 E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 48(2); 2014 > Article
-
Original Article
Incidence and Malignancy Rates of Diagnoses in the Bethesda System for Reporting Thyroid Aspiration Cytology: An Institutional Experience - Ji Hye Park, Sun Och Yoon, Eun Ju Son1, Hye Min Kim, Ji Hae Nahm, SoonWon Hong
-
Korean Journal of Pathology 2014;48(2):133-139.
DOI: https://doi.org/10.4132/KoreanJPathol.2014.48.2.133
Published online: April 28, 2014
Department of Pathology, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
1Department of Radiology, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
- Corresponding Author: SoonWon Hong, M.D. Department of Pathology, Gangnam Severance Hospital, Yonsei University College of Medicine, 211 Eonju-ro, Gangnam-gu, Seoul 135-720, Korea. Tel: +82-2-2019-3543, Fax: +82-2-3463-2103, soonwonh@yuhs.ac
© 2014 The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
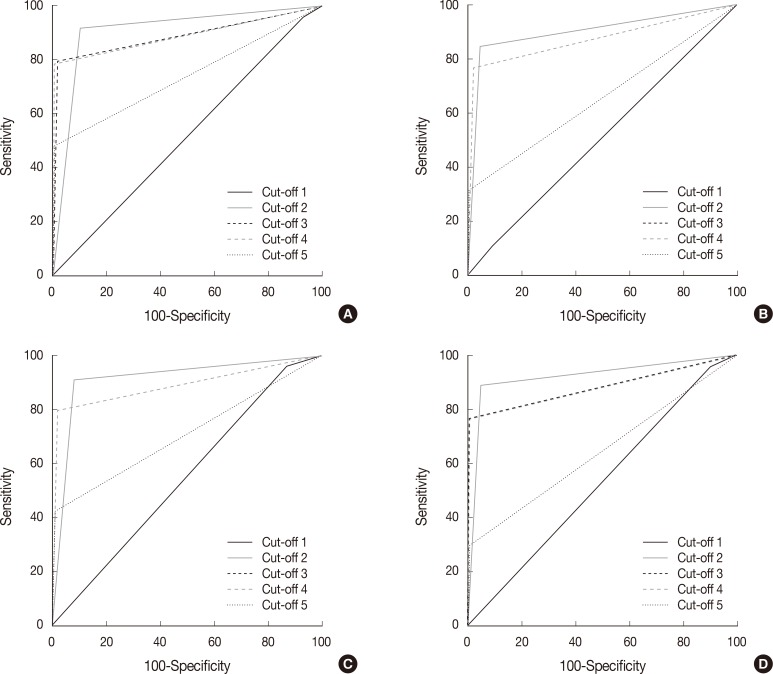
Figure & Data
References
Citations
- Assessment of an innovative synthetic matrix for enhanced cell preservation: evaluating its clinical utility and impact on diagnostic precision in thyroid fine-needle aspiration cytology
Diana-Raluca Streinu, Octavian Constantin Neagoe, Andreea Bena, Dana-Liana Stoian
BMC Endocrine Disorders.2026;[Epub] CrossRef - National Trends in Thyroidectomy and Molecular Diagnostic Utilization: A Medicare Analysis (2016–2023)
David Z. Allen, J. Walker Rosenthal, Matthew L. Harris, Maxwell P. Kligerman, Meredith A. Lilly, Merry E. Sebelik
The Laryngoscope.2026;[Epub] CrossRef - The Malignancy Rates of the Bethesda System for Reporting Thyroid Cytopathology: A 10-year Experience in a Single Asian Institute
Sarah I Liew, Nor S Ahmad, Navarasi R Gopal
World Journal of Endocrine Surgery.2025; 16(2): 42. CrossRef - Assessment of Thyroid Fine-Needle Aspirates Using 2023 Bethesda System
Niti Sureka, Charanjeet Ahluwalia, Sana Ahuja, Neha Kawatra Madan, Meetu Agrawal, Sunil Ranga
Acta Cytologica.2025; 69(3): 280. CrossRef - A Comprehensive Approach to the Thyroid Bethesda Category III (AUS) in the Transition Zone Between 2nd Edition and 3rd Edition of The Bethesda System for Reporting Thyroid Cytopathology: Subcategorization, Nuclear Scoring, and More
Merve Bagıs, Nuray Can, Necdet Sut, Ebru Tastekin, Ezgi Genc Erdogan, Buket Yilmaz Bulbul, Yavuz Atakan Sezer, Osman Kula, Elif Mercan Demirtas, Inci Usta
Endocrine Pathology.2024; 35(1): 51. CrossRef - Evaluation of the Efficacy of Thyroid Imaging Reporting and Data Systems Classification in Risk Stratification and in the Management of Thyroid Swelling by Comparing It With Fine-Needle Aspiration Cytology and Histopathological Examination
Abhishek K Saw, Zenith H Kerketta, Khushboo Rani, Krishna Murari, Kritika Srivastava, Ajay Kumar, Sunny LNU, Anish Baxla, Nabu Kumar, Nusrat Noor
Cureus.2024;[Epub] CrossRef - A COMPARATIVE STUDY BETWEEN CONVENTIONAL METHOD AND THE BETHESDA SYSTEM FOR REPORTING THYROID CYTOPATHOLOGY
Pooja Mangal, Arti Gupta
GLOBAL JOURNAL FOR RESEARCH ANALYSIS.2023; : 67. CrossRef - Study of Fine Needle Aspiration Cytology (FNAC) of Thyroid Gland According to the Bethesda System
Keval A Patel, Garima Anandani, Bhawana S Sharma, Riddhi A Parmar
Cureus.2023;[Epub] CrossRef - Correlation of Thyroid Fine Needle Aspiration Biopsy With Histopathological Results
Cemalettin Durgun
Cureus.2023;[Epub] CrossRef - The Bethesda System for Reporting Thyroid Cytopathology: Validating at Tribhuvan University Teaching Hospital
Kunjan Acharya, Shreya Shrivastav, Prashant Triipathi, Bigyan Raj Gyawali, Bijaya Kharel, Dharma Kanta Baskota, Pallavi Sinha
International Archives of Otorhinolaryngology.2022; 26(01): e097. CrossRef - Validating the ‘CUT score’ risk stratification tool for indeterminate thyroid nodules using the Bethesda system for reporting thyroid cytopathology
Sapir Pinhas, Idit Tessler, Luba Pasherstnik Bizer, Khaled khalilia, Meir Warman, Meital Adi, Doron Halperin, Oded Cohen
European Archives of Oto-Rhino-Laryngology.2022; 279(1): 383. CrossRef - ANALYSIS OF FINE NEEDLE ASPIRATIONS OF THE THYROID: CYTOLOGICAL-HISTOPATHOLOGICAL CORRELATION AND OUTCOMES OF THE BETHESDA SYSTEM
Ayca TAN
SDÜ Tıp Fakültesi Dergisi.2022; 29(2): 213. CrossRef - Reproducibility of Cytomorphological Diagnosis and Assessment of Risk of Malignancy of Thyroid Nodules Based on the Bethesda System for Reporting Thyroid Cytopathology
Sasmita Panda, Mamita Nayak, Lucy Pattanayak, Paresh Kumar Behera, Sagarika Samantaray, Sashibhusan Dash
Journal of Microscopy and Ultrastructure.2022; 10(4): 174. CrossRef - Comparative analysis of cytomorphology of thyroid lesion on conventional cytology versus liquid-based cytology and categorize the lesions according to The Bethesda System for Reporting Thyroid Cytopathology
M Qamar Alam, Pinki Pandey, Megha Ralli, Jitendra Pratap Singh Chauhan, Roopak Aggarwal, Vineet Chaturvedi, Asttha Kapoor, Kapil Trivedi, Savita Agarwal
Journal of Cancer Research and Therapeutics.2022; 18(Suppl 2): S259. CrossRef - Thyroid cytology in Pakistan: An institutional audit of the atypia of undetermined significance/follicular lesion of undetermined significance category
Saira Fatima, Rabia Qureshi, Sumbul Imran, Romana Idrees, Zubair Ahmad, Naila Kayani, Arsalan Ahmed
Cytopathology.2021; 32(2): 205. CrossRef - Outcomes of the Bethesda system for reporting thyroid cytopathology: Real‐life experience
Galit Avior, Or Dagan, Isaac Shochat, Yulia Frenkel, Idit Tessler, Alona Meir, Anat Jaffe, Oded Cohen
Clinical Endocrinology.2021; 94(3): 521. CrossRef - National differences in cost analysis of Afirma Genomic sequencing classifier
Ohad Ronen, Maya Oichman
Clinical Endocrinology.2021; 94(4): 717. CrossRef - Thyroid malignancy rates according to the Bethesda reporting system in Israel - A multicenter study
Ory Madgar, Galit Avior, Isaac Shochat, Ben-Zion Joshua, Lior Baraf, Yuval Avidor, Avi khafif, Niddal Assadi, Eran E. Alon
European Journal of Surgical Oncology.2021; 47(6): 1370. CrossRef - Application of the Bethesda system for reporting thyroid cytopathology for classification of thyroid nodules: A clinical and cytopathological characteristics in Bhutanese population
Sonam Choden, Chimi Wangmo, Sushna Maharjan
Diagnostic Cytopathology.2021; 49(11): 1179. CrossRef - Malignancy rates in thyroid nodules classified as Bethesda categories III and IV; a subcontinent perspective
Adnan Zahid, Waqas Shafiq, Khawaja Shehryar Nasir, Asif Loya, Syed Abbas Raza, Sara Sohail, Umal Azmat
Journal of Clinical & Translational Endocrinology.2021; 23: 100250. CrossRef - The combination of ACR‐Thyroid Imaging Reporting and Data system and The Bethesda System for Reporting Thyroid Cytopathology in the evaluation of thyroid nodules—An institutional experience
Shanmugasundaram Sakthisankari, Sreenivasan Vidhyalakshmi, Sivanandam Shanthakumari, Balalakshmoji Devanand, Udayasankar Nagul
Cytopathology.2021; 32(4): 472. CrossRef - Ultrasound-guided fine needle aspiration cytology and ultrasound examination of thyroid nodules in the UAE: A comparison
Suhail Al-Salam, Charu Sharma, Maysam T. Abu Sa’a, Bachar Afandi, Khaled M. Aldahmani, Alia Al Dhaheri, Hayat Yahya, Duha Al Naqbi, Esraa Al Zuraiqi, Baraa Kamal Mohamed, Shamsa Ahmed Almansoori, Meera Al Zaabi, Aysha Al Derei, Amal Al Shamsi, Juma Al Kaa
PLOS ONE.2021; 16(4): e0247807. CrossRef - Incidence, Clinical Characteristics, and Histopathological Results of Atypia of Undermined Significance in a Tertiary Center in UAE
Maha Osman Shangab, Azza Abdulaziz Khalifa, Fatheya Al Awadi, Mouza Alsharhan, Alaaeldin Bashier
Dubai Diabetes and Endocrinology Journal.2021; 27(1): 1. CrossRef - McGill Thyroid Nodule Score in Differentiating Thyroid Nodules in Total Thyroidectomy Cases of Indeterminate Nodules
Hadi A Al-Hakami, Reem Al-Mohammadi, Rami Al-Mutairi, Haya Al-Subaie, Mohammed A Al Garni
Indian Journal of Surgical Oncology.2020; 11(2): 268. CrossRef - The Bethesda System for Reporting Thyroid Cytopathology: A Cytohistological Study
Bakiarathana Anand, Anita Ramdas, Marie Moses Ambroise, Nirmal P. Kumar
Journal of Thyroid Research.2020; 2020: 1. CrossRef - Differences in cytopathologist thyroid nodule malignancy rate
Ohad Ronen, Hector Cohen, Eyal Sela, Mor Abu
Cytopathology.2020; 31(4): 315. CrossRef - Thyroid Multimodal Ultrasound Evaluation—Impact on Presurgical Diagnosis of Intermediate Cytology Cases
Andreea Borlea, Dana Stoian, Laura Cotoi, Ioan Sporea, Fulger Lazar, Ioana Mozos
Applied Sciences.2020; 10(10): 3439. CrossRef - Fine-needle aspiration cytology of nodular thyroid lesions: A 1-year experience of the thyroid cytopathology in a large regional and a University Hospital, with histological correlation
Kaumudi Konkay, Radhika Kottu, Mutheeswaraiah Yootla, Narendra Hulikal
Thyroid Research and Practice.2019; 16(2): 60. CrossRef - Review of a single institution's fine needle aspiration results for thyroid nodules: Initial observations and lessons for the future
Ohad Ronen, Hector Cohen, Mor Abu
Cytopathology.2019; 30(5): 468. CrossRef - Strain Elastography as a Valuable Diagnosis Tool in Intermediate Cytology (Bethesda III) Thyroid Nodules
Dana Stoian, Florin Borcan, Izabella Petre, Ioana Mozos, Flore Varcus, Viviana Ivan, Andreea Cioca, Adrian Apostol, Cristina Adriana Dehelean
Diagnostics.2019; 9(3): 119. CrossRef - Improvement of diagnostic performance of pathologists by reducing the number of pathologists responsible for thyroid fine needle aspiration cytology: An institutional experience
Jae Yeon Seok, Jungsuk An, Hyun Yee Cho
Diagnostic Cytopathology.2018; 46(7): 561. CrossRef - Bethesda Classification and Cytohistological Correlation of Thyroid Nodules in a Brazilian Thyroid Disease Center
Kassia B. Reuters, Maria C.O.C. Mamone, Elsa S. Ikejiri, Cleber P. Camacho, Claudia C.D. Nakabashi, Carolina C.P.S. Janovsky, Ji H. Yang, Danielle M. Andreoni, Rosalia Padovani, Rui M.B. Maciel, Felipe A.B. Vanderlei, Rosa P.M. Biscolla
European Thyroid Journal.2018; 7(3): 133. CrossRef - The impact of rapid on‐site evaluation on thyroid fine‐needle aspiration biopsy: A 2‐year cancer center institutional experience
Ricardo G. Pastorello, Camila Destefani, Pedro H. Pinto, Caroline H. Credidio, Rafael X. Reis, Thiago de A. Rodrigues, Maryane C. de Toledo, Louise De Brot, Felipe de A. Costa, Antonio G. do Nascimento, Clóvis A. L. Pinto, Mauro A. Saieg
Cancer Cytopathology.2018; 126(10): 846. CrossRef - The Use of the Bethesda System for Reporting Thyroid Cytopathology in Korea: A Nationwide Multicenter Survey by the Korean Society of Endocrine Pathologists
Mimi Kim, Hyo Jin Park, Hye Sook Min, Hyeong Ju Kwon, Chan Kwon Jung, Seoung Wan Chae, Hyun Ju Yoo, Yoo Duk Choi, Mi Ja Lee, Jeong Ja Kwak, Dong Eun Song, Dong Hoon Kim, Hye Kyung Lee, Ji Yeon Kim, Sook Hee Hong, Jang Sihn Sohn, Hyun Seung Lee, So Yeon Pa
Journal of Pathology and Translational Medicine.2017; 51(4): 410. CrossRef - Thyroid FNA cytology in Asian practice—Active surveillance for indeterminate thyroid nodules reduces overtreatment of thyroid carcinomas
K. Kakudo, M. Higuchi, M. Hirokawa, S. Satoh, C. K. Jung, A. Bychkov
Cytopathology.2017; 28(6): 455. CrossRef - Thyroid Fine-Needle Aspiration Cytology Practice in Korea
Yoon Jin Cha, Ju Yeon Pyo, SoonWon Hong, Jae Yeon Seok, Kyung-Ju Kim, Jee-Young Han, Jeong Mo Bae, Hyeong Ju Kwon, Yeejeong Kim, Kyueng-Whan Min, Soonae Oak, Sunhee Chang
Journal of Pathology and Translational Medicine.2017; 51(6): 521. CrossRef - Bethesda System for Reporting Thyroid Cytopathology: A three-year study at a tertiary care referral center in Saudi Arabia
Mohamed Abdulaziz Al Dawish, Asirvatham Alwin Robert, Aljuboury Muna, Alkharashi Eyad, Abdullah Al Ghamdi, Khalid Al Hajeri, Mohammed A Thabet, Rim Braham
World Journal of Clinical Oncology.2017; 8(2): 151. CrossRef - A meta‐analytic review of the Bethesda System for Reporting Thyroid Cytopathology: Has the rate of malignancy in indeterminate lesions been underestimated?
Patrizia Straccia, Esther Diana Rossi, Tommaso Bizzarro, Chiara Brunelli, Federica Cianfrini, Domenico Damiani, Guido Fadda
Cancer Cytopathology.2015; 123(12): 713. CrossRef - Value of TIRADS, BSRTC and FNA-BRAFV600E mutation analysis in differentiating high-risk thyroid nodules
Yu-zhi Zhang, Ting Xu, Dai Cui, Xiao Li, Qing Yao, Hai-yan Gong, Xiao-yun Liu, Huan-huan Chen, Lin Jiang, Xin-hua Ye, Zhi-hong Zhang, Mei-ping Shen, Yu Duan, Tao Yang, Xiao-hong Wu
Scientific Reports.2015;[Epub] CrossRef - A study of malignancy rates in different diagnostic categories of the Bethesda system for reporting thyroid cytopathology: An institutional experience
P. Arul, C. Akshatha, Suresh Masilamani
Biomedical Journal.2015; 38(6): 517. CrossRef - Diagnostic accuracy of Bethesda system for reporting thyroid cytopathology: an institutional perspective
Samreen Naz, Atif Hashmi, Amna khurshid, Naveen Faridi, Muhammad Edhi, Anwar Kamal, Mehmood Khan
International Archives of Medicine.2014; 7(1): 46. CrossRef
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-
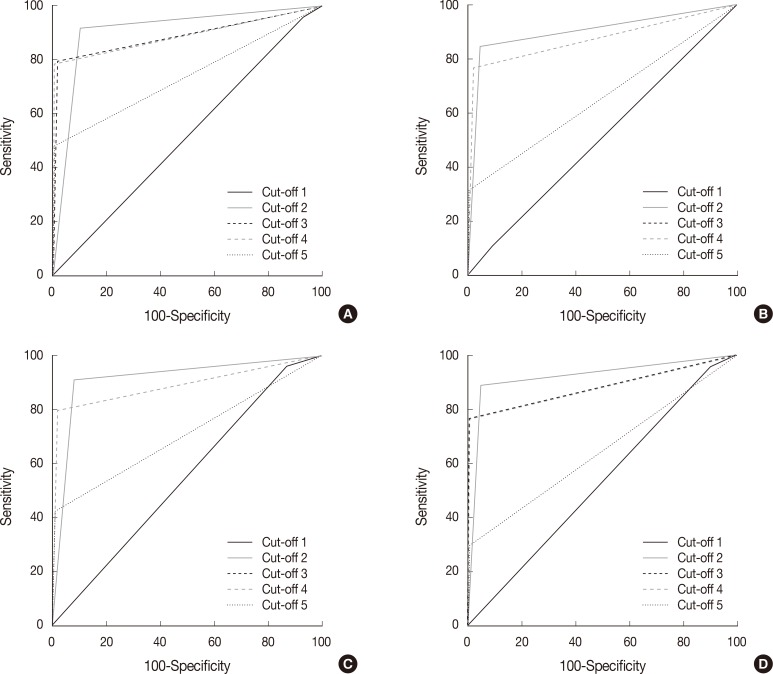

Fig. 1
| Diagnostic category of Bethesda system | Cytopathologists |
Total (n = 1,730) | |||
|---|---|---|---|---|---|
| A (n = 348) | B (n = 330) | C (n = 382) | D (n = 670) | ||
| I | 28 (8.0) | 50 (15.1) | 63 (16.5) | 89 (13.3) | 230 (13.3) |
| II | 128 (36.8) | 151 (45.8) | 122 (31.9) | 301 (44.9) | 702 (40.6) |
| III | 41 (11.8) | 18 (5.5) | 40 (10.5) | 58 (8.7) | 157 (9.1) |
| IV | 5 (1.4) | 0 (0) | 1 (0.3) | 1 (0.1) | 7 (0.4) |
| V | 57 (16.4) | 66 (20.0) | 75 (19.6) | 137 (20.5) | 335 (19.3) |
| VI | 89 (25.6) | 45 (13.6) | 81 (21.2) | 84 (12.5) | 299 (17.3) |
| Diagnostic category of Bethesda system | Follow-up diagnosis |
|||||
|---|---|---|---|---|---|---|
| BN | PTC | MTC | FC | PD | Malignancy | |
| I (n = 116) | 75 (64.7) | 41 (35.3) | 0 (0) | 0 (0) | 0 (0) | 41 (35.3) |
| II (n = 702) | 663 (94.5) | 36 (5.1) | 0 (0) | 2 (0.3) | 1 (0.1) | 39 (5.6) |
| III (n = 126) | 39 (30.9) | 84 (66.7) | 1 (0.8) | 2 (1.6) | 0 (0) | 87 (69.0) |
| IV (n = 4) | 2 (50.0) | 2 (50.0) | 0 (0) | 0 (0) | 0 (0) | 2 (50.0) |
| V (n = 314) | 4 (1.3) | 306 (97.4) | 3 (1.0) | 0 (0) | 1 (0.3) | 310 (98.7) |
| VI (n = 285) | 3 (1.1) | 282 (98.9) | 0 (0) | 0 (0) | 0 (0) | 282 (98.9) |
| Diagnostic category of Bethesda system | Cytopathologists |
|||
|---|---|---|---|---|
| A (M/T) | B (M/T) | C (M/T) | D (M/T) | |
| I | 41.2 (7/17) | 48.4 (15/31) | 28.0 (7/25) | 27.9 (12/43) |
| II | 4.7 (6/128) | 4.0 (6/151) | 7.4 (9/122) | 6.0 (18/301) |
| III | 63.6 (21/33) | 73.3 (11/15) | 70.0 (21/30) | 70.8 (34/48) |
| IV | 33.3 (1/3) | 0 (0/0) | 0 (0/0) | 100.0 (1/1) |
| V | 100.0 (51/51) | 95.4 (62/65) | 100.0 (68/68) | 99.2 (129/130) |
| VI | 98.8 (80/81) | 100.0 (43/43) | 98.7 (78/79) | 98.8 (81/82) |
| Total | 53.0 (166/313) | 44.9 (137/305) | 56.5 (183/324) | 45.5 (275/605) |
| Cytopathologists |
||||
|---|---|---|---|---|
| A | B | C | D | |
| Sensitivity | 79.5 | 76.6 | 79.8 | 76.7 |
| Specificity | 98.0 | 98.2 | 99.3 | 99.4 |
| False negative rate | 20.5 | 23.4 | 20.2 | 23.3 |
| False positive rate | 2.0 | 1.8 | 0.7 | 0.6 |
| Positive predictive value | 97.8 | 97.2 | 99.3 | 99.1 |
| Negative predictive value | 80.9 | 83.8 | 79.1 | 83.7 |
| Diagnostic category of Bethesda system | Present study | Mondal et al. [3] | Jo et al. [4] | Yassa et al. [5] | Yang et al. [6] | Nayar and Ivanovic [7] | Theoharis et al. [8] | Mufti and Molah [9] | Baloch et al. [10] | Stamataki et al. [11] | Wu et al. [12] | Lee et al. [13] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| I | 13.3 | 1.2 | 18.6 | 7.0 | 10.4 | 5.0 | 11.1 | 11.6 | 17.5 | 4.0 | 20.1 | 10.0 |
| II | 40.6 | 87.5 | 59.0 | 66.0 | 64.6 | 64.0 | 73.8 | 77.6 | 15.8 | 74.6 | 39.0 | 67.7 |
| III | 9.1 | 1.0 | 3.4 | 4.0 | 3.2 | 18.0 | 3.0 | 0.8 | 9.8 | 6.7 | 27.2 | 3.1 |
| IV | 0.4 | 4.2 | 9.7 | 9.0 | 11.6 | 6.0 | 5.5 | 4.0 | 16.5 | - | 8.4 | 0.6 |
| V | 19.3 | 1.4 | 2.3 | 9.0 | 2.6 | 2.0 | 1.4 | 2.4 | 19.1 | 2.8 | 2.6 | 5.1 |
| VI | 17.3 | 4.7 | 7.0 | 5.0 | 7.6 | 5.0 | 5.2 | 3.6 | 21.3 | 11.9 | 2.7 | 13.0 |
| Diagnostic category of Bethesda system | Present study | Mondal et al. [3] | Jo et al. [4] | Yassa et al. [5] | Yang et al. [6] | Nayar and Ivanovic [7] | Theoharis et al. [8] | Mufti and Molah [9] | Baloch et al. [10] | Stamataki et al. [11] | Wu et al. [12] | Lee et al. [13] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| I | 35.3 | 0 | 8.9 | 10.0 | 10.7 | 9.0 | - | 20.0 | 64.0 | 30.0 | 12.0 | 77.8 |
| II | 5.6 | 4.5 | 11.0 | 0.3 | 0.7 | 2.0 | 9.8 | 3.1 | 11.0 | 6.0 | 8.0 | 0 |
| III | 69.0 | 20.0 | 17.0 | 24.0 | 19.2 | 6.0 | 48.0 | 50.0 | 50.0 | 33.0 | 27.0 | 79.0 |
| IV | 50.0 | 30.6 | 25.4 | 28.0 | 32.2 | 14.0 | 34.0 | 20.0 | 63.0 | 67.0 | 33.0 | 61.5 |
| V | 98.7 | 75.0 | 70.0 | 60.0 | 64.8 | 53.0 | 87.0 | 80.0 | 71.0 | - | 68.0 | 97.6 |
| VI | 98.9 | 97.8 | 98.1 | 97.0 | 98.4 | 97.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 |
BN, benign; PTC, papillary carcinoma; MTC, medullary carcinoma; FC, follicular carcinoma; PD, poorly differentiated carcinoma.
M, case number of malignancy; T, total case number.

