 E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 48(1); 2014 > Article
-
Original Article
Usual Interstitial Pneumonia with Lung Cancer: Clinicopathological Analysis of 43 Cases - Dae Hyun Song, In Ho Choi, Sang Yun Ha, Kang Min Han, Jae Jun Lee, Min Eui Hong, Kyeongman Jeon1, Man Pyo Chung1, Jhingook Kim2, Joungho Han
-
Korean Journal of Pathology 2014;48(1):10-16.
DOI: https://doi.org/10.4132/KoreanJPathol.2014.48.1.10
Published online: February 25, 2014
Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
1Department of Internal Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
2Department of Thoracic Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- Corresponding Author: Joungho Han, M.D. Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, 81 Irwon-ro, Gangnam-gu, Seoul 135-710, Korea. Tel: +82-2-3410-2800, Fax: +82-2-3410-0025, hanjho@skku.edu
© 2014 The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Background
- Previous studies have suggested an association between usual interstitial pneumonia (UIP) and lung cancer (Ca). However, clinical and histological information is not enough to determine such an association, due to the low incidence and short survival time of patients with both conditions.
-
Methods
- We retrospectively reviewed the clinical and histological records of Ca patients with UIP between January 1999 and August 2013 at the Samsung Medical Center, Seoul, Korea. We found 43 patients who had Ca with UIP (UIP-Ca). Previously reported data of eighty-four patients with UIP-only were included as a comparison group.
-
Results
- Smoking is related to poor prognosis in patients with UIP-Ca, and the number of patients with a high smoking index of more than 30 pack-years significantly increased in UIP-Ca patients compared with UIP-only patients. There is no significant prognostic differentiation between UIP-Ca patients and UIP-only patients. Microscopically, UIP-Ca patients showed characteristically heterogeneous histological patterns and degrees of differentiation. There were many foci of squamous metaplasia or dysplasia at the peripheral area of squamous cell carcinomas.
-
Conclusions
- We report 43 cases of UIP-Ca. Our results suggest that smoking is related to cancer occurrence in UIP patients and poor prognosis in UIP-Ca patients.
- Case selection
- We collected data from lung cancer patients with UIP between January 1999 and August 2013 from the Samsung Medical Center, Seoul, Korea. A total of 46 patients were detected. These patients showed clinically appropriate operability and resectability, and pneumonectomy, lobectomy, sleeve lobectomy or wedge resection was performed. Three patients with connective tissue disease, including one patient with systemic sclerosis, one patient with CREST syndrome, and one patient with Sjogren syndrome, which are known risk factors for interstitial lung disease, were excluded. The remaining 43 patients had no drug or occupational history. Preoperative computed tomographies were examined. Gross findings, hematoxylin and eosin and immunohistochemical slides of surgical specimens were reviewed by two pathologists. Simultaneous diagnosis of lung cancer and UIP was found in twenty of the 43 patients (47%) (Tables 1, 2). The remainder showed the diagnostic time of precedent UIP and subsequent lung cancer. The cancer-free period (CFP) is defined as the period of UIP before the detection of lung cancer (e.g., a CFP of zero means UIP and lung cancer were diagnosed at the same time).
- Microscopically, all cases showed lung cancers at the background of UIP. The Institutional Review Board approved this study (SMC 2013-08-149-001).
- Reference data as comparison group
- Clinical data of eighty-four patients with UIP without lung cancer from a previous report was included for comparison (Table 3).7 These 84 patients were diagnosed at our hospital between July 1996 and June 2002. Fifty-seven of the 84 patients were histologically diagnosed by surgical lung biopsy and the remaining twenty-seven patients were identified by the nonhistological diagnostic criteria of the American Thoracic Society.8 Identical exclusion criteria were used for reference group selection.
- Statistical analysis
- The overall survival of patients with lung cancer and UIP and patients in the reference group was compared using the multivariate analysis of the Cox proportional hazard model. Correlation analysis was performed using chi-squared tests and independent t-tests. Values were considered statistically significant at a p-value less than .05. All statistical analyses were performed in SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA).
MATERIALS AND METHODS
- Of the 43 patients, 41 (95%) were male and 34 (79%) were smokers. The smokers included 14 current and 20 ex-smokers. The mean age was 68 years. Thirty-seven (86%) patients received a lobectomy, and 33 (77%) instances of lung cancer were located in the lower lobe. The lung cancers consisted of 18 squamous cell carcinomas, 17 adenocarcinomas, 2 combined carcinomas, 2 large cell neuroendocrine carcinomas, and a number of other less common neoplasms. The combined carcinomas consisted of squamous cell carcinoma with a large cell neuroendocrine carcinoma, and small cell carcinoma with a non-small cell carcinoma.
- Compared to the reference data, older age and male sex were significantly associated with lung cancer in patients with UIP (Table 4). In addition, positive smoking history and more than 30 pack-years of smoking (mean cigarette number per day multiplied by smoking years) were higher in the UIP with lung cancer group than in the UIP-only group (Table 4).
- Survival analysis results revealed a 1-year survival rate of 60% for patients with lung cancer and UIP. Multivariate analysis of the Cox proportional hazard model was performed with factors of age, stage, surgical procedure, smoking history, smoking index and pulmonary function test before surgery in the 43 UIP with lung cancer patients and in the total 127 patients, including the 84 UIP-only patients (Tables 5, 6). Except for smoking history, all factors showed no significant correlation with survival. In the 43 UIP with lung cancer patients, those with smoking history had an odds ratio of 12.610 (95% confidence interval [CI], 1.293 to 123.016; p=.029) relative to the nonsmoking patients. In the group of all 127 patients, the patients with smoking history had an odds ratio of 1.557 (95% CI, 0.799 to 3.033; p=.193) relative to the nonsmoking patients. In addition, an odds ratio of 0.461 was found between the UIP with cancer and the UIP-only patients.
- The causes of death were examined. Metastasis of lung cancer occurred to the spine in one patient, to the pleura in one patient and to the lung in the other 5 patients. Thirteen patients died due to pulmonary failure with pneumonia. Acute respiratory distress syndrome and acute renal failure occurred in three patients with a survival period of less than 1 month. The remaining 23 patients were censored or had no clinical record.
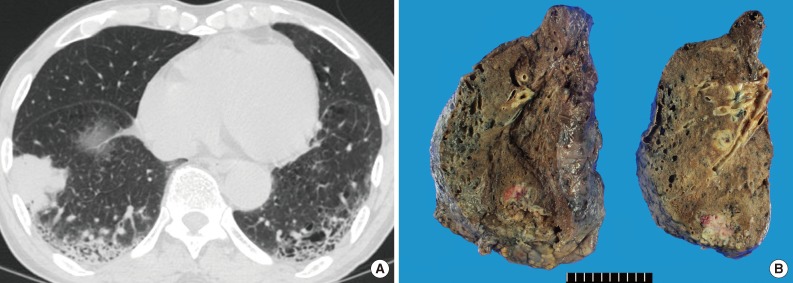
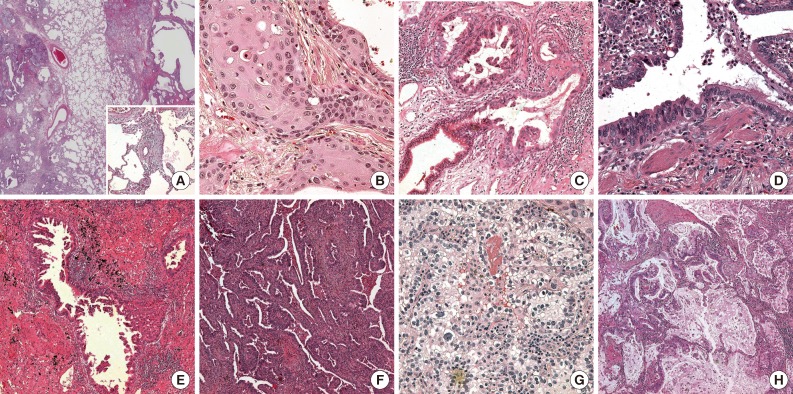
- Histopathologically, on gross examination, all tumors were located at the UIP lesion. Almost all tumors were poorly circumscribed and were 0.4 to 7.5 cm in size. The UIP lesion was found to be firm and poorly circumscribed in appearance with a honeycombing pattern. Microscopically, UIP was detected in the peritumoral area in all cases. The UIP showed nonuniform interstitial fibrosis with a patchwork pattern, fibroblastic foci, mild inflammation and honeycomb changes (Figs. 1, 2A). Several areas with hyperplasia of bronchial smooth muscle were detected. There were frequent areas of brown pigmented macrophages in the air spaces and interstitia.
- Squamous cell carcinoma with UIP
- Eighteen of the 43 lung cancers were squamous cell carcinomas. Twelve cases were moderately differentiated, 5 cases were poorly differentiated and 1 case was well differentiated. The patient with a well-differentiated squamous cell carcinoma (case no. 43) had a comparatively longer survival period. Microscopically, the structure of UIP was maintained in the tumoral areas, and cancer cell proliferation was observed along the cavernous hall of the honeycombing. The tumors showed variable degrees of differentiation. Wide dense fibrotic stroma was detected between the clusters of the squamous cell carcinomas. Peritumoral UIP lesions occasionally showed squamous metaplasia or dysplastic epithelial cells (Fig. 2). The foci of squamous metaplasia were haphazardly distributed along the cavernous hall of honeycombing.
- Adenocarcinoma with UIP
- Seventeen of the 43 lung cancers were adenocarcinomas. Microscopically, dense fibrotic stroma and large cavities of honeycombing were discovered in the tumoral areas. The adenocarcinomas also grew along the cavernous halls of honeycombing rather than invading the fibrotic stroma. The growth patterns varied at tumors and were described as acinar, papillary, micropapillary or solid with cavitation.9,10 The acinar pattern with branching was the most frequently observed (Fig. 2F), followed by papillary and micropapillary patterns (Fig. 2E). One case showed a mainly solid pattern. Most of the adenocarcinomas accompanied clear cell changes (Fig. 2G). Clear cells had distinct cell borders that had plump clear to pinkish cytoplasm and round nuclei with smooth and slightly thickened membranes. Several areas of intracellular or extracellular mucin production (Fig. 2H) were detected. In addition, there were many foci of transformation from normal bronchiolar epithelium to adenocarcinomas in the peripheral tumor areas (Fig. 2C, D).
RESULTS
- UIP is a fatal interstitial fibrosing disease of the lung. In recent studies, a similarity between UIP and lung cancer has been suggested based on epigenetic and genetic abnormalities, pathogenetic sequence, a shared feature of uncontrolled proliferation and abnormalities of specific signaling pathways in UIP.11,12 UIP is also known to increase the risk of lung cancer.6 Although there are only a few reports regarding lung cancer in patients with UIP, they commonly describe a predominance of squamous cell carcinoma, male sex and a positive history of smoking.5 Our study also showed a significantly higher incidence in older or male patients compared to a reference group. UIP patients with lung cancer showed higher rates of smoking history (p=.113) and more than 30 pack-years of smoking (p=.052). According to several previous reports,5,6,13 smoking ought to be related to UIP with lung cancer. Our study also shows such a relationship. We also found many foci of squamous metaplasia at the periphery of squamous cell carcinomas. Considering the well-known relationship between smoking and squamous metaplasia, we suggest smoking as a pathogen of lung cancer in UIP patients. Calabrese et al.14 described the overexpression of squamous cell carcinoma antigens in IPF. They demonstrated that metaplastic epithelial cells play an important role in the tumorigenesis of UIP. There were many foci of squamous metaplasia in honeycombing epithelium in the present study. According to a report of Hironaka and Fukuyama,15 IPF patients with lung cancer showed more frequent foci of squamous metaplasia than IPF patients without lung cancer (p=.002). They suggested that squamous metaplasia may not be a precursor of lung cancer itself, but could cause a susceptibility to developing lung carcinoma on the basis of Ki67 and p53 indexes. As a result, smoking may promote tumorigenesis, and metaplastic and dysplastic foci of the UIP lesion suggest progression to lung cancer. We recommend that the amount of metaplastic or dysplastic foci be mentioned in the pathologic report of lung biopsies, and that UIP patients who have frequently metaplastic foci and more than 30 pack-years of smoking receive close follow-up.
- Histologically, the major lung neoplasms identified in patients with UIP were squamous cell carcinoma and adenocarcinoma. These lesions showed a characteristically variable degree of differentiation and histological pattern. These disparate findings may be explained by two broad hypotheses regarding pathogenesis. 1) UIP background: UIP has heterogeneous microscopic features that lead to heterogeneous structural patterns and a variable degree of differentiation. 2) Synchronous dysplastic foci: many metaplastic and dysplastic foci were found in peritumoral UIP lesions. A neoplastic mass may be composed of several synchronous tumors originating from a single UIP lesion. This hypothesis of conjoined synchronous tumors can explain the variable degree of differentiation and structural patterns, as well as the incidence of combined tumors and tumors that are found soon after or at the same time patients are diagnosed with UIP.
- In the survival analysis, the odds ratio between the cancer group and the no cancer group was 0.461. This indicates that there is no significant prognostic differentiation between the UIP with lung cancer group and the UIP-only group. Even though this study has a limitation of the previously reported comparison group, such a low value of the odds ratio has implications for clinical prognostic guidelines and Korean data.
- In conclusion, we report a rare 43 cases of UIP with lung cancer. Smoking is related to poor prognosis in UIP patients with lung cancer, and the number of patients with high a smoking index of more than 30 pack-years significantly increased in UIP with lung cancer patients compared with UIP-only patients. There is no significant prognostic differentiation between UIP with lung cancer patients and UIP-only patients in multivariate analysis.
DISCUSSION
- 1. Katzenstein AL, Myers JL. Nonspecific interstitial pneumonia and the other idiopathic interstitial pneumonias: classification and diagnostic criteria. Am J Surg Pathol 2000; 24: 1-3. ArticlePubMed
- 2. American Thoracic Society. European Respiratory Society. American Thoracic Society/European Respiratory Society International Multidisciplinary Consensus Classification of the Idiopathic Interstitial Pneumonias. This joint statement of the American Thoracic Society (ATS), and the European Respiratory Society (ERS) was adopted by the ATS board of directors, June 2001 and by the ERS Executive Committee, June 2001. Am J Respir Crit Care Med 2002; 165: 277-304. ArticlePubMed
- 3. Plones T, Osei-Agyemang T, Elze M, et al. Morbidity and mortality in patients with usual interstitial pneumonia (UIP) pattern undergoing surgery for lung biopsy. Respir Med 2013; 107: 629-632. ArticlePubMed
- 4. Poletti V, Ravaglia C, Buccioli M, et al. Idiopathic pulmonary fibrosis: diagnosis and prognostic evaluation. Respiration 2013; 86: 5-12. ArticlePubMedPDF
- 5. Archontogeorgis K, Steiropoulos P, Tzouvelekis A, Nena E, Bouros D. Lung cancer and interstitial lung diseases: a systematic review. Pulm Med 2012; 2012: 315918.ArticlePubMedPMCPDF
- 6. Park J, Kim DS, Shim TS, et al. Lung cancer in patients with idiopathic pulmonary fibrosis. Eur Respir J 2001; 17: 1216-1219. ArticlePubMed
- 7. Jeon K, Chung MP, Lee KS, et al. Prognostic factors and causes of death in Korean patients with idiopathic pulmonary fibrosis. Respir Med 2006; 100: 451-457. ArticlePubMed
- 8. American Thoracic Society. Idiopathic pulmonary fibrosis: diagnosis and treatment. International consensus statement. American Thoracic Society (ATS), and the European Respiratory Society (ERS). Am J Respir Crit Care Med 2000; 161(2 Pt 1): 646-664. ArticlePubMed
- 9. Ha SY, Roh MS. The new 2011 international Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society classification of lung adenocarcinoma in resected specimens: clinicopathologic relevance and emerging issues. Korean J Pathol 2013; 47: 316-325. ArticlePubMedPMC
- 10. Travis WD, Brambilla E, Noguchi M, et al. International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society: international multidisciplinary classification of lung adenocarcinoma: executive summary. Proc Am Thorac Soc 2011; 8: 381-385. ArticlePubMed
- 11. Vancheri C, Failla M, Crimi N, Raghu G. Idiopathic pulmonary fibrosis: a disease with similarities and links to cancer biology. Eur Respir J 2010; 35: 496-504. ArticlePubMed
- 12. Chilosi M, Poletti V, Rossi A. The pathogenesis of COPD and IPF: distinct horns of the same devil? Respir Res 2012; 13: 3.ArticlePubMedPMC
- 13. Ma Y, Seneviratne CK, Koss M. Idiopathic pulmonary fibrosis and malignancy. Curr Opin Pulm Med 2001; 7: 278-282. ArticlePubMed
- 14. Calabrese F, Lunardi F, Giacometti C, et al. Overexpression of squamous cell carcinoma antigen in idiopathic pulmonary fibrosis: clinicopathological correlations. Thorax 2008; 63: 795-802. ArticlePubMed
- 15. Hironaka M, Fukayama M. Pulmonary fibrosis and lung carcinoma: a comparative study of metaplastic epithelia in honeycombed areas of usual interstitial pneumonia with or without lung carcinoma. Pathol Int 1999; 49: 1060-1066. ArticlePubMedPDF
REFERENCES
| Case No. | Age (yr) | Sex | Histologic type | Size (cm) | Lobe | Segment | T | N | M | Stage | Smoking | SI (py) | PFT FEV1/FVC (%) | Procedure | CFP (mo) | SP (mo) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 60 | M | SQ | 3.5 | LLL | Superior | 2a | 1 | 0 | IIA | S | N/A | 89/81 | P | 0 | 0 |
| 2 | 70 | M | SQ | 5.5 | LLL | Bronchus | 2b | 1 | 0 | IIB | E | 35 | 108/101 | S | 58 | 0 |
| 3 | 66 | M | LCNE | 2.5 | RLL | Posterior basal | 1b | 2 | 0 | IIIA | N | 0 | 93/84 | L | 8 | 0 |
| 4 | 69 | M | SQ | 7.5 | LLL | Basal | 3 | 1 | 0 | IIIA | S | N/A | 65/84 | L | 0 | 1 |
| 5 | 71 | M | SQ | 5 | LUL | Apicoposterior | 2a | 0 | 0 | IB | N | 0 | 94/87 | L | 44 | 1 |
| 6 | 73 | M | SQ | 6.8 | LUL | Anterior | 2b | 2 | 0 | IIIA | E | 40 | 90/68 | L | 0 | 1 |
| 7 | 58 | M | Ad, SQ | 2.8, 1.1 | RUL | Anterior | 1b | 0 | 0 | IA | E | 25 | 77/85 | L | 60 | 1a |
| 8 | 68 | M | Ad | 4.5 | LLL | Posterior basal | 2a | 0 | 0 | IB | E | 40 | 123/104 | L | 18 | 1 |
| 9 | 57 | M | Ad | 2.2 | LLL | Anterior basal | 2a | 2 | 0 | IIIA | S | 40 | 79/67 | L | 11 | 2 |
| 10 | 63 | M | SQ | 4 | RLL | Lateral basal | 2a | 0 | 0 | IB | E | 40 | 87/90 | L | 0 | 4a |
| 11 | 59 | M | SQ | 4.8 | RLL | Superior | 2a | 0 | 0 | IB | E | 40 | 71/73 | L | 2 | 4a |
| 12 | 72 | M | Ad | 2 | LLL | Anterior basal | 1a | 0 | 0 | IA | N | 0 | 110/89 | L | 2 | 4 |
| 13 | 67 | M | LCC | 6 | LLL | Superior | 2b | 1 | 0 | IIB | S | 60 | 93/90 | P | 0 | 6 |
| 14 | 75 | M | Ad | 3.5 | RLL | Basal | 2a | 2 | 0 | IIIA | N | 0 | 103/88 | L | 0 | 8 |
| 15 | 72 | M | LCNE | 2.6 | RLL | Superior | 2a | 0 | 0 | IB | N | 0 | 94/96 | L | 13 | 9 |
| 16 | 69 | M | LCNE+SQ | 4 | RML | Bronchus | 2a | 2 | 0 | IIIA | E | 30 | 107/110 | L | 48 | 10a |
| 17 | 50 | M | Ad | 3.5 | LLL | Posterior basal | 2a | 2 | 0 | IIIA | E | N/A | 75/70 | L | 48 | 10a |
| 18 | 71 | M | SQ | 1.8 | RUL | Anterior | 1a | 0 | 0 | IA | E | 25 | 76/61 | W | 13 | 12a |
| 19 | 73 | M | SQ | 4.5 | RLL | Lateral basal | 2a | 2 | 0 | IIIA | E | N/A | 90/87 | L | 24 | 13a |
| 20 | 66 | M | Ad | 2.5 | LLL | Superior | 2a | 1 | 0 | IIA | E | 44 | 108/94 | L | 20 | 13 |
| 21 | 74 | M | Ad | 0.4 | LLL | Superior | 1a | 1 | 0 | IIA | S | 60 | 118/105 | L | 1 | 15 |
| 22 | 71 | M | Ad | 3 | LLL | Medial basal | 3 | 2 | 0 | IIIA | S | 49 | 80/89 | L | 20 | 15 |
| 23 | 76 | M | SQ | 2.3 | RUL | Anterior | 1b | 0 | 0 | IA | E | 50 | 83/77 | L | 0 | 16a |
| 24 | 63 | M | SCC+NSCC | 2.2 | RUL | Anterior | N/A | N/A | N/A | N/A | S | 20 | 88/77 | W | 1 | 17 |
| 25 | 70 | M | ASQ | 4.5 | RLL | Lateral basal | 1b | 1 | 0 | IIA | E | 47 | 96/82 | L | 84 | 17a |
| 26 | 84 | M | Ad | 1.7 | RUL | Posterior | 1b | 0 | 0 | IA | S | 58 | 105/91 | L | 31 | 19 |
| 27 | 71 | M | Ad | 4.8 | RLL | Lateral basal | 2a | 1 | 0 | IIA | S | 45 | 122/113 | L | 0 | 20 |
| 28 | 76 | M | SQ | 1.5 | RLL | Superior | 1a | 0 | 0 | IA | S | 50 | 76/83 | L | 0 | 21 |
| 29 | 76 | M | Ad | 2.2 | LLL | Superior | 1b | 2 | 0 | IIIA | S | 20 | 100/91 | L | 0 | 22 |
| 30 | 79 | M | SQ × 2 | 1.9, 0.4 | RLL | Superior | 2b | 0 | 0 | IIA | E | N/A | 96/75 | L | 65 | 26a |
| 31 | 65 | M | SQ | 2 | RLL | Lateral basal | 2a | 0 | 0 | IB | E | 38 | 90/85 | L | 0 | 29a |
| 32 | 73 | M | SQ | 3.1 | LLL | Posterior basal | 2a | 0 | 0 | IB | E | 50 | 92/86 | L | 0 | 29a |
| 33 | 70 | M | Pl | 3.3 | RLL | Superior | 2a | 0 | 0 | IB | S | N/A | 104/85 | L | 0 | 30 |
| 34 | 70 | M | Ad | 4.5 | RLL | Anterior basal | 2a | 0 | 0 | IB | N | 0 | 124/107 | L | 0 | 33 |
| 35 | 68 | M | SQ | 3 | RLL | Superior | 4 | 2 | 0 | IIIB | N/A | N/A | 102/88 | P | 8 | 38 |
| 36 | 54 | F | Ad | 3.5 | RLL | Anterior basal | 2a | 1 | 0 | IIA | N | 0 | 82/75 | L | 0 | 40 |
| 37 | 63 | M | SQ | 4 | LLL | Lateral basal | 2a | 0 | 0 | IB | S | 60 | 96/77 | L | 17 | 43a |
| 38 | 51 | F | Ad | 2.5 | RLL | Superior | 1b | 0 | 0 | IA | N | 0 | 87/71 | L | 0 | 53a |
| 39 | 64 | M | Ad | 1.8 | RUL | Anterior basal | 2a | 1 | 0 | IIA | E | 40 | 123/99 | L | 6 | 56 |
| 40 | 73 | M | Ad | 1 | RLL | Superior | 1a | 0 | 0 | IA | E | N/A | 79/81 | L | 0 | 63 |
| 41 | 71 | M | Ad | 2.8 | RLL | Superior | 1b | 1 | 0 | IIA | S | 60 | 95/103 | L | 0 | 82a |
| 42 | 60 | M | SQ | 3.5 | LUL | Anterior | 2a | 1 | 0 | IIA | E | 40 | 106/97 | L | 0 | 117 |
| 43 | 67 | M | SQ | 1.8 | LLL | Superior | 2a | 0 | 0 | IB | E | 40 | N/A | L | 0 | 160a |
SI, smoking index; py, packyears; PFT, pre-operative pulmonary function test; FEV1, forced expiratory volume at 1 second; FVC, forced vital capacity; CFP, cancer-free period; SP, survival period; M, male; SQ, squamous cell carcinoma; LLL, left lower lobe; S, current smoker; N/A, not available; P, pneumonectomy; E, ex-smoker; LCNE, large cell neuroendocrine carcinoma; RLL, right lower lobe; N, non-smoker; L, lobectomy; LUL, left upper lobe; Ad, adenocarcinoma; RUL, right upper lobe; LCC, large cell carcinoma; LCNE+SQ, combined large cell neuroendocrine carcinoma and squamous cell carcinoma; RML, right middle lobe; W, wedge resection; SCC, small cell carcinoma; NSCC, non-small cell carcinoma; ASQ, adenosquamous carcinoma; Pl, pleomorphic carcinoma; F, female.
aCensored.
| Parameter | Value |
|---|---|
| No. of patients (surgical diagnosis:nonsurgical diagnosis) | 57:27 |
| Mean age (yr) | 60 |
| Sex (male:female) | 66:18 |
| Smoking history (N:E:C) | 29:31:24 |
| Mean survival period (mo)a | 39.83 (2-117) |
| OR (95% CI) | p-value | |
|---|---|---|
| Smoking history (nonsmoking vs smoking) | 12.610 (1.293-123.016) | .029 |
| Smoking index (≤ 30 py vs > 30 py) | 0.528 (0.065-4.321) | .552 |
| FVC (> 86.5%a vs ≤ 86.5%) | 0.342 (0.090-1.308) | .117 |
| Age (≤ 70a yr vs > 70 yr) | 0.222 (0.070-0.709) | .011 |
| Stage (I vs II, III) | 0.310 (0.100-0.957) | .042 |
| Procedure (W vs L, P) | 0.026 (0.002-0.399) | .009 |
| CFP (≤ 2 mo vs > 2 mo) | 0.188 (0.062-0.567) | .003 |
| OR (95% CI) | p-value | |
|---|---|---|
| Smoking history (nonsmoking vs smoking) | 1.557 (0.799-3.033) | .193 |
| Smoking index (≤ 30 py vs > 30 py) | 0.913 (0.464-1.797) | .792 |
| FVC (≤ 80.5%a vs > 80.5%) | 0.804 (0.480-1.347) | .408 |
| Age (≤ 63a yr vs > 63 yr) | 0.699 (0.423-1.154) | .161 |
| Cancer (UIP-only vs UIP with cancer) | 0.461 (0.262-0.810) | .007 |
Figure & Data
References
Citations
- Treatable traits in interstitial lung disease: a narrative review
Megan Harrison, Chloe Lawler, Fiona Lake, Vidya Navaratnam, Caitlin Fermoyle, Yuben Moodley, Tamera J. Corte
Therapeutic Advances in Respiratory Disease.2025;[Epub] CrossRef - Usual Interstitial Pneumonia and Lung Cancer
Lamiyae Senhaji, Meryem Karhate, Abir Bouhamdi, Mounia Serraj, Mohamed ElBiaze, Mohammed Chakib Benjelloun, Badreddine Alami, Bouchra Amara
Cureus.2025;[Epub] CrossRef - Prognosis of idiopathic pulmonary fibrosis without anti-fibrotic therapy: a systematic review
Yet H. Khor, Yvonne Ng, Hayley Barnes, Nicole S.L. Goh, Christine F. McDonald, Anne E. Holland
European Respiratory Review.2020; 29(157): 190158. CrossRef - Linfoma difuso de células B grandes pulmonar en paciente con neumonía intersticial no específica
Luis Gorospe Sarasúa, Paola Arrieta, Anabelle Chinea-Rodríguez, Carlos de la Puente-Bujidos
Reumatología Clínica.2019; 15(6): e151. CrossRef - Diffuse Large B-cell Lymphoma of the Lung in a Patient With Nonspecific Interstitial Pneumonia
Luis Gorospe Sarasúa, Paola Arrieta, Anabelle Chinea-Rodríguez, Carlos de la Puente-Bujidos
Reumatología Clínica (English Edition).2019; 15(6): e151. CrossRef - Characteristics of lung cancer among patients with idiopathic pulmonary fibrosis and interstitial lung disease – analysis of institutional and population data
Joo Heung Yoon, Mehdi Nouraie, Xiaoping Chen, Richard H Zou, Jacobo Sellares, Kristen L Veraldi, Jared Chiarchiaro, Kathleen Lindell, David O Wilson, Naftali Kaminski, Timothy Burns, Humberto Trejo Bittar, Samuel Yousem, Kevin Gibson, Daniel J Kass
Respiratory Research.2018;[Epub] CrossRef - Genomic profiles of lung cancer associated with idiopathic pulmonary fibrosis
Ji An Hwang, Deokhoon Kim, Sung‐Min Chun, SooHyun Bae, Joon Seon Song, Mi Young Kim, Hyun Jung Koo, Jin Woo Song, Woo Sung Kim, Jae Cheol Lee, Hyeong Ryul Kim, Chang‐Min Choi, Se Jin Jang
The Journal of Pathology.2018; 244(1): 25. CrossRef - Survival after repeated surgery for lung cancer with idiopathic pulmonary fibrosis: a retrospective study
Seijiro Sato, Yuki Shimizu, Tatsuya Goto, Akihiko Kitahara, Terumoto Koike, Hiroyuki Ishikawa, Takehiro Watanabe, Masanori Tsuchida
BMC Pulmonary Medicine.2018;[Epub] CrossRef - Alveolar Squamous Cell Metaplasia: Preneoplastic Lesion?
Adriana Handra-Luca
Journal of Pathology and Translational Medicine.2018; 52(6): 355. CrossRef - Low expression of long noncoding RNA CDKN2B-AS1 in patients with idiopathic pulmonary fibrosis predicts lung cancer by regulating the p53-signaling pathway
Yufeng Du, Xiaoyan Hao, Xuejun Liu
Oncology Letters.2018;[Epub] CrossRef - A clinicopathological study of surgically resected lung cancer in patients with usual interstitial pneumonia
Yasutaka Watanabe, Yoshinori Kawabata, Nobuyuki Koyama, Tomohiko Ikeya, Eishin Hoshi, Noboru Takayanagi, Shinichiro Koyama
Respiratory Medicine.2017; 129: 158. CrossRef - Risk of the preoperative underestimation of tumour size of lung cancer in patients with idiopathic interstitial pneumonias
Mariko Fukui, Kazuya Takamochi, Takeshi Matsunaga, Shiaki Oh, Katsutoshi Ando, Kazuhiro Suzuki, Atsushi Arakawa, Toshimasa Uekusa, Kenji Suzuki
European Journal of Cardio-Thoracic Surgery.2016; 50(3): 428. CrossRef - The Idiopathic Interstitial Pneumonias: Histology and Imaging
Diane C. Strollo, Teri J. Franks, Jeffrey R. Galvin
Seminars in Roentgenology.2015; 50(1): 8. CrossRef - Do Chest Expansion Exercises Aid Re‐shaping the Diaphragm Within the First 72 Hours Following Lung Transplantation in a Usual Interstitial Pneumonia Patient?
Massimiliano Polastri, Erika Venturini, Saverio Pastore, Andrea Dell'Amore
Physiotherapy Research International.2015; 20(3): 191. CrossRef - Scrotal wall metastasis from a primary lung adenocarcinoma
Marie-Louise M. Coussa-Koniski, Pia A. Maalouf, Nehme E. Raad, Noha A. Bejjani
Respiratory Medicine Case Reports.2015; 15: 77. CrossRef - The Ratio KL-6 to SLX in Serum for Prediction of the Occurrence of Drug-Induced Interstitial Lung Disease in Lung Cancer Patients with Idiopathic Interstitial Pneumonias Receiving Chemotherapy
Kosuke Kashiwabara, Hiroshi Semba, Shinji Fujii, Shinsuke Tsumura, Ryota Aoki
Cancer Investigation.2015; 33(10): 516. CrossRef - Idiopathic pulmonary fibrosis will increase the risk of lung cancer
Li Junyao, Yang Ming, Li Ping, Su Zhenzhong, Gao Peng, Zhang Jie
Chinese Medical Journal.2014; 127(17): 3142. CrossRef
 PubReader
PubReader Cite this Article
Cite this Article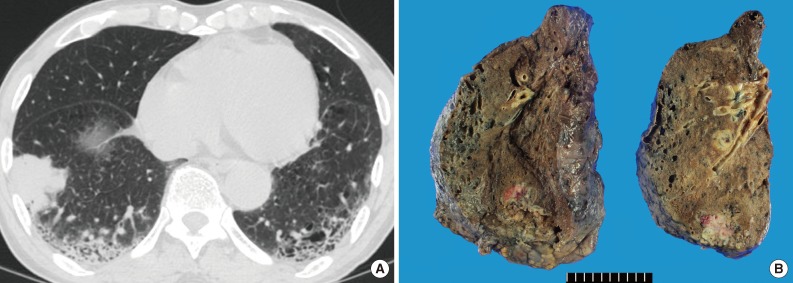
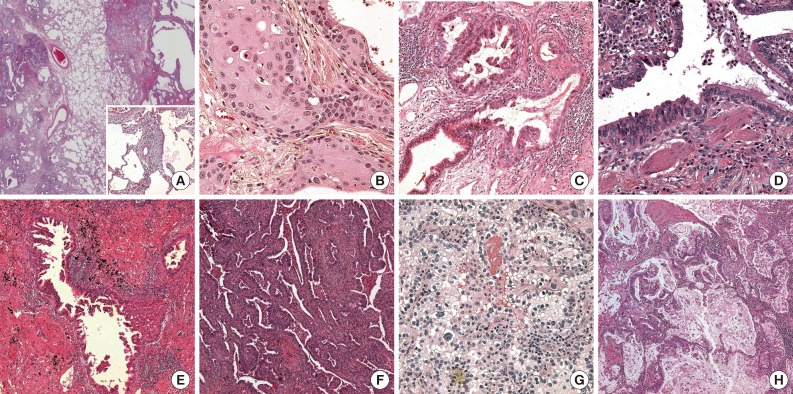


Fig. 1
Fig. 2
| Parameter | n (%) |
|---|---|
| Sex (male) | 41 (95) |
| Smoking history | 34 (79) |
| Mean age (yr) | 68 |
| TNM stage | |
| I | 19 (44) |
| II | 12 (28) |
| III | 11 (26) |
| N/A | 1 (2) |
| Surgical procedure | |
| Lobectomy | 37 (86) |
| Pneumonectomy | 3 (7) |
| Wedge resection | 2 (5) |
| Sleeve lobectomy | 1 (2) |
| Histologic type | |
| Squamous cell carcinoma | 18 (42) |
| Adenocarcinoma | 17 (40) |
| LCNE | 2 (5) |
| Combined carcinoma | 2 (5) |
| Others | 4 (9) |
| Location (lobe) | |
| Right lower | 18 (42) |
| Left lower | 15 (35) |
| Right upper | 6 (14) |
| Left upper | 3 (7) |
| Right middle | 1 (2) |
| Less than 1 month of cancer-free period | 20 (47) |
| 1-Year survival rate | 26 (60) |
| Case No. | Age (yr) | Sex | Histologic type | Size (cm) | Lobe | Segment | T | N | M | Stage | Smoking | SI (py) | PFT FEV1/FVC (%) | Procedure | CFP (mo) | SP (mo) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 60 | M | SQ | 3.5 | LLL | Superior | 2a | 1 | 0 | IIA | S | N/A | 89/81 | P | 0 | 0 |
| 2 | 70 | M | SQ | 5.5 | LLL | Bronchus | 2b | 1 | 0 | IIB | E | 35 | 108/101 | S | 58 | 0 |
| 3 | 66 | M | LCNE | 2.5 | RLL | Posterior basal | 1b | 2 | 0 | IIIA | N | 0 | 93/84 | L | 8 | 0 |
| 4 | 69 | M | SQ | 7.5 | LLL | Basal | 3 | 1 | 0 | IIIA | S | N/A | 65/84 | L | 0 | 1 |
| 5 | 71 | M | SQ | 5 | LUL | Apicoposterior | 2a | 0 | 0 | IB | N | 0 | 94/87 | L | 44 | 1 |
| 6 | 73 | M | SQ | 6.8 | LUL | Anterior | 2b | 2 | 0 | IIIA | E | 40 | 90/68 | L | 0 | 1 |
| 7 | 58 | M | Ad, SQ | 2.8, 1.1 | RUL | Anterior | 1b | 0 | 0 | IA | E | 25 | 77/85 | L | 60 | 1 |
| 8 | 68 | M | Ad | 4.5 | LLL | Posterior basal | 2a | 0 | 0 | IB | E | 40 | 123/104 | L | 18 | 1 |
| 9 | 57 | M | Ad | 2.2 | LLL | Anterior basal | 2a | 2 | 0 | IIIA | S | 40 | 79/67 | L | 11 | 2 |
| 10 | 63 | M | SQ | 4 | RLL | Lateral basal | 2a | 0 | 0 | IB | E | 40 | 87/90 | L | 0 | 4 |
| 11 | 59 | M | SQ | 4.8 | RLL | Superior | 2a | 0 | 0 | IB | E | 40 | 71/73 | L | 2 | 4 |
| 12 | 72 | M | Ad | 2 | LLL | Anterior basal | 1a | 0 | 0 | IA | N | 0 | 110/89 | L | 2 | 4 |
| 13 | 67 | M | LCC | 6 | LLL | Superior | 2b | 1 | 0 | IIB | S | 60 | 93/90 | P | 0 | 6 |
| 14 | 75 | M | Ad | 3.5 | RLL | Basal | 2a | 2 | 0 | IIIA | N | 0 | 103/88 | L | 0 | 8 |
| 15 | 72 | M | LCNE | 2.6 | RLL | Superior | 2a | 0 | 0 | IB | N | 0 | 94/96 | L | 13 | 9 |
| 16 | 69 | M | LCNE+SQ | 4 | RML | Bronchus | 2a | 2 | 0 | IIIA | E | 30 | 107/110 | L | 48 | 10 |
| 17 | 50 | M | Ad | 3.5 | LLL | Posterior basal | 2a | 2 | 0 | IIIA | E | N/A | 75/70 | L | 48 | 10 |
| 18 | 71 | M | SQ | 1.8 | RUL | Anterior | 1a | 0 | 0 | IA | E | 25 | 76/61 | W | 13 | 12 |
| 19 | 73 | M | SQ | 4.5 | RLL | Lateral basal | 2a | 2 | 0 | IIIA | E | N/A | 90/87 | L | 24 | 13 |
| 20 | 66 | M | Ad | 2.5 | LLL | Superior | 2a | 1 | 0 | IIA | E | 44 | 108/94 | L | 20 | 13 |
| 21 | 74 | M | Ad | 0.4 | LLL | Superior | 1a | 1 | 0 | IIA | S | 60 | 118/105 | L | 1 | 15 |
| 22 | 71 | M | Ad | 3 | LLL | Medial basal | 3 | 2 | 0 | IIIA | S | 49 | 80/89 | L | 20 | 15 |
| 23 | 76 | M | SQ | 2.3 | RUL | Anterior | 1b | 0 | 0 | IA | E | 50 | 83/77 | L | 0 | 16 |
| 24 | 63 | M | SCC+NSCC | 2.2 | RUL | Anterior | N/A | N/A | N/A | N/A | S | 20 | 88/77 | W | 1 | 17 |
| 25 | 70 | M | ASQ | 4.5 | RLL | Lateral basal | 1b | 1 | 0 | IIA | E | 47 | 96/82 | L | 84 | 17 |
| 26 | 84 | M | Ad | 1.7 | RUL | Posterior | 1b | 0 | 0 | IA | S | 58 | 105/91 | L | 31 | 19 |
| 27 | 71 | M | Ad | 4.8 | RLL | Lateral basal | 2a | 1 | 0 | IIA | S | 45 | 122/113 | L | 0 | 20 |
| 28 | 76 | M | SQ | 1.5 | RLL | Superior | 1a | 0 | 0 | IA | S | 50 | 76/83 | L | 0 | 21 |
| 29 | 76 | M | Ad | 2.2 | LLL | Superior | 1b | 2 | 0 | IIIA | S | 20 | 100/91 | L | 0 | 22 |
| 30 | 79 | M | SQ × 2 | 1.9, 0.4 | RLL | Superior | 2b | 0 | 0 | IIA | E | N/A | 96/75 | L | 65 | 26 |
| 31 | 65 | M | SQ | 2 | RLL | Lateral basal | 2a | 0 | 0 | IB | E | 38 | 90/85 | L | 0 | 29 |
| 32 | 73 | M | SQ | 3.1 | LLL | Posterior basal | 2a | 0 | 0 | IB | E | 50 | 92/86 | L | 0 | 29 |
| 33 | 70 | M | Pl | 3.3 | RLL | Superior | 2a | 0 | 0 | IB | S | N/A | 104/85 | L | 0 | 30 |
| 34 | 70 | M | Ad | 4.5 | RLL | Anterior basal | 2a | 0 | 0 | IB | N | 0 | 124/107 | L | 0 | 33 |
| 35 | 68 | M | SQ | 3 | RLL | Superior | 4 | 2 | 0 | IIIB | N/A | N/A | 102/88 | P | 8 | 38 |
| 36 | 54 | F | Ad | 3.5 | RLL | Anterior basal | 2a | 1 | 0 | IIA | N | 0 | 82/75 | L | 0 | 40 |
| 37 | 63 | M | SQ | 4 | LLL | Lateral basal | 2a | 0 | 0 | IB | S | 60 | 96/77 | L | 17 | 43 |
| 38 | 51 | F | Ad | 2.5 | RLL | Superior | 1b | 0 | 0 | IA | N | 0 | 87/71 | L | 0 | 53 |
| 39 | 64 | M | Ad | 1.8 | RUL | Anterior basal | 2a | 1 | 0 | IIA | E | 40 | 123/99 | L | 6 | 56 |
| 40 | 73 | M | Ad | 1 | RLL | Superior | 1a | 0 | 0 | IA | E | N/A | 79/81 | L | 0 | 63 |
| 41 | 71 | M | Ad | 2.8 | RLL | Superior | 1b | 1 | 0 | IIA | S | 60 | 95/103 | L | 0 | 82 |
| 42 | 60 | M | SQ | 3.5 | LUL | Anterior | 2a | 1 | 0 | IIA | E | 40 | 106/97 | L | 0 | 117 |
| 43 | 67 | M | SQ | 1.8 | LLL | Superior | 2a | 0 | 0 | IB | E | 40 | N/A | L | 0 | 160 |
| Parameter | Value |
|---|---|
| No. of patients (surgical diagnosis:nonsurgical diagnosis) | 57:27 |
| Mean age (yr) | 60 |
| Sex (male:female) | 66:18 |
| Smoking history (N:E:C) | 29:31:24 |
| Mean survival period (mo) |
39.83 (2-117) |
| Lung cancer with UIP (n = 43) | UIP-only (n = 84) | p-value | |
|---|---|---|---|
| Age (yr) | 67.9 ± 7.2 | 60.3 ± 7.7 | < .001 |
| Sex (male:female) | 41:2 (95.3) | 65:19 (77.4) | .01 |
| Smoking history | 34 (79.1) | 55 (65.5) | .113 |
| More than 30 py | 81.5% | 60.0% | .052 |
| OR (95% CI) | p-value | |
|---|---|---|
| Smoking history (nonsmoking vs smoking) | 12.610 (1.293-123.016) | .029 |
| Smoking index (≤ 30 py vs > 30 py) | 0.528 (0.065-4.321) | .552 |
| FVC (> 86.5% |
0.342 (0.090-1.308) | .117 |
| Age (≤ 70 |
0.222 (0.070-0.709) | .011 |
| Stage (I vs II, III) | 0.310 (0.100-0.957) | .042 |
| Procedure (W vs L, P) | 0.026 (0.002-0.399) | .009 |
| CFP (≤ 2 mo vs > 2 mo) | 0.188 (0.062-0.567) | .003 |
| OR (95% CI) | p-value | |
|---|---|---|
| Smoking history (nonsmoking vs smoking) | 1.557 (0.799-3.033) | .193 |
| Smoking index (≤ 30 py vs > 30 py) | 0.913 (0.464-1.797) | .792 |
| FVC (≤ 80.5% |
0.804 (0.480-1.347) | .408 |
| Age (≤ 63 |
0.699 (0.423-1.154) | .161 |
| Cancer (UIP-only vs UIP with cancer) | 0.461 (0.262-0.810) | .007 |
LCNE, large cell neuroendocrine carcinoma.
SI, smoking index; py, packyears; PFT, pre-operative pulmonary function test; FEV1, forced expiratory volume at 1 second; FVC, forced vital capacity; CFP, cancer-free period; SP, survival period; M, male; SQ, squamous cell carcinoma; LLL, left lower lobe; S, current smoker; N/A, not available; P, pneumonectomy; E, ex-smoker; LCNE, large cell neuroendocrine carcinoma; RLL, right lower lobe; N, non-smoker; L, lobectomy; LUL, left upper lobe; Ad, adenocarcinoma; RUL, right upper lobe; LCC, large cell carcinoma; LCNE+SQ, combined large cell neuroendocrine carcinoma and squamous cell carcinoma; RML, right middle lobe; W, wedge resection; SCC, small cell carcinoma; NSCC, non-small cell carcinoma; ASQ, adenosquamous carcinoma; Pl, pleomorphic carcinoma; F, female. Censored.
N, non-smoker; E, ex-smoker; C, current smoker. The dead:the censored=46:38.
Values are presented as mean±standard deviation or number (%), unless indicated otherwise. UIP, usual interstitial pneumonia; py, pack years.
OR, odds ratio; CI, confidence interval; Smoking, ex-smoker and current smoker; py, pack years; FVC, forced vital capacity; W, wedge resection; L, lobectomy; P, pneumonectomy; CFP, cancer free period. Median number.
UIP, usual interstitial pneumonia; OR, odds ratio; CI, confidence interval; Smoking, ex-smoker and current smoker; py, pack years; FVC, forced vital capacity. Median number.

