGCCC. This is the first report of cytomorphological findings of LGCCC in Korea.
- Brief patient history
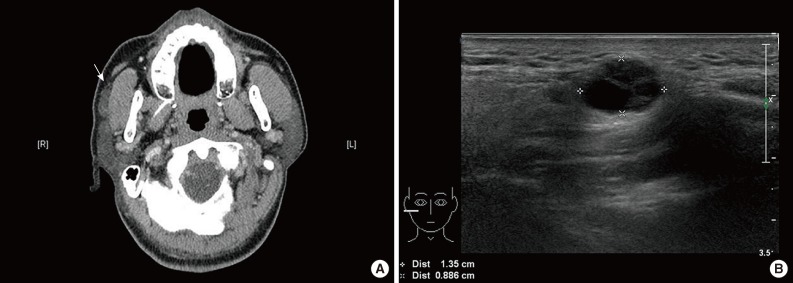
- A 57-year-old man had a barely palpable, nontender mass in the right cheek area, followed up over a nine-month period. Contrast-enhanced computed tomography revealed a mildly enhancing mass in an anterior superficial lobe of the right parotid gland (Fig. 1A). On ultrasonography, the lesion appeared as an approximately 1.2 cm large, multiseptated, cystic, solid nodule (Fig. 1B). FNA was performed and the cytologic examination led to a diagnosis of ductal epithelial proliferative lesion, favoring neoplasm, of uncertain malignant potential. Histologic confirmation was required.
- Pathologic diagnosis
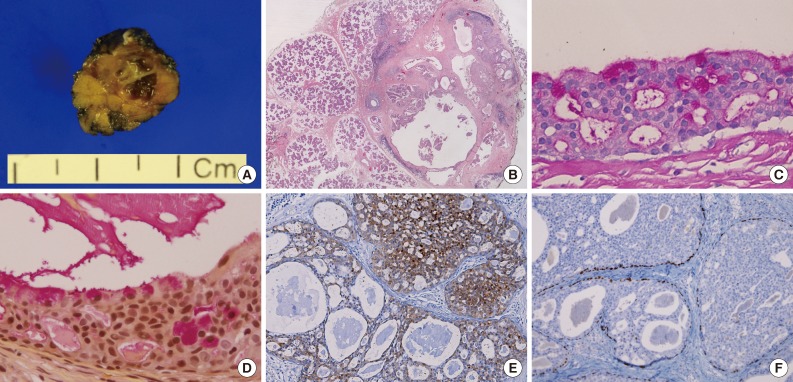
- Excision of the lesion from the right parotid gland was performed. The surgical specimen revealed a tiny multicystic nodule (0.7 cm), which appeared to be surrounded by normal salivary gland tissue. The cut surface of the tumor was partly solid and partly cystic (Fig. 2A). Microscopically, it was a salivary ductal epithelial neoplasm showing multiple cysts lined by relatively bland ductal cells and a partly solid proliferation of ductal cells (Fig. 2B). Many of the superficial lining cells contained cytoplasmic apocrine-type microvacuoles that were periodic acid-Schiff-positive/diastase-resistant (Fig. 2C) and mucicarmine-positive (Fig. 2D). The tumor cells were strongly and diffusely S-100 protein positive (Fig. 2E). Myoepithelial markers (including actin and p63) highlighted the presence of cells surrounding the cystic spaces, confirming the intraductal nature of the lesion (Fig. 2F). No invasive foci were noted. On the basis of these findings, we diagnosed the mass as a low grade cribriform cystadenocarcinoma, marginally excised.
- Cytomorphological findings and histological correlation
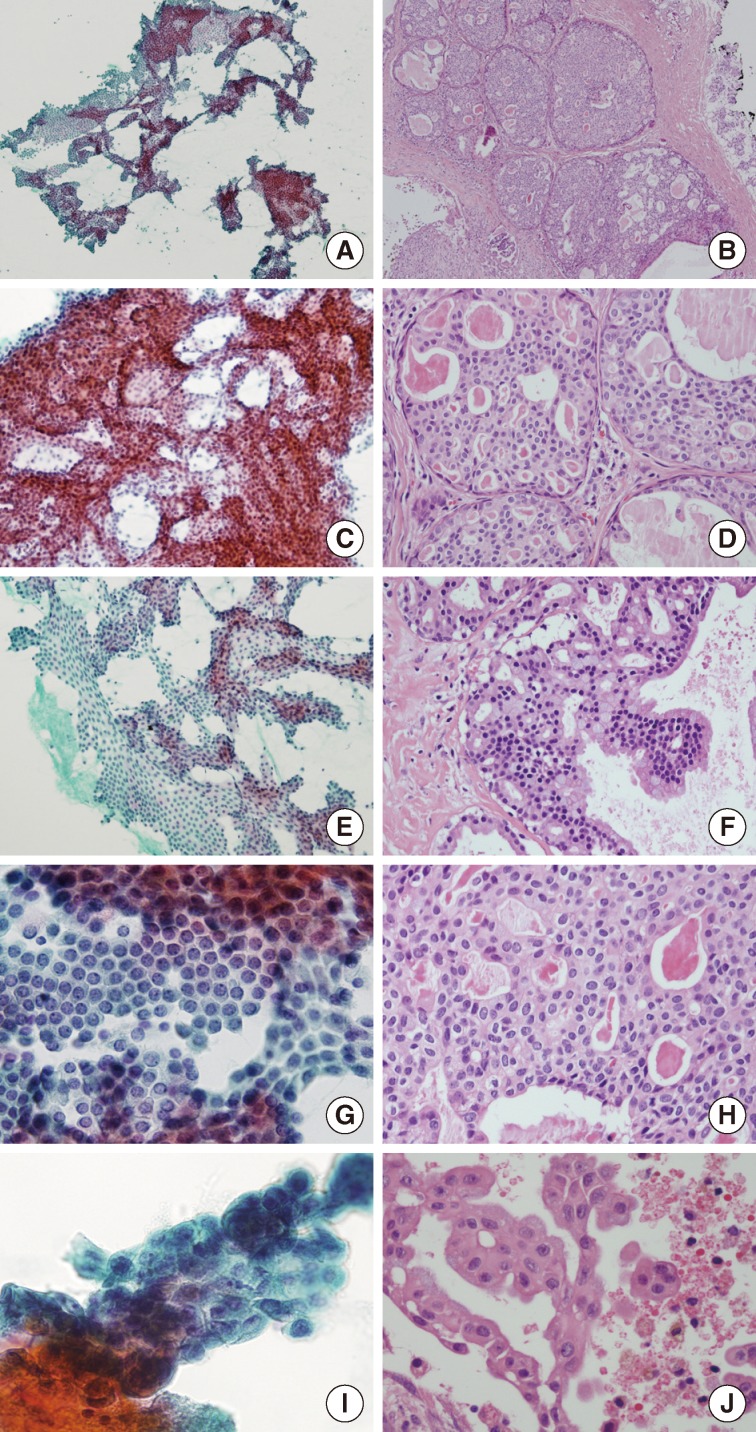
- The cellular smear showed many large sheets or clusters of ductal epithelial cells in an irregular overlapping arrangement (Fig. 3A). These cytologic components could be aspirated from the solid area of this tumor (Fig. 3B). Architecturally, the tumor cells had tight intercellular connections forming a vague cribriform (Fig. 3C), solid, or pseudopapillary (Fig. 3E) arrangement. These were matched with histologic findings. The solid areas revealed a cribriform pattern, resembling ADH and low-grade ductal carcinoma in situ of the breast (Fig. 3D). The pseudopapillary projections were found in the epithelial lining the cystic areas (Fig. 3F). Cytologically, almost all tumor cells were bland looking, ductal epithelial cells with low nuclear/cytoplasmic (N/C) ratio. The nucleoli were found to be small, single, or entirely absent. Nuclear chromatin was fine or slightly coarse (Fig. 3G, H). Squamoid or metaplastic changes of the tumor cells, mentioned by Nakazawa et al.,9 were also identified in this case. Nuclear atypia was inconspicuous; however, one focus showed mild atypia with minimal nuclear size variation, prominent nucleoli, and vacuolated cytoplasm (Fig. 3I, J). The background was relatively clear in the cystic space. Scattered inflammatory cells with hemosiderin-laden macrophages, neutrophils, and eosinophils were seen. No evidence of necrosis or mucin was found.
- Postoperative outcome
- Whole-body positron emission tomography-computed tomography scanning was conducted after surgery. A residual, enhancing nodular lesion in the anteriosuperior aspect of the right parotid gland showed mild, increased fluorodeoxyglucose uptake. Overall, residual malignancy was suggested. Postoperative chemotherapy or radiation therapy was not recommended. A follow-up was conducted two months later. At that time, the patient was healthy, with no evidence of recurrence or distant metastasis.
CASE REPORT
- This is the first report of the cytomorphological findings of LGCCC in Korea and the second report in the English literature. Compared with the first case, described by Nakazawa et al.,9 the two cases share common cytomorphology summarized as follows: 1) irregular and overlapping sheets or clusters of ductal epithelial proliferation with tight connections; 2) mild nuclear atypia with low N/C ratio, slightly coarse chromatin, inconspicuous or one small nucleolus and minimal size variation; 3) cytoplasmic vacuoles and squamoid or metaplastic changes of tumor cells; and 4) a cystic or inflammatory background with mixed inflammatory cells and hemosiderin-laden macrophages with no evidence of necrosis or mucin. Further, we report the following new findings that were not reported by Nakazawa et al.9: 1) tumor cells with solid, pseudopapillary, or cribriform architectural arrangement; 2) absence of "large yellow to brown pigments" in the cytoplasm of the tumor cells; 3) the smear in our case showed more benign-looking cytomorphology, with almost all tumor cells presenting inconspicuous cytologic atypia, resembling instead benign, ductal proliferating cells. Only a few clusters of tumor cells revealed minimal cytologic atypia.
- Nakazawa et al.9 presented salivary duct carcinoma, papillary cystic variant of acinar cell carcinoma, and mucoepidermoid carcinoma as the results of differential diagnoses. However, in this case, we would consider benign salivary gland adenoma as the differential diagnosis since almost all tumor cells showed benign-looking cytomorphology. However, this diagnosis can be ruled out by the small clusters of mild cytologic atypia, as previously described. Adenoid cystic carcinoma (ACC) might be considered a differential diagnosis due to similar architecture at low magnification; however, the cribriform architecture of LGCCC is different from ACC. It can be described as "less defined" or "more vague" than ACC because basaloid cells were not identified in the cribriform area. Typical hyaline globules were also not seen in our case. Finally, the cytologic atypia observed in this case was too mild. High-grade tumors can also be ruled out as a diagnosis because the observed atypia was not severe or marked; rather, it was very minimal or mild.
- In conclusion, when pathologists are presented with an aspiration cytology of salivary gland tumors, an effort must be made to discover any small foci showing minimal atypism; otherwise, there is potential to overlook the possibility of a low-grade malignancy such as LGCCC. We recommend more intensive investigation of FNA specimens.
- This report is important as it is the second case report in the English literature on the cytologic features of LGCCC in FNA. Herein, we also described histologic correlations, which provide new observations, and the absence of previously reported features. Furthermore, we hope to encourage more authors to report cytomorphologic features of LGCCC in salivary gland in order to gather diagnostic criteria in FNA of this tumor. Until then, when LGCCC is suspected in FNA cytology, an improved descriptive diagnosis will facilitate the differential diagnosis and the recommendation of surgical excision, which would be preferred over a report limited only to a specific diagnosis.
DISCUSSION
- 1. Brandwein-Gensler MS, Gnepp DR. Low-grade cribriform cystadenocarcinoma. In: Barnes L, Evenson JW, Reichart P, eds. Sidransky. World Health Organization classification of tumours: pathology and genetics head and neck tumours. Lyon: IARC Press, 2005; 233.
- 2. Delgado R, Klimstra D, Albores-Saavedra J. Low grade salivary duct carcinoma: a distinctive variant with a low grade histology and a predominant intraductal growth pattern. Cancer 1996; 78: 958-967. ArticlePubMed
- 3. Brandwein-Gensler M, Hille J, Wang BY, et al. Low-grade salivary duct carcinoma: description of 16 cases. Am J Surg Pathol 2004; 28: 1040-1044. PubMed
- 4. Simpson RH, Desai S, Di Palma S. Salivary duct carcinoma in situ of the parotid gland. Histopathology 2008; 53: 416-425. ArticlePubMed
- 5. Arai A, Taki M, Mimaki S, Ueda M, Hori S. Low-grade cribriform cystadenocarcinoma of the parotid gland: a case report. Auris Nasus Larynx 2009; 36: 725-728. ArticlePubMed
- 6. Laco J, Podhola M, Dolezalova H. Low-grade cribriform cystadenocarcinoma of the parotid gland: a neoplasm with favorable prognosis, distinct from salivary duct carcinoma. Int J Surg Pathol 2010; 18: 369-373. ArticlePubMedPDF
- 7. Weinreb I. Intraductal carcinoma of salivary gland (so-called low-grade cribriform cystadenocarcinoma) arising in an intraparotid lymph node. Head Neck Pathol 2011; 5: 321-325. ArticlePubMedPMCPDF
- 8. Nakatsuka S, Harada H, Fujiyama H, et al. An invasive adenocarcinoma of the accessory parotid gland: a rare example developing from a low-grade cribriform cystadenocarcinoma? Diagn Pathol 2011; 6: 122.ArticlePubMedPMCPDF
- 9. Nakazawa T, Kondo T, Yuminomochi T, et al. Fine-needle aspiration biopsy of low-grade cribriform cystadenocarcinoma of the salivary gland. Diagn Cytopathol 2011; 39: 218-222. ArticlePubMed
REFERENCES
Fig. 1Radiologic findings. Enhanced computed tomography reveals a mildly enhanced mass (arrow) in the anterior superficial lobe of the right parotid gland. (A) It is separated from the main parotid gland and could be an accessory parotid gland tumor or lymphadenopathy. (B) On ultrasonography, an approximately 1.2-cm large, cystic, solid nodule is noted in the right cheek area.
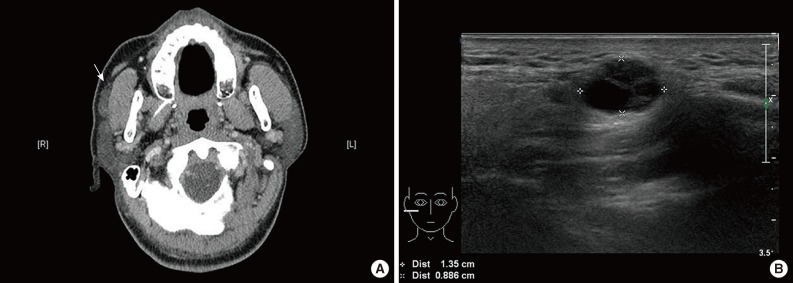
Fig. 2Gross findings and histopathology. (A) Gross findings reveal a tiny multicystic nodule (0.7 cm). (B) Microscopically, the tumor consists of multiple cysts with partly solid ductal epithelial proliferation. Many superficial cells contain cytoplasmic apocrine-type microvacuoles that are periodic acid-Schiff-positive/diastase-resistant (C) and mucicarmine-positive (D). (E) S-100 protein is diffusely expressed in the tumor cells. (F) p63 immunostaining demonstrates the presence of myoepithelial cells and absence of p63 in the intraductal proliferating tumor cells.
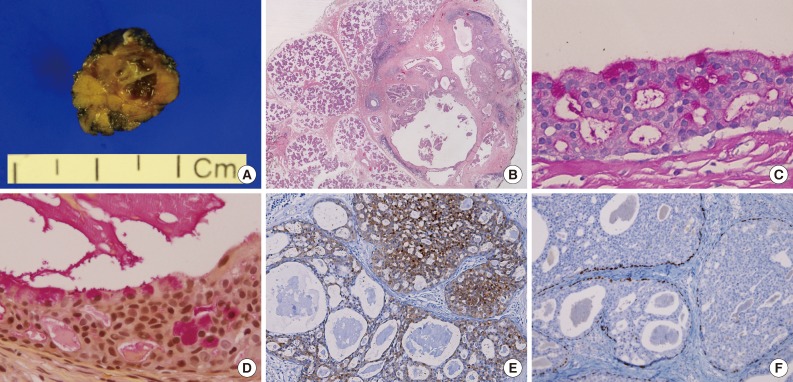
Fig. 3Cytomorphological findings and histological correlation. Papanicolaou staining of a smear reveals many sheets and clusters of ductal epithelial cells with irregular overlapping (A) which might be aspirated from solid areas of the tumor (B). Tight intercellular connections with vague cribriform arrangement (C), correlates with the histologic component of the solid area resembling atypical ductal hyperplasia and low-grade ductal carcinoma in situ of the breast (D). (E, F) The pseudopapillary architecture may be a micropapillary projection of the lining epithelium of cystic area. (G, H) Almost all tumor cells are bland-looking with low nuclear/cytoplasmic ratios, with inconspicuous or one small nucleolus and relatively fine nuclear chromatin. (I, J) Only small foci of tumor cells have mild cytologic atypia with minimal size variation and prominent nucleoli.
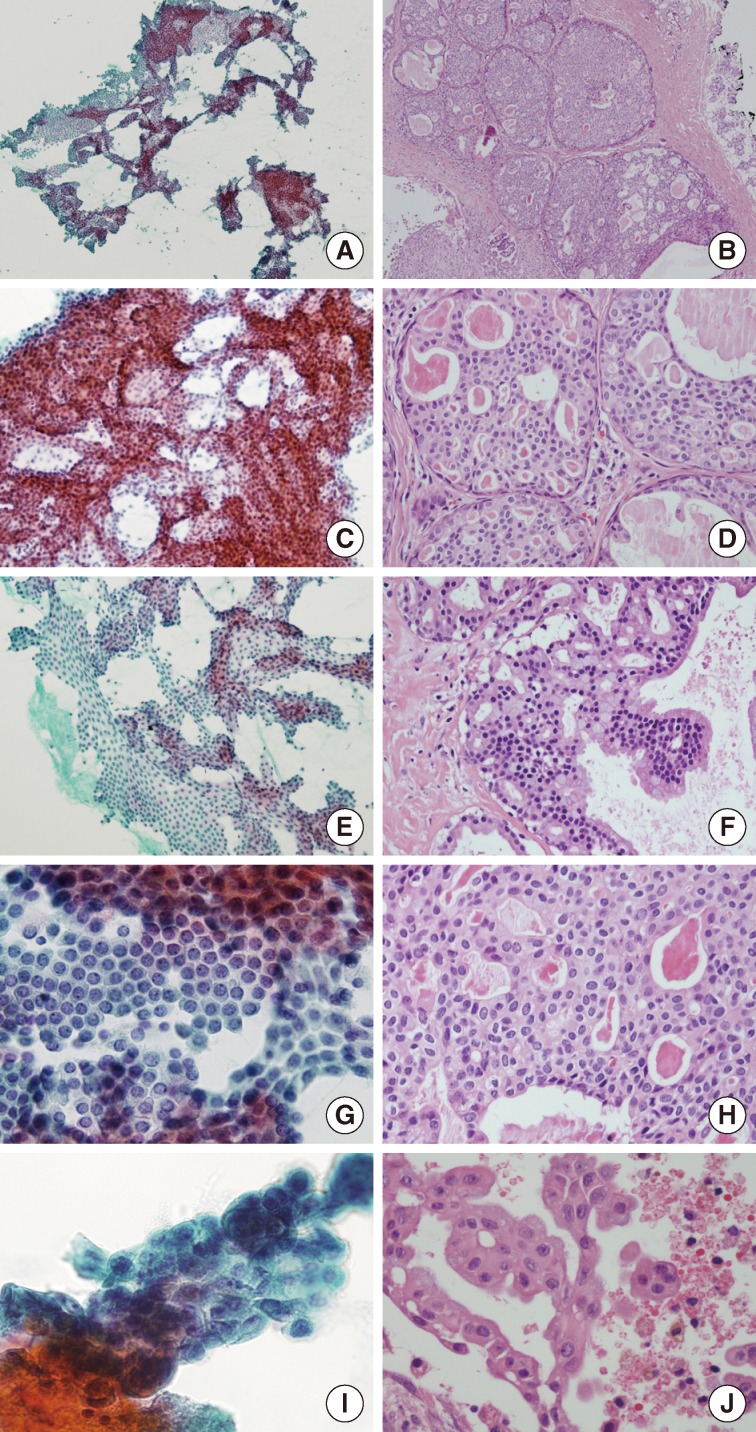
Figure & Data
References
Citations
Citations to this article as recorded by 
- Duct tales of a parotid gland swelling
Swati Raj, Monika Singh, Mamta Gupta, Naveen Thapliyal
Cytojournal.2023; 20: 22. CrossRef - Salivary Gland Intraductal Carcinoma: How Do 183 Reported Cases Fit Into a Developing Classification
Lester D.R. Thompson, Justin A. Bishop
Advances in Anatomic Pathology.2023; 30(2): 112. CrossRef - Intraductal carcinoma of the parotid gland
Yukiya HIRATA, Kayoko HIGUCHI, Toshitaka NAGAO, Yoko ZUKERAN, Takao KINJO, Naoki WADA
The Journal of the Japanese Society of Clinical Cytology.2022; 61(6): 431. CrossRef - Intraductal carcinomas of the salivary glands: systematic review and classification of 93 published cases
Andrea Palicelli
APMIS.2020; 128(3): 191. CrossRef - What do we know about the cytological features of pure intraductal carcinomas of the salivary glands?
Andrea Palicelli
Cytopathology.2020; 31(3): 185. CrossRef - Diagnosing Recently Defined and Uncommon Salivary Gland Lesions in Limited Cellularity Specimens: Cytomorphology and Ancillary Studies
Esther Diana Rossi, Zubair Baloch, William Faquin, Liron Pantanowitz
AJSP: Reviews and Reports.2020; 25(5): 210. CrossRef - Low-grade intraductal carcinoma of salivary glands: A systematic review of this rare entity
Francesco Giovacchini, Caterina Bensi, Stefano Belli, Maria Elena Laurenti, Martina Mandarano, Daniele Paradiso, Michele Giansanti, Antonio Tullio
Journal of Oral Biology and Craniofacial Research.2019; 9(1): 96. CrossRef - The rare entity of cystadenocarcinoma (CAC) in parotid gland: A single-center experience
Bing Guo, Yu-an Cao, Xingjun Qin, Chunyue Ma
Journal of Cranio-Maxillofacial Surgery.2019; 47(5): 826. CrossRef - Cytopathology approach to rare salivary gland lesions with oncocytic features
Siba El Hussein, Samer N. Khader
Diagnostic Cytopathology.2019; 47(10): 1090. CrossRef - Unicystic high‐grade intraductal carcinoma of the parotid gland: cytological and histological description with clinic–pathologic review of the literature
Andrea Palicelli, Paola Barbieri, Narciso Mariani, Paola Re, Stefania Galla, Raffaele Sorrentino, Francesca Locatelli, Nunzio Salfi, Guido Valente
APMIS.2018; 126(9): 771. CrossRef - Low-grade cribriform cystadenocarcinoma arising from a minor salivary gland: a case report
Masashi Kimura, Shinji Mii, Shinichi Sugimoto, Kosuke Saida, Shojiroh Morinaga, Masahiro Umemura
Journal of Oral Science.2016; 58(1): 145. CrossRef - A Case of Cystadenocarcinoma Arising from Parotid Gland
Jong Chul Hong, Tae Kyoung Koh, Min Gyoung Pak, Heon Soo Park
Korean Journal of Otorhinolaryngology-Head and Neck Surgery.2016; 59(4): 300. CrossRef - Mammary analogue secretory carcinoma of parotid gland
Atsuko NASU, Sakae HATA, Masaru FUJITA, Toyoko YAMAUCHI, Satoko NAKAMURA, Takehiro TANAKA, Kouichi ICHIMURA, Hiroyuki YANAI
The Journal of the Japanese Society of Clinical Cytology.2016; 55(2): 112. CrossRef
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-
Cytomorphological Findings and Histological Correlation of Low-Grade Cribriform Cystadenocarcinoma of Salivary Gland in Fine-Needle Aspiration: A Case Study



Fig. 1 Radiologic findings. Enhanced computed tomography reveals a mildly enhanced mass (arrow) in the anterior superficial lobe of the right parotid gland. (A) It is separated from the main parotid gland and could be an accessory parotid gland tumor or lymphadenopathy. (B) On ultrasonography, an approximately 1.2-cm large, cystic, solid nodule is noted in the right cheek area.
Fig. 2 Gross findings and histopathology. (A) Gross findings reveal a tiny multicystic nodule (0.7 cm). (B) Microscopically, the tumor consists of multiple cysts with partly solid ductal epithelial proliferation. Many superficial cells contain cytoplasmic apocrine-type microvacuoles that are periodic acid-Schiff-positive/diastase-resistant (C) and mucicarmine-positive (D). (E) S-100 protein is diffusely expressed in the tumor cells. (F) p63 immunostaining demonstrates the presence of myoepithelial cells and absence of p63 in the intraductal proliferating tumor cells.
Fig. 3 Cytomorphological findings and histological correlation. Papanicolaou staining of a smear reveals many sheets and clusters of ductal epithelial cells with irregular overlapping (A) which might be aspirated from solid areas of the tumor (B). Tight intercellular connections with vague cribriform arrangement (C), correlates with the histologic component of the solid area resembling atypical ductal hyperplasia and low-grade ductal carcinoma in situ of the breast (D). (E, F) The pseudopapillary architecture may be a micropapillary projection of the lining epithelium of cystic area. (G, H) Almost all tumor cells are bland-looking with low nuclear/cytoplasmic ratios, with inconspicuous or one small nucleolus and relatively fine nuclear chromatin. (I, J) Only small foci of tumor cells have mild cytologic atypia with minimal size variation and prominent nucleoli.
Fig. 1
Fig. 2
Fig. 3
Cytomorphological Findings and Histological Correlation of Low-Grade Cribriform Cystadenocarcinoma of Salivary Gland in Fine-Needle Aspiration: A Case Study

